What Is the A-Spot? A Complete Guide to Finding and Stimulating It

Key points
- Curved Toys: G-spot vibrators or dildos with a pronounced curve are perfect for reaching the A-spot. Look for toys with a firm yet flexible tip and a flared base for safety. Graduated or slimmer designs are often easier for beginners to maneuver. Ergonomic curves should align with the natural anterior-posterior axis of the vagina, allowing the tip to rest comfortably against the anterior fornix without requiring awkward wrist angles.
- Wands: Non-vibrating wands, like the popular njoy Pure Wand, are made of steel and have a curved end designed for precise internal massage. The weight and temperature retention of stainless steel can enhance proprioceptive feedback and provide consistent, targeted pressure without requiring excessive muscle effort. Steel also adapts to body temperature, which can be deeply soothing for individuals experiencing vaginal tension or stress-related arousal difficulties.
While the G-spot has long been a focal point in conversations about female pleasure, there's another, deeper erogenous zone that offers a different path to arousal and orgasm: the A-spot. Less known but potentially just as powerful, understanding the A-spot can unlock new dimensions of sexual satisfaction, particularly for those who experience vaginal dryness or seek a different kind of orgasmic experience. From a physiological standpoint, this region is intimately connected to the autonomic nervous system, which governs involuntary responses like natural lubrication, pelvic floor relaxation, and vascular engorgement. By shifting focus away from performance-oriented goals and toward mindful exploration, individuals can cultivate a deeper, more sustainable connection to their sexual wellness.
Historically, sexual anatomy has been mapped with a heavy emphasis on external structures and superficial landmarks. However, modern urogynecology and sexual medicine increasingly recognize the vagina as a dynamic, responsive ecosystem rather than a passive canal. The anterior vaginal wall, in particular, houses a complex matrix of connective tissue, vascular networks, and neural pathways that interact synergistically during arousal. When individuals approach deep-zone exploration with anatomical literacy and physiological awareness, they often report not only enhanced physical pleasure but also improved emotional intimacy, reduced sexual anxiety, and a more holistic understanding of their bodily responses.
This guide synthesizes expert knowledge and clinical research to provide a comprehensive look at what the A-spot is, how it differs from the G-spot, and how you can explore it for yourself. Whether you are navigating changes in sexual function, looking to enhance partnered intimacy, or simply curious about your own anatomy, approaching this topic with patience and anatomical awareness can lead to profoundly rewarding experiences. Sexual wellness is inherently individual, and understanding your unique neurovascular landscape is the first step toward cultivating a safe, satisfying, and evidence-based sexual practice.
What Is the A-Spot? Unveiling the Anterior Fornix Erogenous Zone
The A-spot is the common term for the Anterior Fornix Erogenous Zone (AFE). It's a highly sensitive area of tissue located deep inside the vagina, on the front wall (the side closest to your belly button), between the bladder and the cervix. Anatomically, the anterior fornix is a shallow recess or "pocket" formed where the vaginal vault meets the cervix. Unlike the more superficial vaginal canal, this region is rich in autonomic nerve fibers and highly vascularized tissue, which plays a crucial role in sexual arousal. The vaginal wall itself is stratified squamous epithelium, but the underlying lamina propria contains an extensive network of blood vessels, lymphatic channels, and nerve plexuses that become engorged and sensitized during sexual stimulation.
This zone was first identified in a 1997 study by researcher Dr. Chua Chee Ann, who found that stimulating this area for 10-15 minutes helped women with orgasmic difficulties and vaginal dryness. His research showed that A-spot stimulation could rapidly increase natural lubrication and arousal, making intercourse more comfortable and pleasurable. The physiological mechanism behind this phenomenon involves the activation of the pelvic splanchnic nerves (S2-S4), which trigger parasympathetic responses. When these nerves are gently stimulated, blood flow to the vaginal walls increases dramatically, prompting the Bartholin's glands and vaginal transudate to produce moisture at an accelerated rate. This makes the A-spot particularly relevant for individuals experiencing arousal disorders, menopausal vaginal dryness, or discomfort during penetration. The surge in transudate is a direct result of capillary filtration through the vaginal epithelium, a process that relies heavily on adequate vascular tone and hormonal balance.
Furthermore, the anterior fornix shares anatomical proximity with the cervix and the lower uterine segment, meaning stimulation here can sometimes produce unique referred sensations throughout the pelvic cavity. Because this area is not heavily innervated by the somatic nervous system (which processes sharp, localized touch), the sensations tend to feel diffuse, warm, and deeply grounding rather than sharply localized. Understanding this nerve distribution helps set realistic expectations and encourages a slower, more mindful approach to exploration. The pelvic splanchnic nerves also interface with the enteric nervous system and the vagus nerve, which explains why some individuals report feelings of emotional release, full-body warmth, or even altered states of consciousness during prolonged, gentle A-zone stimulation. This neurobiological cross-talk highlights why the experience is often described as more "visceral" than "cutaneous."
From a clinical perspective, it is essential to recognize that the anterior fornix is not a static structure. Its depth, accessibility, and sensitivity fluctuate throughout the menstrual cycle, during different phases of sexual arousal, and across life stages such as postpartum recovery and perimenopause. The cervix itself undergoes positional changes: during ovulation, it softens, elevates, and opens slightly, while in the luteal phase it descends and firms. These cyclical variations directly impact how the anterior fornix is positioned and how it responds to touch. Tracking these physiological shifts alongside exploration can help individuals identify optimal timing for deeper stimulation and reduce frustration during periods of natural decreased sensitivity.
The A-Spot vs. The G-Spot: Key Differences
While both spots are located on the front vaginal wall, they are distinct in location, sensation, and function. Understanding these differences can help you target them more effectively. From a neurophysiological perspective, the G-spot is primarily connected to the pudendal nerve and the internal clitoral network (including the clitoral bulbs and crura), whereas the A-spot engages deeper pelvic autonomic pathways. This neurological divergence explains why stimulation in one area can feel entirely different from the other, and why some individuals may respond strongly to one while feeling neutral toward the other. The pudendal nerve carries somatic sensory information, which is why G-spot stimulation often feels sharp, precise, and highly localized. In contrast, the pelvic splanchnic nerves are parasympathetic, meaning their activation promotes rest, digestion, and arousal, resulting in a broader, more systemic response.
| Feature | A-Spot (Anterior Fornix) | G-Spot (Gräfenberg Spot) |
|---|---|---|
| Location | Deep in the vagina, about 4-6 inches in, near the cervix. | Closer to the vaginal opening, about 1-2 inches in. |
| Texture | Generally smooth, no distinct texture. | Often described as spongy, ridged, or like the texture of a walnut. |
| Sensation | A deep, diffuse, "full-body" pleasure. Less intense but can feel more encompassing. | An intense, localized, and sometimes sharp pleasure. |
| Stimulation | Responds best to deep, consistent pressure with a gentle, stroking, or circular motion. | Responds well to firm, direct pressure in a "come-hither" motion. |
| Primary Effect | Rapid and significant increase in vaginal lubrication. | Can trigger swelling and, for some, female ejaculation (squirting). |
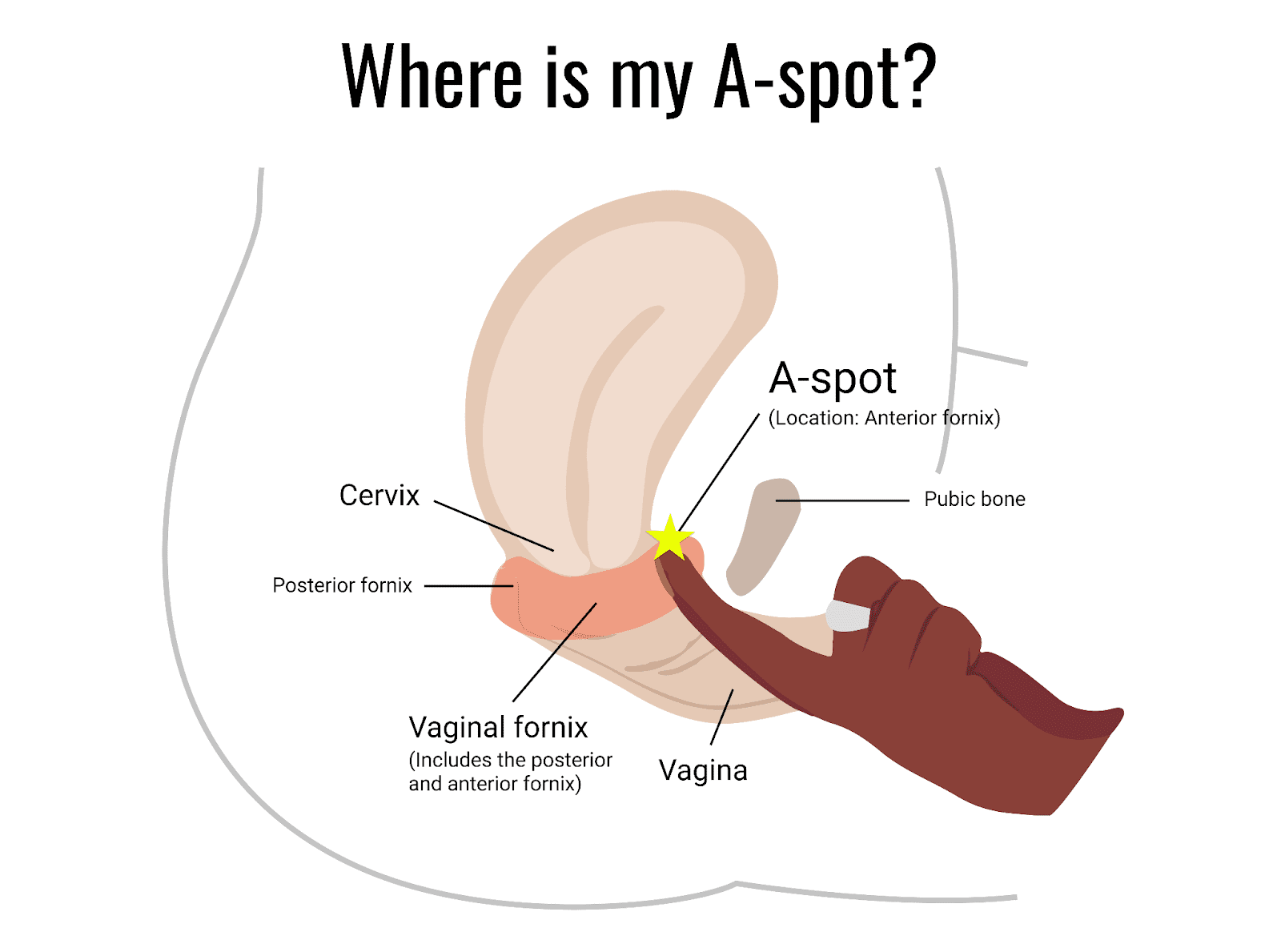 Image Source: The Fornix by Flex
Image Source: The Fornix by Flex
The distinction also extends to hormonal influences. Research indicates that estrogen plays a significant role in maintaining tissue elasticity and sensitivity in both zones. During perimenopause or menopause, declining estrogen levels can thin vaginal tissues and reduce natural sensitivity, which may make A-spot exploration more challenging or occasionally uncomfortable. In such cases, incorporating medical-grade vaginal moisturizers or consulting a healthcare provider about localized estrogen therapy can restore tissue health and make deep-zone exploration more comfortable. Estrogen receptors are densely concentrated in the vaginal epithelium, and their downregulation leads to decreased glycogen content, altered vaginal microbiome pH, and reduced vascular responsiveness. Proactive management of these changes ensures that anatomical exploration remains safe and pleasurable.
Additionally, pelvic floor muscle tone heavily influences accessibility. Individuals with a hypertonic (overly tight) pelvic floor may experience pain or a sensation of "hitting a wall" before reaching the anterior fornix, highlighting the importance of addressing muscular health alongside erogenous zone exploration. The levator ani complex, particularly the pubococcygeus muscle, can involuntarily contract during anxiety or anticipation of pain, effectively shortening the vaginal canal and blocking access to deeper structures. Conversely, a well-conditioned, relaxed pelvic floor with good proprioceptive awareness allows for comfortable deep penetration and enhances the transmission of tactile signals from the anterior fornix to the central nervous system. Pelvic floor rehabilitation, diaphragmatic breathing, and progressive desensitization techniques are often recommended by specialists before attempting deep-zone stimulation in individuals with baseline pelvic tension or dyspareunia.
How to Find the A-Spot: A Step-by-Step Guide
Finding the A-spot requires arousal, patience, and a bit of exploration. When you're aroused, the vagina elongates and becomes more sensitive, making the process easier and more pleasurable. This physiological process, known as vaginal tenting and ballooning, occurs during the plateau phase of arousal. The uterus lifts upward, the vaginal canal lengthens, and the anterior fornix naturally expands, making the A-spot more accessible. Rushing this process or attempting exploration without adequate arousal often leads to cervical sensitivity, which can cause discomfort rather than pleasure. Therefore, prioritizing extended foreplay, mental relaxation, and intentional breathing is medically sound and practically essential. The brain's limbic system must first downregulate sympathetic "fight-or-flight" signaling before parasympathetic "rest-and-digest" pathways can facilitate full genital engorgement.
Understanding lubricant selection is equally critical when exploring deeper anatomical zones. Water-based lubricants are generally compatible with all toy materials and condoms, but their osmolality matters. Hyperosmolar lubricants can draw fluid out of vaginal epithelial cells, causing micro-drying, irritation, or increased infection risk over time. Opting for iso-osmolar or slightly hypo-osmolar formulations protects mucosal integrity. Silicone-based lubricants offer longer-lasting glide and are excellent for extended sessions or water-based play, though they degrade silicone toys unless fully covered with a compatible sleeve or used with glass/metal devices. Hybrid lubricants can bridge these gaps, but patch testing is recommended to rule out individual sensitivities to preservatives like parabens or glycerin, which can alter vaginal flora and trigger candidiasis in susceptible individuals.
Solo Exploration with Fingers
- Get Comfortable and Aroused: Start with what you know feels good. Clitoral stimulation is a great way to begin. Allow at least 10-20 minutes of gradual arousal to let the natural physiological changes occur. Engage diaphragmatic breathing to lower cortisol levels and encourage pelvic floor relaxation, which naturally opens the vaginal canal. Place a hand on your lower abdomen and visualize warmth spreading downward; this mindful grounding technique enhances mind-body connection and reduces anticipatory tension.
- Use Lubricant: Apply a generous amount of water-based lubricant to your fingers to ensure comfortable entry. Even if natural lubrication increases during arousal, adding a high-quality, osmolality-balanced lubricant reduces friction and protects delicate mucosal tissues from micro-abrasions. Reapply as needed; drying lubricant can increase shear force and cause epithelial irritation.
- Find the G-Spot First: Gently insert one or two fingers into your vagina, palm facing up. About one to two inches in, curl your fingers in a "come-hither" motion. You may feel a spongy or textured area—this is likely your G-spot. Pausing here to allow your body to adjust to internal touch helps build confidence and reduces reflexive pelvic floor clenching. Focus on rhythmic, predictable pressure rather than erratic movements to allow sensory adaptation.
- Go Deeper: From the G-spot, continue to slide your fingers deeper into your vagina, maintaining contact with the front wall. You'll need to go another two to four inches deeper. The A-spot is located in the deep pouch just before you reach the cervix. If your fingers brush against a firm, rounded structure resembling the tip of your nose, you have reached the cervix. The A-spot lies in the shallow dip directly anterior to it. Note that cervical position varies; if it feels high and soft, you are closer to ovulation. If it feels low and firm, the fornix may be shallower.
- Explore the Sensation: Once you reach this deep area, instead of a "come-hither" motion, try a gentle side-to-side "windshield wiper" motion or apply steady, circular pressure. Pay attention to the sensations. Many report a feeling of deep pleasure and a noticeable increase in wetness. If you encounter sharp pain or a cramping sensation, stop, add more lubricant, and ease off pressure. The anterior fornix contains sensitive nerve plexuses that can sometimes trigger referred uterine sensations if pressed too aggressively. Maintain light, consistent contact rather than deep thrusting; sustained pressure is key to activating the parasympathetic lubrication reflex.
Using Sex Toys for Deeper Access
Because the A-spot is so deep, fingers may not be long enough for everyone. A sex toy can be an excellent tool for exploration. When selecting a device, prioritize body-safe, non-porous materials such as medical-grade silicone, borosilicate glass, or stainless steel. These materials can be fully sterilized and are less likely to harbor bacteria or cause micro-tears compared to porous materials like "jelly" rubber or TPE. Porous materials degrade over time, trapping bacteria, fungi, and biofilm that standard washing cannot remove. For long-term pelvic health, investing in certified, phthalate-free devices is non-negotiable.
- Curved Toys: G-spot vibrators or dildos with a pronounced curve are perfect for reaching the A-spot. Look for toys with a firm yet flexible tip and a flared base for safety. Graduated or slimmer designs are often easier for beginners to maneuver. Ergonomic curves should align with the natural anterior-posterior axis of the vagina, allowing the tip to rest comfortably against the anterior fornix without requiring awkward wrist angles.
- Wands: Non-vibrating wands, like the popular njoy Pure Wand, are made of steel and have a curved end designed for precise internal massage. The weight and temperature retention of stainless steel can enhance proprioceptive feedback and provide consistent, targeted pressure without requiring excessive muscle effort. Steel also adapts to body temperature, which can be deeply soothing for individuals experiencing vaginal tension or stress-related arousal difficulties.
When using any internal device, always start on the lowest vibration or speed setting. High-intensity vibrations applied directly to the anterior fornix too quickly can overwhelm nerve endings and cause temporary desensitization. Incorporate a small amount of compatible lubricant even with silicone toys to maintain glide, and always clean devices according to manufacturer guidelines to prevent bacterial imbalances or yeast infections. Post-use hygiene should involve warm water, mild fragrance-free soap, and thorough drying. For glass and steel, boiling for 10 minutes or using a 10% bleach solution (followed by thorough rinsing) provides medical-grade sterilization. Storing toys separately in breathable cloth bags prevents cross-contamination and material degradation.
Techniques and Positions for A-Spot Stimulation
To stimulate the A-spot during partnered sex, choose positions that allow for deep, angled penetration targeting the front vaginal wall. The angle of penetration is far more critical than depth alone; a straight, piston-like motion often bypasses the anterior wall and may impact the posterior fornix or cervix uncomfortably. Instead, positioning that tilts the pelvis upward or allows for controlled angling will maximize contact with the anterior fornix while minimizing cervical collision. Understanding basic pelvic biomechanics—how hip flexion, spinal extension, and pelvic tilt alter vaginal orientation—can transform frustrating exploration into precise, pleasurable stimulation. Communication about angle adjustments, pacing, and feedback loops is essential, as anatomical variations between partners dictate optimal mechanics.
Best Sex Positions
- Lifted Missionary: In the missionary position, place pillows or a sex ramp under your hips. This tilts your pelvis upwards, shortening the vaginal canal and creating a better angle for your partner to reach the A-spot. Pulling your knees toward your chest further enhances this angle. Partners should focus on shallow-to-deep thrusting rhythms rather than rapid, full-length penetration, allowing time for nerve endings to register sustained pressure. The elevated pelvis aligns the anterior vaginal wall more directly with the penetrating object, reducing friction on less sensitive posterior tissues.
- Doggy Style: This position naturally allows for deep penetration. To better target the A-spot, the receiving partner can arch their back slightly while the penetrating partner aims their penis or toy slightly upward. Modifying this by keeping the torso lowered and hips elevated shifts the angle toward the anterior wall, increasing the likelihood of consistent contact. Using a firm pillow under the receiving partner's lower abdomen can stabilize the pelvis and prevent overextension of the lumbar spine, making the position more sustainable for extended sessions.
- Cow / On-Top Positions: Positions where the receiving partner is on top provide maximum control over the depth and angle. By leaning back, you can encourage deeper penetration that stimulates the anterior fornix. This position also allows the receiving partner to grind in circular motions, which can provide the sustained, broad pressure the A-spot responds to best, rather than rapid friction. Rocking forward and back while maintaining base contact allows for micro-adjustments in real-time, optimizing stimulation without relying on partner coordination.
- Side-Lying Spoon with Leg Adjustment: Lying on your side with your partner behind you reduces the risk of overly aggressive penetration while still allowing deep access. Raising your top leg onto a pillow or wrapping it around your partner’s hip alters the pelvic tilt, aligning the vaginal canal for anterior wall contact. This is an excellent low-impact option for individuals with pelvic or lower back discomfort. The spoon position also facilitates intimate physical contact, which releases oxytocin and enhances emotional safety, a known catalyst for deeper physiological arousal.
Regardless of position, communication and pacing remain paramount. The A-spot does not respond to rapid, intermittent stimulation as effectively as the clitoris or G-spot. Sustained, rhythmic contact for at least 10-15 minutes is typically required to trigger the full autonomic response, including the characteristic surge in natural lubrication and deep pelvic warmth. Partners should establish verbal or non-verbal feedback signals to indicate comfort, pleasure, or the need to adjust pressure. Using a scale (1-10) for both sensation intensity and comfort level helps demystify internal experiences and reduces the guesswork often present in partnered exploration. Remember that arousal is cumulative; skipping the initial phases of tactile, emotional, and neurological priming often results in diminished sensitivity regardless of mechanical precision.
The Scientific Debate: Does the A-Spot Really Exist?
It's important to note that, much like the G-spot, the existence of the A-spot as a distinct anatomical structure is a topic of scientific debate. There is no single, universally identified "spot." Histological studies have not consistently identified a unique glandular or nerve bundle exclusive to the anterior fornix, leading some researchers to classify the A-spot as a functional erogenous zone rather than a discrete organ. However, the absence of a standalone anatomical landmark does not invalidate the subjective experiences reported by countless individuals. Modern sexual medicine has largely moved away from the "spot" paradigm toward a "network" model, recognizing that pleasure arises from integrated tissue systems rather than isolated pressure points.
Many sexologists, including Dr. Jennifer Gunsaullus, suggest it's more helpful to think of it as an "A-zone"—an area with a higher concentration of nerve endings that is particularly sensitive to stimulation. Some researchers theorize that the pleasure from A-spot and G-spot stimulation comes from indirectly stimulating the vast internal network of the clitoris through the vaginal wall. Advanced imaging studies, particularly 3D ultrasounds and fMRI scans, have revealed that the clitoris is not merely an external pea-sized structure, but a complex, wishbone-shaped organ with bulbs and crura that extend several centimeters internally along the anterior vaginal wall. When the anterior fornix is compressed or massaged, it likely transmits mechanical pressure through this extensive clitoral network, triggering orgasmic pathways. This interconnected architecture explains why some individuals experience blended orgasms when both external and deep internal structures are stimulated synchronously.
Furthermore, functional MRI studies have shown that different erogenous zones activate overlapping but distinct cortical regions during sexual arousal. Stimulation of the anterior vaginal wall consistently activates the insula, anterior cingulate cortex, and somatosensory areas responsible for interoception and emotional processing. This neurological mapping supports the idea that the A-spot is less about precise anatomical geography and more about neurovascular responsiveness. Tissue health, hydration, blood flow, and psychological safety modulate how signals from this region are processed. Stress, anxiety, or negative body image can suppress pelvic blood flow and dampen nerve signaling, while relaxation, trust, and positive expectation can amplify it through top-down cortical modulation.
Ultimately, whether it's a "spot" or a "zone" is less important than the fact that for many people, this area is a source of immense pleasure. Sexual medicine increasingly embraces a functional, experience-based model of anatomy. Rather than hunting for rigid anatomical proof, clinicians and researchers focus on how neural plasticity, pelvic health, and mindful awareness contribute to sexual satisfaction. Individual variation in pelvic anatomy, nerve distribution, and psychological conditioning means that some individuals will experience profound pleasure from anterior fornix stimulation, while others may find it neutral or even uncomfortable. Both responses are physiologically normal. Validating subjective experience over rigid anatomical dogma empowers individuals to explore without performance pressure, fostering a healthier, more sustainable relationship with their bodies.
Expert Insights and Tips for Exploration
- Communication is Key: Talk with your partner about what you're feeling. Guide their hand, penis, or toy to where it feels best. Use clear, anatomical language or descriptive cues ("deeper," "more pressure toward my belly button," "slower circles") to bridge the gap between internal sensation and external action. Establish a non-judgmental space where feedback is welcomed, not interpreted as criticism. Regular check-ins during and after exploration help recalibrate techniques to match evolving comfort levels and preferences.
- Don't Hunt for a Button: As sex educator Alicia Sinclair notes, "Everyone’s ‘money spot’ is different." The goal is to explore what feels good for your unique body, not to find a mythical magic button. Shifting from a goal-oriented mindset to a process-oriented one reduces performance anxiety, which is a known inhibitor of parasympathetic arousal and natural lubrication. Pleasure exists in the journey of discovery, not just the destination. Celebrating small milestones of increased awareness or comfort builds long-term sexual confidence.
- Combine with Clitoral Play: The majority of people with vulvas require clitoral stimulation to orgasm. Combining deep A-spot pressure with external clitoral touch can create a powerful, blended orgasm. This dual-pathway stimulation engages both somatic (pudendal) and autonomic (pelvic splanchnic) nerves, potentially leading to longer-lasting, full-body orgasmic waves. Experiment with different combinations: gentle vibration externally paired with deep circular pressure internally, or synchronized rhythmic contact that mirrors natural pelvic contractions. Finding your unique synergy may require trial, but the neurological payoff is often profound.
- Pelvic Floor Awareness: Chronic stress, sedentary lifestyles, or past trauma can lead to pelvic floor dysfunction. If you experience pain during deep penetration, consider consulting a pelvic floor physical therapist. They can assess for muscle hypertonicity, trigger points, or fascial restrictions that may be blocking access to deeper erogenous zones and provide targeted rehabilitation exercises. Biofeedback training, myofascial release, and progressive desensitization protocols can restore optimal muscle tone and improve proprioceptive mapping of internal structures, making exploration safer and more rewarding.
- Post-Stimulation Care: After extended deep-zone exploration, the vaginal and cervical tissues may feel highly sensitive or emotionally vulnerable. This is a normal neurochemical response involving dopamine, oxytocin, and prolactin fluctuations. Hydrating, gentle stretching, and using a mild, pH-balanced cleanser externally can help restore comfort. Some individuals experience a "post-orgasmic refractory period" characterized by temporary emotional sensitivity or fatigue; this is a healthy regulatory response. Allow time for nervous system integration, engage in gentle grounding practices, and avoid immediately jumping into high-intensity activities or harsh soaps that disrupt the vaginal microbiome.
- Cycle Syncing and Hormonal Awareness: Track your menstrual cycle alongside exploration to identify peak sensitivity windows. During the follicular and ovulatory phases, rising estrogen thickens vaginal epithelium, increases transudate production, and elevates libido. The luteal phase, dominated by progesterone, often brings decreased sensitivity and natural dryness. Aligning exploration with your hormonal baseline reduces friction, enhances comfort, and improves success rates. Apps or simple journaling can help you map physiological patterns over several cycles, revealing personalized optimal timing for deeper exploration.
Exploration of the A-spot is a journey of self-discovery. It offers a wonderful opportunity to learn more about your body, communicate your desires, and add a new and exciting dimension to your sexual pleasure. By integrating anatomical knowledge, physiological awareness, and open communication, you can cultivate a sexual practice that prioritizes wellness, safety, and authentic satisfaction. Sexual health is a lifelong continuum; remaining curious, patient, and informed ensures that your practices evolve alongside your body's changing needs. Whether you experience profound pleasure, subtle warmth, or simply enjoy the process of mindful exploration, your experience is valid and medically supported.
Frequently Asked Questions
Can stimulating the A-spot help with vaginal dryness during menopause?
Yes, A-spot stimulation has been clinically observed to trigger a rapid increase in vaginal lubrication, even in postmenopausal individuals. The parasympathetic nervous system response to sustained anterior fornix pressure increases blood flow to the vaginal walls, encouraging transudation of fluid through the epithelium. However, because estrogen decline thins vaginal tissues over time, many individuals still benefit from using a high-quality lubricant, vaginal moisturizers, or discussing localized estrogen therapy with a gynecologist to ensure optimal tissue health and comfort. Combining mechanical stimulation with hormonal support and proper lubrication creates a comprehensive approach to managing menopausal dryness safely.
Is it normal to experience cramping or an urge to urinate when exploring the A-spot?
Yes, this is a common and typically harmless physiological response. The A-spot lies directly against the base of the bladder and shares nerve pathways with the lower urinary tract. Deep pressure here can stimulate stretch receptors, creating a temporary sensation similar to needing to urinate or mild menstrual cramping. Emptying your bladder before exploration and adjusting pressure or angle usually alleviates this sensation. If sharp, persistent pain occurs, reduce intensity or discontinue and consult a healthcare provider to rule out pelvic inflammatory conditions or endometriosis. Gradual acclimation and mindful breathing often help the nervous system differentiate between harmless fullness signals and true discomfort.
How long does it typically take to feel pleasure or notice lubrication from A-spot stimulation?
Research and clinical observations suggest that consistent, focused stimulation for 10 to 15 minutes is usually required to fully engage the autonomic response. Unlike the clitoris, which can respond rapidly to direct friction, the A-spot thrives on sustained, rhythmic pressure that allows vascular engorgement and nerve signaling to build. Patience and extended arousal time significantly improve the likelihood of experiencing the characteristic warmth, deep pleasure, and natural lubrication associated with this zone. Rushing the process interrupts the neurovascular cascade, so maintaining steady, gentle contact and tracking subtle physiological shifts yields better results over time.
Are there any medical conditions that make A-spot exploration unsafe?
While generally safe for healthy individuals, certain conditions warrant caution or medical consultation before deep internal exploration. Active pelvic infections, unexplained vaginal bleeding, severe pelvic organ prolapse, untreated vaginismus, recent pelvic surgery, or advanced endometriosis can make deep penetration painful or medically inadvisable. Always listen to your body’s feedback; pain is a protective neurological signal, not a barrier to push through. If you have underlying pelvic health concerns, consult a urogynecologist or pelvic floor specialist first. They can provide imaging, functional assessments, and tailored clearance guidelines to ensure your exploration aligns with your overall medical health.
Does the A-spot have any connection to fertility or menstrual cycle changes?
The anterior fornix is primarily a sexual response zone and does not play a direct role in conception or fertility. However, cervical position and vaginal moisture naturally fluctuate throughout the menstrual cycle due to hormonal shifts in estrogen and progesterone. During ovulation, elevated estrogen increases cervical mucus production and vaginal lubrication, which can make the A-spot more accessible and sensitive. During the luteal phase, progesterone dominance may reduce natural wetness and make tissues feel firmer or less responsive. Tracking your cycle alongside exploration can help you identify when your body is most receptive to deeper stimulation. Hormonal contraceptives may alter these natural fluctuations, so adjusting expectations and lubrication use accordingly is recommended.
Conclusion
The A-spot, or anterior fornix erogenous zone, represents a fascinating intersection of neuroanatomy, vascular physiology, and sexual wellness. While it may not possess the distinct anatomical boundaries of more superficial erogenous zones, its functional impact on arousal, natural lubrication, and deep pelvic pleasure is well-documented both clinically and anecdotally. By understanding its location, recognizing how it differs from the G-spot, and approaching exploration with patience, proper lubrication, and mindful technique, individuals can safely tap into this often-overlooked pathway to sexual satisfaction. The integration of pelvic splanchnic nerve activation, clitoral network stimulation, and parasympathetic dominance creates a unique physiological state that many describe as deeply restorative and profoundly pleasurable.
Key takeaways for successful A-spot exploration include prioritizing extended arousal to trigger vaginal tenting, using appropriate toys or finger techniques that favor sustained circular or side-to-side pressure over rapid friction, and maintaining open communication with partners. It is equally important to normalize individual variation; not every person will respond to anterior fornix stimulation in the same way, and that is entirely consistent with the diverse nature of human sexual response. When combined with clitoral stimulation, pelvic floor awareness, cycle tracking, and a focus on holistic sexual health, A-spot exploration can become a valuable tool for enhancing intimacy, addressing arousal-related dryness, and deepening bodily autonomy.
Safety remains the cornerstone of any intimate exploration practice. Using body-safe materials, respecting physiological feedback loops, avoiding forceful penetration, and seeking professional guidance when pain or dysfunction arise ensures that the journey remains empowering rather than harmful. Sexual wellness is an ongoing practice of listening, learning, and adapting. Whether you are navigating changes in hormonal health, seeking new dimensions of partnered intimacy, or simply expanding your understanding of your own anatomy, approaching the A-spot with curiosity, medical literacy, and respect yields the most rewarding results. As sexual medicine continues to evolve, the integration of evidence-based guidance, trauma-informed practices, and personalized exploration will remain the foundation of fulfilling, healthy, and sustainable sexual experiences.
References
- Medical News Today. "A-spot: Definition, how to find it, and stimulation."
- Healthline. "A-Spot: 10 FAQs on What It Is, How to Find It, Positions to Try, More."
- Chua, C. A. (1997). "A new method of relieving female sexual dysfunction." Sexual and Marital Therapy, 12(4), 359-363.
- Well+Good. "What Is the A-Spot? Access Deeper Pleasure with This Little-Known Erogenous Zone."

About the author
Sofia Rossi, MD, is a board-certified obstetrician-gynecologist with over 15 years of experience in high-risk pregnancies and reproductive health. She is a clinical professor at a top New York medical school and an attending physician at a university hospital.