Knot on the Back of Your Heel: Causes, Treatment, and Prevention
Key points
- A bony prominence: An enlargement of the heel bone, such as a heel spur or Haglund's deformity.
- An inflamed bursa: Swelling of the small, fluid-filled sac (bursa) that cushions the tendon and bone, a condition known as bursitis.
- A damaged tendon: Thickening or scar tissue on the Achilles tendon due to overuse, known as Achilles tendonitis or tendinosis.
- Other rare causes: In uncommon cases, the lump could be a fatty deposit (xanthoma) related to high cholesterol or a benign soft tissue tumor.
A painful, hard knot on the back of your heel is a common complaint that can interfere with daily activities and exercise. Often noticed after wearing new shoes or increasing physical activity, this lump can be caused by several underlying conditions, from a bony growth to an inflamed tendon.
Understanding the cause of the knot is the first step toward finding relief. This guide covers the most common causes, such as Haglund's deformity and Achilles tendonitis, their symptoms, and a full range of treatment options, from simple home care to medical procedures.
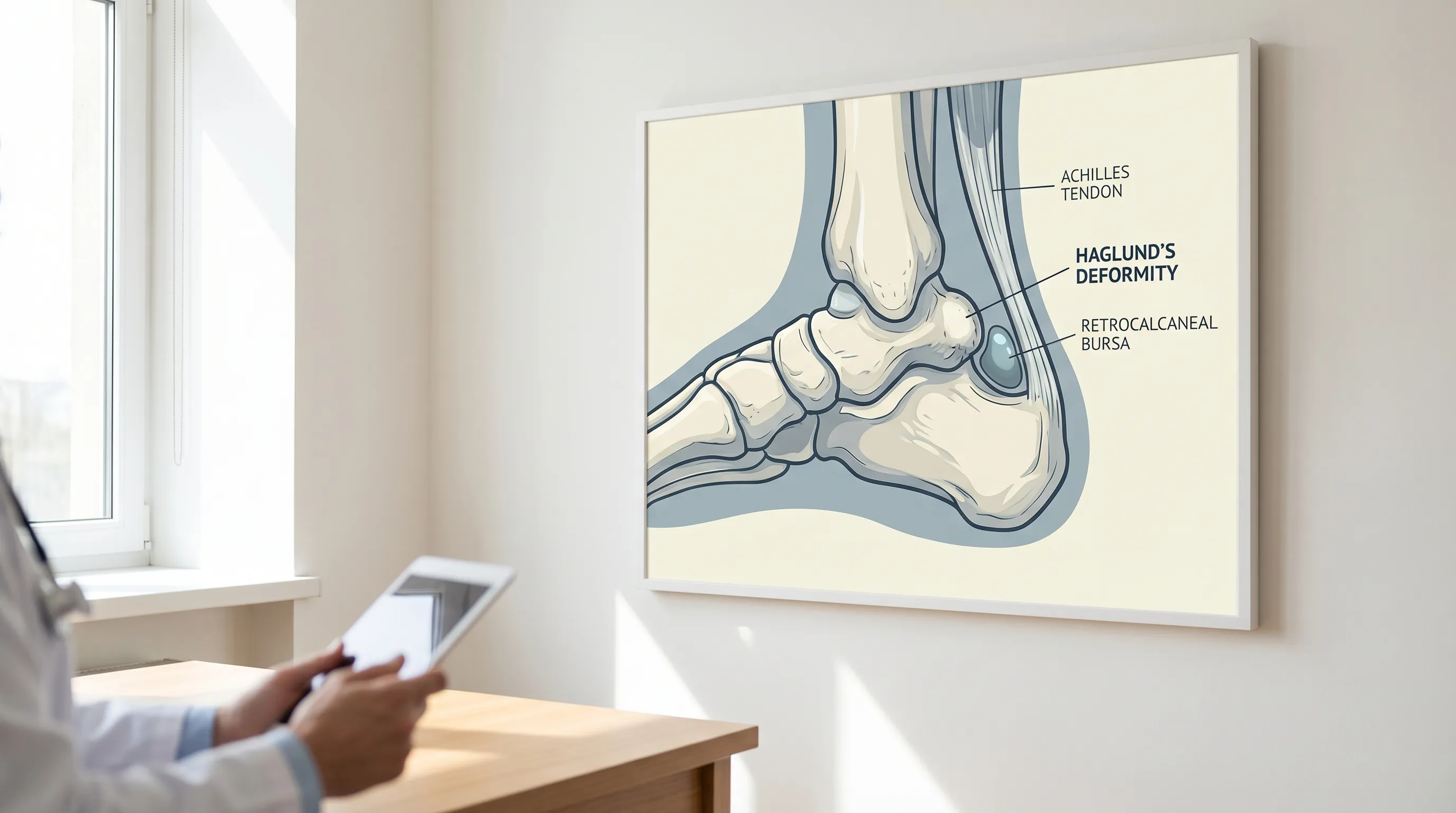 Image: The bony enlargement of Haglund's deformity can irritate the nearby Achilles tendon and bursa. (Image source: Lifespan Health System)
Image: The bony enlargement of Haglund's deformity can irritate the nearby Achilles tendon and bursa. (Image source: Lifespan Health System)
The heel complex is an anatomical marvel, bearing up to 1.5 times your body weight during walking and nearly five times your body weight during running. The posterior calcaneus serves as the primary attachment point for the Achilles tendon, the strongest and thickest tendon in the human body. When repetitive microtrauma, structural anomalies, or improper footwear disrupt the delicate balance of load distribution in this area, the body's natural healing response can lead to localized thickening, calcification, or fluid accumulation. This physiological reaction manifests clinically as a palpable knot, which may be purely structural, inflammatory, or degenerative in nature. Recognizing the nuanced differences between these presentations is essential for targeted intervention and long-term resolution.
What Is a Knot on the Back of the Heel?
A "knot on the back of the heel" is a non-medical term for any lump, bump, or swelling where the Achilles tendon attaches to the heel bone (calcaneus). This knot can feel hard like bone or soft and tender, and it often becomes painful when it rubs against footwear.
This bump is typically the result of structural changes or inflammation involving the heel bone or surrounding soft tissues. The most likely culprits include:
- A bony prominence: An enlargement of the heel bone, such as a heel spur or Haglund's deformity.
- An inflamed bursa: Swelling of the small, fluid-filled sac (bursa) that cushions the tendon and bone, a condition known as bursitis.
- A damaged tendon: Thickening or scar tissue on the Achilles tendon due to overuse, known as Achilles tendonitis or tendinosis.
- Other rare causes: In uncommon cases, the lump could be a fatty deposit (xanthoma) related to high cholesterol or a benign soft tissue tumor.
Repetitive stress is often the trigger. Constant pressure from shoes can cause the body to build extra bone, while overuse from activities like running can lead to inflammation and thickening of the soft tissues.
From a biomechanical standpoint, the posterior heel operates under significant mechanical stress. During the gait cycle, specifically the stance and push-off phases, the Achilles tendon transmits tremendous tensile forces to the calcaneus. When the subtalar joint pronates excessively or when individuals possess a naturally high-arched (pes cavus) foot structure, the heel can invert excessively, driving the calcaneal prominence directly into the posterior collar of the shoe. This constant friction triggers a cascade of cellular responses: fibroblasts deposit collagen irregularly, chondrocytes may appear in fibrocartilage transition zones, and osteoblasts lay down additional bone matrix as a defensive adaptation. Over time, these microscopic changes coalesce into a macroscopic, palpable mass that disrupts normal biomechanics and creates a pain-inflammation-feedback loop.
Common Causes of a Heel Knot
1. Haglund's Deformity ("Pump Bump")
One of the most frequent causes of a hard knot is Haglund's deformity, a bony enlargement on the back of the heel bone. It's often called a "pump bump" because it was historically associated with wearing rigid-backed pump-style shoes. The constant pressure from such footwear can irritate the area, leading the body to form extra bone.
"We often see Haglund’s deformity in patients who have a tight Achilles tendon or who frequently wear stiff, closed-heel shoes. The rigid back of a shoe can constantly irritate the area, leading to a bony enlargement and inflammation." — Dr. Jane Smith, DPM, Podiatrist.
Key characteristics of Haglund's deformity include:
- A hard, bony bump visible on the back of the heel.
- Pain that worsens when wearing shoes with firm backs.
- A predisposition in individuals with high arches or tight Achilles tendons.
- It is often accompanied by retrocalcaneal bursitis, where the bursa between the bone and tendon becomes inflamed, adding to the pain and swelling.
The pathophysiology of Haglund's deformity extends beyond mere friction. Genetic predisposition plays a documented role, with studies indicating that foot morphology, particularly a prominent superior-lateral calcaneal angle (often exceeding 75 degrees on radiographic evaluation), significantly increases susceptibility. When combined with a cavus foot type, the heel bone naturally sits in a more inverted position, forcing the lateral aspect of the posterior calcaneus into direct contact with shoe counter materials. Additionally, the Achilles tendon itself may have a varus alignment, meaning it doesn't pull straight back on the heel but rather angles inward, concentrating compressive forces on a specific area of the bone. This chronic mechanical irritation stimulates endochondral ossification, gradually forming the characteristic exostosis. In severe, untreated cases, the bony overgrowth can actually begin to erode the anterior surface of the Achilles tendon fibers, leading to chronic insertional tendinopathy and potential partial tearing.
2. Achilles Tendonitis or Tendinosis
If the knot feels like it's part of the tendon itself, located just above the heel bone, it may be Achilles tendonitis (acute inflammation) or tendinosis (chronic degeneration). Overuse from activities like running or jumping can cause microtears in the tendon. As the tendon tries to heal, it can thicken and develop scar tissue, forming a palpable lump.
Signs of an Achilles tendon-related knot include:
- A lump that feels like a thick cord or nodule within the tendon.
- Pain and stiffness, especially in the morning or after periods of rest.
- The swelling may move slightly when you flex your foot up and down.
- The lump may feel firmer or more rubbery than a bony spur.
Modern sports medicine distinguishes sharply between insertional Achilles tendinopathy and midportion Achilles tendinopathy, though both can present with nodular thickening. Insertional tendinopathy occurs within 2 cm of the calcaneal attachment and is frequently associated with Haglund's deformity and bone spur formation. Midportion tendinopathy typically appears 2 to 6 cm above the insertion site and is driven by cumulative mechanical overload that exceeds the tendon's regenerative capacity. In chronic tendinosis, the histological architecture of the tendon changes dramatically: organized, parallel type I collagen fibers become disorganized, neovascularization (the growth of new, pain-generating blood vessels) increases, and the ground substance of the tendon matrix becomes more hydrated and less dense. The "knot" you feel is often a focal area of tendinous thickening where the body has laid down disorganized reparative tissue in response to repetitive tensile stress. Without appropriate load management, this degenerative nodule can become highly symptomatic, leading to compensatory gait alterations that subsequently strain the knees, hips, and lower back.
3. Retrocalcaneal Bursitis
The retrocalcaneal bursa is a fluid-filled sac that provides cushioning between the Achilles tendon and the heel bone. When this bursa becomes inflamed from pressure or overuse, it swells with fluid, causing a soft, tender, and "squishy" knot. This condition is known as retrocalcaneal bursitis.
Bursitis is often a companion to Haglund's deformity—the bony bump irritates the bursa—but it can also occur on its own due to poorly fitting shoes or repetitive ankle movements.
Symptoms include:
- Tenderness when you squeeze the sides of the heel, just in front of the Achilles tendon.
- A soft swelling that may be accompanied by redness or warmth.
- Pain when wearing closed-back shoes.
There are actually two primary bursae in the posterior heel region: the retrocalcaneal bursa (deep to the Achilles tendon, anterior to the calcaneus) and the subcutaneous calcaneal bursa (superficial, lying between the Achilles tendon and the skin). Both can become inflamed, but retrocalcaneal bursitis is far more common and clinically significant. The bursa functions as a mechanical buffer, reducing shear forces during ankle dorsiflexion. When the ankle repeatedly moves into extreme dorsiflexion—such as during uphill running, stair climbing, or aggressive calf stretching—the bursa becomes compressed. This compression restricts local blood flow, leading to tissue hypoxia, cytokine release, and fluid extravasation. The resulting knot is essentially a localized fluid-filled cyst that can significantly limit ankle mobility. Differentiating bursitis from tendon pathology requires specific clinical maneuvers, most notably the "crossed-finger test" or "pinch test," where deep pressure applied medial and lateral to the tendon reproduces the patient's primary pain, isolating the bursa from the tendon itself.
Additional Etiologies to Consider
While the three conditions above account for the vast majority of posterior heel knots, several other medical conditions warrant consideration during differential diagnosis. Insertional Achilles tendinopathy with calcific spurring involves calcium phosphate crystal deposition directly within the tendon fibers at their attachment point, creating a hard, gritty knot that can be seen on lateral radiographs. Gouty tophi represent uric acid crystal deposits that can accumulate around the heel, particularly in patients with poorly controlled hyperuricemia; these lumps are often accompanied by acute, severe inflammatory flares. Tendon xanthomas are lipid deposits that may signal underlying familial hypercholesterolemia or metabolic syndrome. Ganglion cysts originating from the subtalar joint or tendon sheaths can also migrate to the posterior heel, presenting as firm, sometimes transilluminating nodules that fluctuate in size. Finally, in immunocompromised individuals or those with open wounds, localized infection or abscess formation must be ruled out, as these require urgent antimicrobial intervention.
Symptoms of a Heel Knot
While symptoms vary based on the cause, common signs include:
- A visible bump or swelling on the back of the heel.
- Pain that ranges from a dull ache to a sharp pain, often worsened by activity or shoe pressure.
- Tenderness to the touch.
- Stiffness in the Achilles tendon, particularly in the morning.
- Redness or warmth over the bump due to inflammation.
- Difficulty wearing certain shoes, especially those with a hard heel counter.
Symptom patterns often provide crucial diagnostic clues. Morning stiffness lasting more than 30 to 60 minutes strongly suggests chronic tendinosis or an active inflammatory arthropathy, whereas immediate pain upon first steps that quickly improves with light movement is characteristic of acute inflammatory phases. Pain that localizes precisely to the bony prominence and radiates anteriorly when shoes are worn typically indicates mechanical compression from Haglund's deformity or superficial bursitis. Conversely, a knot that produces a deep, burning ache during push-off phases, accompanied by a sensation of weakness or "giving way," raises suspicion for structural tendon degeneration or partial tearing. Systemic symptoms such as unexplained fever, profound fatigue, or bilateral symmetrical swelling should prompt immediate evaluation for rheumatological conditions like ankylosing spondylitis, psoriatic arthritis, or rheumatoid arthritis, which frequently manifest with heel enthesopathy. Additionally, sudden onset of severe posterior heel pain with an audible "pop" or immediate inability to bear weight requires urgent rule-out of a complete Achilles tendon rupture, a medical emergency requiring orthopedic intervention within 72 hours for optimal outcomes.
Diagnosis and When to See a Doctor
If you have a persistent or painful knot, it's best to see a healthcare professional, such as a podiatrist or an orthopedic specialist.
Diagnosis typically involves:
- A medical history to understand your symptoms, activities, and footwear.
- A physical examination to feel the lump, check your ankle's range of motion, and pinpoint the source of pain.
- Imaging tests, if needed. An X-ray can confirm a bony issue like Haglund's deformity, while an ultrasound or MRI can visualize soft tissues like the Achilles tendon and bursa to check for inflammation or damage.
During the clinical evaluation, practitioners will assess foot posture, ankle dorsiflexion range (using the Silfverskiöld test to differentiate gastrocnemius vs. soleus tightness), and gait mechanics. They may measure the Fowler-Philip angle on lateral weight-bearing radiographs; an angle greater than 75 degrees is highly indicative of a prominent Haglund's lesion. Musculoskeletal ultrasound offers dynamic, real-time visualization, allowing clinicians to observe tendon fiber alignment, vascularity via Doppler imaging, and bursa distension during active movement. Magnetic resonance imaging (MRI) remains the gold standard for evaluating bone marrow edema, partial tendon tears, and deep retrocalcaneal pathology, particularly when surgical planning is anticipated. Laboratory testing, including ESR, CRP, rheumatoid factor, or uric acid panels, may be ordered if systemic inflammation or crystal arthropathy is suspected. You should seek immediate medical attention if the knot is accompanied by open wounds, purulent drainage, uncontrollable pain, rapid enlargement, numbness, or if conservative self-care fails to yield improvement after 3 to 4 weeks.
Treatment and Management
The goal of treatment is to reduce pain, relieve pressure, and allow tissues to heal. Most cases respond well to conservative (non-surgical) care.
Non-Surgical Treatments
- Rest and Activity Modification: Avoid high-impact activities like running and jumping. Switch to low-impact options such as swimming or cycling.
- Footwear Changes: Wear open-backed shoes (like clogs) or shoes with a soft, flexible heel counter. Avoid rigid dress shoes and high heels.
- Heel Lifts or Padding: An over-the-counter heel lift can slightly elevate your heel, reducing pressure on the back. Moleskin or gel pads can also cushion the area.
- Ice Therapy: Apply an ice pack for 15-20 minutes several times a day to reduce inflammation and pain.
- Anti-Inflammatory Medication: Over-the-counter NSAIDs like ibuprofen or naproxen can help manage pain and swelling.
- Stretching and Exercises: Gentle stretching of the calf muscles is crucial. A physical therapist can guide you through specific exercises, such as eccentric heel drops, which are highly effective for strengthening and healing the Achilles tendon.
- Physical Therapy: A therapist can use treatments like ultrasound, massage, and taping to accelerate healing and address any biomechanical issues.
- Orthotics: Custom or over-the-counter shoe inserts can help correct foot alignment issues (like high arches or flat feet) that may contribute to the problem.
Advanced conservative management has evolved significantly, offering patients multiple evidence-based interventions before considering invasive procedures. Extracorporeal Shockwave Therapy (ESWT) has emerged as a highly effective modality for chronic tendinopathy and refractory bursitis. Focused acoustic waves stimulate neovascularization, disrupt disorganized scar tissue, and trigger a localized regenerative inflammatory response that resets the tendon's healing cascade. Typically administered in 3 to 5 weekly sessions, ESWT demonstrates success rates exceeding 70% in patients with chronic insertional Achilles pathology.
For persistent inflammatory pain, targeted corticosteroid injections may provide short-to-medium term relief, though they are generally used cautiously near tendons due to documented risks of collagen degradation and potential tendon rupture. Alternatively, platelet-rich plasma (PRP) therapy leverages the patient's own concentrated growth factors to accelerate tissue remodeling, showing promising outcomes in degenerative tendon conditions. Dry needling and ASTYM/Graston technique (instrument-assisted soft tissue mobilization) help break down fibrotic adhesions, improve local circulation, and restore normal tissue pliability. When prescribing orthotics, clinicians often utilize medial heel wedges or custom carbon-fiber foot orthoses with deep heel cups to control excessive subtalar joint motion, effectively offloading the posterior heel structures during weight-bearing activities. Taping techniques, such as Low-Dye strapping or Achilles taping with rigid athletic tape, provide proprioceptive feedback and temporarily correct faulty foot mechanics during the rehabilitation phase.
Surgical Options
Surgery is a last resort, considered only when months of conservative treatment fail to provide relief. Procedures may include:
- Haglund's Deformity Resection: The surgeon removes the bony bump from the heel bone.
- Achilles Tendon Debridement: Unhealthy, degenerated tendon tissue is removed.
- Bursectomy: The inflamed bursa is removed.
Recovery from surgery typically involves a period of immobilization followed by physical therapy and can take several months.
Modern posterior heel surgery has transitioned toward minimally invasive and endoscopic approaches whenever anatomically feasible, reducing wound complications and accelerating rehabilitation timelines. Endoscopic calcaneoplasty utilizes two small portals to visualize and resect the bony prominence and inflamed bursa under direct camera guidance, preserving the Achilles attachment and surrounding soft tissue envelope. In cases with severe tendon degeneration involving more than 50% of the cross-sectional area, surgeons may perform a flexor hallucis longus (FHL) tendon transfer to augment the compromised Achilles and restore push-off strength. Post-operatively, patients are typically placed in a non-weightbearing cast or walking boot for 4 to 8 weeks, followed by a highly structured physical therapy protocol emphasizing early protected range of motion, progressive loading, and eventual return to sport. Complication rates are generally low but can include sural nerve injury, wound dehiscence, deep infection, or persistent stiffness, underscoring the importance of selecting an experienced foot and ankle specialist for surgical management.
Prevention Tips
Once the pain is gone, prevent the knot from returning with these strategies:
- Wear Proper Footwear: Choose shoes that fit well and have soft, supportive heel counters.
- Stretch Regularly: Keep your calf muscles and Achilles tendons flexible with daily stretching.
- Increase Activity Gradually: Avoid sudden increases in exercise intensity or duration. Follow the "10% rule" by not increasing your mileage by more than 10% per week.
- Strengthen Your Calves: Strong calf muscles better absorb stress.
- Maintain a Healthy Weight: Less weight means less strain on your feet and tendons.
- Listen to Your Body: Address minor aches and stiffness early with rest and ice before they become a major problem.
Prevention extends beyond basic footwear and stretching. Biomechanical screening every 6 to 12 months can identify developing gait asymmetries before they cause tissue damage. Incorporate eccentric calf strengthening as a permanent fixture in your training regimen; the Alfredson protocol (3 sets of 15 reps on both straight and bent knee, twice daily) remains the most validated exercise for building tendon tensile capacity and resisting future overload. Pay meticulous attention to shoe rotation and lifespan: running shoes should be replaced every 300 to 500 miles as midsole compression alters load distribution, forcing the Achilles and heel into compensatory, high-stress positions. Cross-training is essential; alternating high-impact days with pool workouts, cycling, or elliptical training provides cardiovascular conditioning while allowing the posterior kinetic chain adequate recovery time.
Nutritional and metabolic factors also play a critical, often overlooked role in heel health. Tendons are composed largely of collagen, requiring adequate dietary protein, vitamin C, zinc, and copper for optimal synthesis and cross-linking. Chronic dehydration reduces tendon viscoelasticity, making the tissue more brittle and susceptible to microtrauma. Managing systemic inflammation through an omega-3 rich diet, limiting refined sugars and alcohol, and addressing metabolic conditions like insulin resistance or hyperlipidemia can significantly improve tissue resilience and reduce the likelihood of degenerative nodular formation. Finally, establish a pre-activity dynamic warm-up routine (5-10 minutes of ankle circles, calf raises, and brisk walking) to increase local tissue temperature, synovial fluid viscosity, and neuromuscular activation, effectively preparing the posterior heel complex for mechanical demands.
Frequently Asked Questions
Can a knot on the back of the heel go away without surgery?
In the majority of cases, yes. Posterior heel knots caused by inflammation, bursitis, or early-stage tendinopathy typically resolve completely with dedicated conservative management over 3 to 6 months. This requires strict adherence to load management, appropriate footwear modification, targeted physical therapy, and consistent stretching. While bony enlargements from Haglund's deformity do not physically "dissolve," the associated pain and inflammation can be successfully managed long-term, allowing patients to resume pain-free function without surgical intervention. Surgery is reserved for cases where structural deformity causes irreversible tissue damage or when exhaustive conservative protocols yield no symptomatic improvement after 6 to 12 months.
How do I know if my heel knot is a tendon issue or a bony spur?
The tactile characteristics and symptom patterns provide reliable initial clues. A bony spur or Haglund's deformity typically presents as a fixed, immovable, rock-hard mass that does not change in size day-to-day. Pain is primarily mechanical, triggered almost exclusively by shoe pressure or direct palpation of the bone. In contrast, a tendon-related knot often feels firm yet slightly compressible or rubbery, may fluctuate in size or firmness depending on activity levels, and commonly exhibits significant morning stiffness. A simple clinical test involves moving your toes up and down while feeling the lump; if the knot moves with tendon excursion, it originates from the Achilles itself. If it remains completely stationary, it is likely bony. A definitive diagnosis always requires imaging (X-ray for bone, ultrasound/MRI for soft tissue).
Are corticosteroid injections safe for treating heel knots?
Corticosteroid injections can provide powerful, rapid relief for retrocalcaneal bursitis or severe acute inflammation, but they carry specific risks when used near the Achilles tendon. Repeated or improperly placed steroid injections into the tendon substance can weaken collagen fibers, disrupt normal tissue architecture, and significantly increase the risk of spontaneous tendon rupture. Most foot and ankle specialists reserve corticosteroids for strictly extra-tendinous, bursa-focused injections under ultrasound guidance, typically limiting administration to one or two doses. Alternative injectables like platelet-rich plasma (PRP) or hyaluronic acid are increasingly preferred for tendon pathology due to their regenerative properties and superior safety profiles. Always discuss the risk-benefit ratio thoroughly with your physician before proceeding with any injection therapy.
What type of shoes should I avoid if I have a painful heel bump?
You should strictly avoid footwear with rigid, unyielding posterior heel counters, narrow toe boxes that alter gait mechanics, and elevated heels (generally anything above a 1-inch heel drop). Stiff leather dress shoes, traditional running shoes with high-backed synthetic collars, and backless shoes that force you to grip with your toes should all be eliminated during active treatment. Instead, prioritize shoes with open heels, flexible mesh backing, or deep, wide heel counters that accommodate the posterior swelling without direct compression. Look for brands that advertise "soft heel collars," "drop-in midsoles," or "orthopedic-friendly designs." Additionally, temporarily using heel lifts or silicone heel sleeves can offload pressure by altering the angle of contact between your shoe and the affected anatomical region.
How long does recovery take after physical therapy for a heel knot?
Recovery timelines depend heavily on the underlying pathology, symptom chronicity, and patient compliance with home exercise programs. Acute bursitis or mild tendinopathy often improves significantly within 4 to 8 weeks of guided physical therapy, with full return to high-impact sports achievable in 12 to 16 weeks. Chronic tendinosis with significant nodular thickening or insertional calcification requires a more prolonged approach, typically spanning 3 to 6 months, as tendon remodeling is a slow, biologically regulated process. During this period, therapists will progressively transition you from isometric loading to heavy slow resistance training, then to plyometrics and sport-specific drills. Adherence to eccentric loading protocols, proper warm-up routines, and long-term biomechanical maintenance is crucial to prevent recurrence and ensure lasting recovery.
Conclusion
A painful knot on the back of the heel is more than a minor nuisance; it is a clinical indicator of underlying structural, inflammatory, or degenerative changes within the complex biomechanics of the foot and ankle. Whether stemming from Haglund's deformity, Achilles tendinopathy, retrocalcaneal bursitis, or less common metabolic conditions, the presence of a posterior heel mass warrants a systematic diagnostic approach and a disciplined, multi-faceted treatment strategy. The vast majority of patients achieve excellent outcomes through conservative management, emphasizing load modification, targeted rehabilitative exercise, strategic footwear selection, and advanced non-invasive therapies like shockwave treatment. By understanding the anatomical triggers, recognizing early warning signs, and adhering to evidence-based rehabilitation protocols, you can effectively resolve current symptoms, prevent future flare-ups, and maintain long-term mobility and foot health. Early consultation with a podiatric or orthopedic specialist ensures accurate diagnosis and personalized intervention, ultimately restoring pain-free movement and returning you to your active lifestyle safely and sustainably.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider for any health concerns or before making any decisions related to your health or treatment.

About the author
Samuel Jones, MD, is a board-certified orthopedic surgeon specializing in joint replacement and orthopedic trauma. He is a team physician for a professional sports team and practices at a renowned orthopedic institute in Georgia.