Can Sperm Cause Yeast Infections? What the Science Really Says

The relationship between sexual activity and vaginal health is a frequent source of concern, yet it remains one of the most misunderstood topics in modern reproductive medicine. Many individuals experience uncomfortable symptoms following intercourse and immediately wonder whether the biological material introduced during sex could be the culprit. Specifically, the question of can sperm cause yeast infections surfaces repeatedly in clinical consultations, online health forums, and wellness communities. While it might seem intuitive to connect the two, the underlying physiological mechanisms are far more nuanced than a simple cause-and-effect relationship. To truly understand how sexual activity influences vaginal ecology, we must examine the delicate balance of the vaginal microbiome, the chemical composition of seminal fluid, and the environmental triggers that allow opportunistic fungi to proliferate. This comprehensive guide breaks down the science behind pH fluctuations, microbial competition, and evidence-based strategies to protect reproductive wellness without compromising intimacy.
Understanding Yeast Infections: The Basics
What Is a Yeast Infection?
A vaginal yeast infection, medically termed vulvovaginal candidiasis, occurs when an overgrowth of the fungus Candida disrupts the natural equilibrium of the vaginal environment. Candida albicans is responsible for approximately 80 to 90 percent of all clinical cases, though non-albicans species like Candida glabrata and Candida tropicalis are increasingly recognized in treatment-resistant presentations. Importantly, Candida is not a foreign pathogen that must be eradicated entirely; it is a commensal organism that resides harmlessly in the gastrointestinal tract, mouth, skin, and vagina of up to 20 to 30 percent of healthy, asymptomatic individuals. Problems arise only when the immune system and microbial flora lose their regulatory control, allowing the yeast to transition from its harmless, rounded yeast form into invasive, filamentous hyphae. This morphological shift triggers inflammation, resulting in the hallmark symptoms: intense pruritus, erythema, thick white cottage-chease-like discharge, dyspareunia, and localized vulvar edema. Clinical diagnosis typically relies on symptom presentation, microscopic wet mount examination revealing pseudohyphae, and occasionally vaginal pH testing, which notably remains within the normal acidic range of 3.8 to 4.5 during candidiasis, differentiating it from bacterial vaginosis.
How the Vaginal Microbiome Works
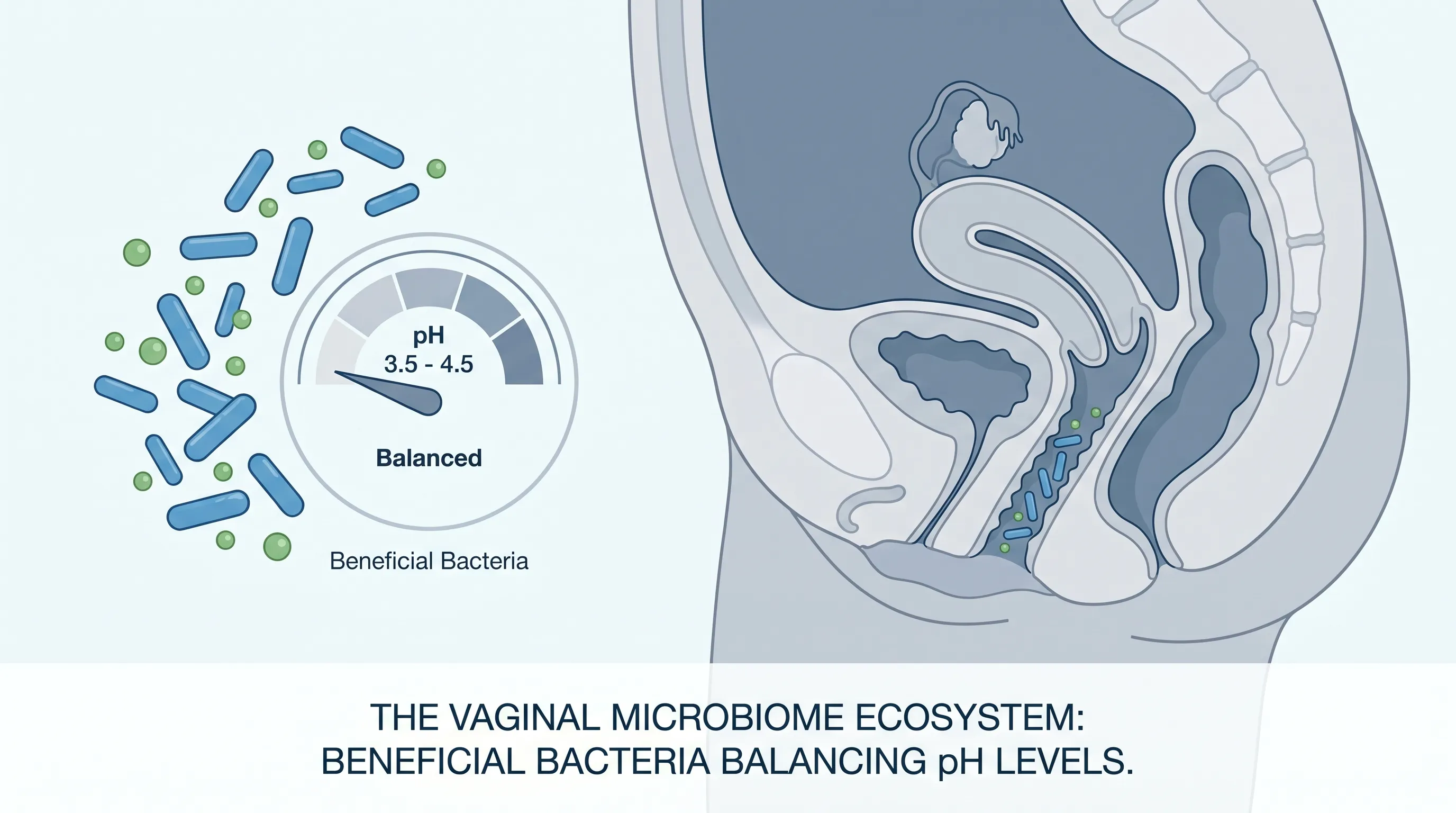
The human vagina hosts a highly specialized, dynamic ecosystem primarily dominated by Lactobacillus species. These beneficial bacteria serve as the primary line of defense against pathogenic invasion through multiple synergistic mechanisms. First, they metabolize glycogen released by estrogen-primed vaginal epithelial cells into lactic acid, maintaining the characteristic low pH that inhibits the growth of most opportunistic bacteria and fungi. Second, they produce hydrogen peroxide and bacteriocins, natural antimicrobial compounds that create a hostile environment for invaders. Third, they compete for adhesion sites and nutrient availability, effectively outcompeting potential pathogens for colonization space. This intricate balance is exquisitely sensitive to internal and external variables. Hormonal fluctuations during menstruation, pregnancy, perimenopause, or while using hormonal contraceptives can alter glycogen availability and estrogen levels, directly impacting microbial density. Systemic antibiotic use, chronic stress, immunosuppression, uncontrolled diabetes mellitus, and dietary patterns high in refined sugars can all compromise this delicate equilibrium. Understanding this foundational ecology is essential when evaluating how can sperm cause yeast infections, because the introduction of external biological fluids directly interacts with these protective mechanisms.
The Biological Interaction: Semen, pH, and Vaginal Health
The pH Scale and Vaginal Flora
The pH scale measures hydrogen ion concentration, with 7.0 representing neutrality. Healthy vaginal tissue thrives in a consistently acidic environment ranging from 3.8 to 4.5. This acidity is non-negotiable for maintaining optimal Lactobacillus dominance and suppressing the metabolic activation of Candida. When the vaginal pH rises above 4.5, the protective lactic acid barrier weakens, allowing dormant yeast spores to germinate and proliferate rapidly. Various factors can temporarily elevate vaginal pH, including menstrual blood (pH ~7.4), tap water used during cleansing (pH ~6.5 to 8.0), certain lubricants, and seminal fluid. The vagina possesses remarkable buffering capacity, capable of neutralizing minor alkaline exposures and rapidly restoring homeostasis through endogenous acidification. However, repeated or prolonged pH disruption exhausts this adaptive capacity, leading to dysbiosis. This physiological reality directly informs the conversation about can sperm cause yeast infections, as the chemical composition of semen fundamentally challenges the acidic baseline that keeps fungal populations in check.
How Seminal Fluid Alters the Environment
Semen is a complex biochemical matrix composed of spermatozoa suspended in seminal plasma. Seminal plasma itself contains fructose for energy, prostaglandins, enzymes, zinc, citric acid, and various proteins. Crucially, its pH ranges from 7.2 to 8.0, specifically designed to protect sperm during their journey through the acidic cervical mucus and into the alkaline uterine environment. During unprotected intercourse, this alkaline fluid enters the vaginal canal, temporarily neutralizing the acidic ecosystem. Research published in clinical gynecology journals demonstrates that vaginal pH can remain elevated for up to eight hours following ejaculation in some individuals. During this window, Lactobacillus activity diminishes, glycogen metabolism slows, and Candida gains a competitive advantage. Additionally, the physical presence of semen can increase local moisture and warmth, further creating an incubator-like environment conducive to fungal proliferation. For individuals with a resilient microbiome, the vagina self-corrects quickly. However, for those with preexisting risk factors such as recent antibiotic therapy, high stress, or genetic predispositions to impaired immunity, the transient pH shift introduced by semen can be the tipping point that triggers symptomatic candidiasis. This biochemical interaction provides the most scientifically grounded explanation for why individuals frequently question can sperm cause yeast infections after experiencing recurrent postcoital flare-ups.
Addressing the Core Question: Can Sperm Cause Yeast Infections?
Direct Causation vs. Contributing Factors
To answer directly, spermatozoa themselves are not pathogenic to the vaginal epithelium, nor do they introduce Candida into a previously sterile environment. Therefore, in strict microbiological terms, sperm does not directly cause yeast infections. However, the question of can sperm cause yeast infections is best answered through the lens of ecological disruption rather than direct infection. The introduction of alkaline seminal plasma acts as a significant environmental stressor. When the vaginal pH rises, Lactobacillus populations temporarily decline, glycogen utilization drops, and the natural antimicrobial barrier weakens. In susceptible individuals, this creates a permissive window for endogenous Candida to transition from commensal colonization to active overgrowth. It is essentially a classic case of ecological succession: when dominant competitors (beneficial bacteria) are temporarily suppressed, opportunistic species (yeast) exploit the newly available niche. Clinical studies consistently show that women experiencing recurrent vulvovaginal candidiasis (RVVC) often report symptom exacerbation following unprotected intercourse, particularly when ejaculation occurs intravaginally. This pattern strongly supports the conclusion that while sperm is not the primary infectious agent, the physiological changes it initiates can absolutely serve as a catalyst for yeast proliferation.
The Role of Sperm Composition and Volume
Not all exposures to seminal fluid carry equal risk. Sperm concentration, seminal volume, and individual variations in plasma composition all influence the degree of vaginal pH disruption. Men with higher seminal volumes or higher concentrations of alkaline buffering agents may cause more pronounced and prolonged pH elevation. Conversely, individuals who engage in frequent intercourse may experience cumulative pH disturbances that prevent the microbiome from fully recovering between exposures. Additionally, the presence of other components in semen, such as prostaglandins and certain immune-modulating proteins, can induce localized mild inflammation in sensitive individuals, further compromising mucosal integrity and immune surveillance. Understanding these variables is crucial for individuals trying to determine can sperm cause yeast infections in their specific circumstances. Those experiencing chronic symptoms should track exposure frequency, timing relative to menstrual cycles, and associated lifestyle factors to identify personal triggers. In many clinical cases, switching to barrier protection or adjusting intercourse frequency during high-risk periods (such as post-antibiotic use or during times of elevated stress) dramatically reduces recurrence rates, confirming the contributory role of seminal fluid in the pathogenesis of candidiasis.
Other Sexual Health Factors That Trigger Imbalance
Unprotected Sex and Microbiome Disruption
Beyond semen, the mechanical aspects of unprotected intercourse introduce multiple variables that can disrupt vaginal ecology. Friction during penetration can cause microscopic microtrauma to the vaginal mucosa, temporarily compromising the epithelial barrier and increasing local inflammatory responses. This physical irritation, combined with the introduction of skin flora, environmental contaminants, or residual lubricants, creates additional stress on the microbiome. Some individuals utilize saliva as a natural lubricant, which inadvertently introduces oral Streptococcus and Candida species directly into the vaginal canal, potentially altering microbial composition. Furthermore, the practice of not using barrier protection eliminates a physical buffer that would otherwise limit direct fluid exchange. While condoms are traditionally viewed as STI prevention tools, their role in maintaining vaginal pH stability is equally significant. When evaluating can sperm cause yeast infections, it is vital to recognize that unprotected sex acts as a multifactorial disruptor rather than a singular event. The combination of pH alteration, mechanical friction, and foreign microbial introduction creates a compounding effect that significantly elevates the risk of dysbiosis and subsequent fungal overgrowth in susceptible individuals.
Allergic Reactions to Semen or Lubricants
A distinct but frequently confused phenomenon is human seminal plasma hypersensitivity, commonly referred to as semen allergy. This condition is not a fungal infection but an immunoglobulin E (IgE) mediated allergic reaction to specific proteins in seminal fluid. Symptoms can mimic yeast infections or bacterial vaginosis, including intense itching, redness, swelling, and burning sensations following exposure to semen. Misdiagnosis often leads to inappropriate antifungal treatments that fail to resolve the underlying immune response. Additionally, commercial lubricants, particularly those containing glycerin, parabens, or chlorhexidine, can severely disrupt vaginal flora. Glycerin, a sugar derivative, serves as a direct fermentable substrate for Candida, actively feeding yeast populations and accelerating overgrowth. When individuals ask can sperm cause yeast infections, they are often unknowingly reacting to added chemicals, allergic responses to seminal proteins, or friction-related irritation rather than the sperm itself. Identifying these distinctions requires careful symptom tracking, patch testing, and consultation with a healthcare provider. Switching to hypoallergenic, glycerin-free, water-based lubricants and using high-quality latex or polyurethane condoms frequently resolves symptoms mistakenly attributed to yeast infections.
STIs vs. Yeast Infections: Understanding the Difference
Differentiating between sexually transmitted infections and fungal overgrowth is critical for appropriate treatment and long-term reproductive health. Conditions like Trichomonas vaginalis, Chlamydia trachomatis, Neisseria gonorrhoeae, and bacterial vaginosis often present with overlapping symptoms such as discharge, irritation, and dysuria. However, their etiology, treatment protocols, and public health implications differ dramatically. Yeast infections typically present with thick, white, odorless discharge and intense vulvar pruritus, while bacterial vaginosis usually produces thin, grayish-white discharge with a characteristic fishy odor and elevated vaginal pH above 4.5. Trichomoniasis often causes frothy, yellow-green discharge and significant inflammation. Misattributing symptoms can lead to delayed care, inappropriate self-medication, and persistent complications. When exploring whether can sperm cause yeast infections, it is equally important to rule out sexually transmitted pathogens that may have been introduced during the same encounter. Routine STI screening, accurate symptom recognition, and avoiding self-diagnosis are foundational pillars of sexual health management. Healthcare providers rely on nucleic acid amplification tests (NAATs), wet mount microscopy, and pH testing to distinguish between these conditions, ensuring targeted and effective intervention.

Prevention and Risk Reduction Strategies
Practical Tips for Maintaining Vaginal Health
Proactive vaginal care centers on supporting the innate resilience of the microbiome through daily lifestyle choices. First, avoid unnecessary antibiotic exposure and complete prescribed courses exactly as directed to minimize collateral damage to beneficial bacteria. Second, manage blood glucose levels effectively, as hyperglycemia creates a systemic environment that promotes Candida growth. Third, prioritize stress management techniques such as mindfulness, adequate sleep, and regular moderate exercise, as chronic cortisol elevation directly suppresses localized immune function in the vaginal mucosa. Dietary modifications play a surprising yet significant role; incorporating probiotic-rich foods like unsweetened yogurt, kefir, kimchi, and sauerkraut can help replenish Lactobacillus strains systemically. Additionally, reducing refined sugar and high-glycemic carbohydrate intake starves potential fungal overgrowth at its metabolic source. When considering can sperm cause yeast infections, implementing these foundational wellness strategies creates a resilient internal environment capable of rapidly neutralizing postcoital pH fluctuations. Hydration, fiber intake, and consistent sleep hygiene further support mucosal integrity and immune regulation, forming a comprehensive defense network that operates independently of sexual activity patterns.
Safe Sex Practices and Barrier Methods
Strategic adjustments to sexual practices can dramatically reduce recurrence risk without eliminating intimacy. The most effective intervention for individuals prone to postcoital yeast infections is consistent condom use. High-quality latex or non-latex barriers prevent direct semen exposure, preserving vaginal pH and minimizing microbial disruption. If latex sensitivity or discomfort is an issue, polyurethane or polyisoprene alternatives provide comparable protection. For couples attempting to conceive or preferring barrier-free intercourse, timing intercourse outside high-risk periods, such as immediately following antibiotic courses or during menstruation, can reduce susceptibility. Additionally, urinating shortly after sex, though primarily recommended for UTI prevention, helps flush residual fluids from the vestibule and reduces prolonged mucosal contact. Avoiding immediate washing with harsh soaps or douching is critical, as the vagina is self-cleaning; external cleansing with warm water or mild, fragrance-free emollients is sufficient. Applying a clinically validated vaginal probiotic suppository containing specific Lactobacillus rhamnosus or Lactobacillus crispatus strains 24 to 48 hours before anticipated intercourse may also bolster microbial defenses. Understanding can sperm cause yeast infections empowers individuals to make informed choices that balance sexual satisfaction with long-term ecological stability.
| Factor | Mechanism of Disruption | Preventive Strategy | Impact on Yeast Risk |
|---|---|---|---|
| Seminal Fluid Exposure | Alkaline pH neutralizes vaginal acidity temporarily | Consistent condom use | High |
| Commercial Lubricants (Glycerin-based) | Sugar derivatives ferment, feeding Candida directly | Switch to glycerin-free, water-based formulas | Moderate to High |
| Recent Antibiotic Therapy | Eliminates protective Lactobacillus populations | Probiotic supplementation, dietary fiber | High |
| Chronic Stress & Cortisol Elevation | Suppresses local mucosal immunity | Mindfulness, adequate sleep, regular exercise | Moderate |
| Uncontrolled Blood Glucose | Systemic hyperglycemia promotes fungal metabolism | Carbohydrate management, routine screening | High |
Treatment Options and When to See a Doctor
Over-the-Counter Antifungals
For mild to moderate, uncomplicated episodes, over-the-counter topical antifungals remain the first-line intervention. Clotrimazole and miconazole formulations are available in single-dose, three-day, or seven-day regimens. The choice of treatment length depends on symptom severity and patient preference, though clinical guidelines consistently indicate that shorter courses are equally effective for standard presentations. These medications work by disrupting the ergosterol synthesis pathway in fungal cell membranes, leading to cellular leakage and death. Vaginal creams, ointments, and intravaginal tablets provide localized delivery with minimal systemic absorption. When using OTC treatments, patients should complete the full prescribed course even if symptoms resolve prematurely to prevent partial eradication and resistance development. External vulvar itching can be temporarily managed with cool compresses, oatmeal baths, or barrier creams containing zinc oxide. It is important to note that frequent self-treatment without proper diagnosis can mask other conditions or lead to azole-resistant Candida strains. If symptoms persist beyond three days of OTC use or return within two months, clinical evaluation becomes necessary to confirm the diagnosis and rule out alternative pathologies.
Prescription Medications and Recurrent Cases
Individuals experiencing four or more confirmed yeast infections within a single year meet the clinical criteria for recurrent vulvovaginal candidiasis (RVVC). This condition requires a fundamentally different treatment paradigm focused on induction and maintenance therapy rather than episodic intervention. The standard protocol typically begins with an intensive induction phase using oral fluconazole (150 mg) every 72 hours for three doses to achieve complete fungal clearance. This is followed by a maintenance phase of weekly fluconazole administration for six consecutive months. For non-albicans species or azole-resistant strains, alternative agents like boric acid vaginal suppositories (600 mg daily for two to fourteen days), topical nystatin, or oral itraconazole may be utilized. Boric acid is particularly effective due to its broad-spectrum antifungal activity and ability to normalize vaginal pH, though it must be strictly used intravaginally and is contraindicated during pregnancy. When managing chronic cases, clinicians investigate underlying contributors such as undiagnosed diabetes, immunodeficiency, hormonal imbalances, or persistent environmental triggers. Addressing the recurring question of can sperm cause yeast infections in RVVC patients often reveals that consistent semen exposure is maintaining a state of chronic ecological disruption, necessitating temporary barrier use during the intensive treatment phase. Close collaboration with a gynecologist ensures personalized, evidence-based management that restores long-term microbial harmony.
Frequently Asked Questions
Can sperm cause yeast infections in otherwise healthy individuals?
While spermatozoa themselves do not introduce fungal pathogens, the alkaline seminal plasma temporarily raises vaginal pH, which can disrupt protective Lactobacillus populations and create a favorable environment for endogenous Candida to overgrow. The infection is not directly caused by the sperm but rather by the ecological shift it triggers.
Does washing after sex prevent yeast infections?
External rinsing with warm water can remove residual semen and reduce prolonged mucosal contact, potentially lowering irritation. However, internal douching or using harsh soaps actively harms the microbiome and increases infection risk. The vagina is self-cleaning, and gentle external hygiene is sufficient for maintaining optimal health.
Are yeast infections considered sexually transmitted infections?
No, vulvovaginal candidiasis is not classified as an STI. Candida naturally colonizes the human body, and overgrowth results from internal ecological imbalances rather than partner transmission. While sexual activity can trigger flare-ups, treating male partners is generally unnecessary unless they exhibit symptomatic balanitis.
How long does it take for vaginal pH to normalize after intercourse?
In individuals with a robust microbiome, vaginal pH typically restores to its baseline acidic range (3.8 to 4.5) within two to eight hours following ejaculation. Frequent intercourse, hormonal fluctuations, or underlying dysbiosis can prolong this recovery period, requiring strategic interventions to maintain microbial equilibrium.
Should individuals prone to yeast infections use condoms consistently?\nYes, barrier methods are highly recommended for those experiencing recurrent symptoms. Condoms prevent direct seminal fluid exposure, helping maintain stable pH and Lactobacillus dominance. Switching to high-quality condoms during vulnerable periods, such as post-antibiotic use or high-stress phases, significantly reduces recurrence rates.
Conclusion
The relationship between sexual intimacy and vaginal health is complex, governed by intricate biochemical interactions and microbial ecology. When addressing the persistent question of can sperm cause yeast infections, the scientific evidence clearly demonstrates that while spermatozoa are not infectious agents, the alkaline composition of seminal fluid acts as a significant ecological stressor. This temporary pH elevation can disrupt the protective Lactobacillus barrier, creating a permissive environment for endogenous Candida to proliferate into symptomatic infection. Understanding this mechanism empowers individuals to move beyond fear and toward proactive, evidence-based management. By prioritizing consistent barrier protection when necessary, utilizing hypoallergenic lubricants, supporting the microbiome through diet and stress management, and seeking clinical guidance for recurrent cases, individuals can maintain both sexual wellness and reproductive health. Knowledge is the most powerful tool in navigating intimate health concerns, and recognizing the subtle triggers that influence vaginal ecology transforms confusion into confident, informed decision-making. Always consult a qualified healthcare provider for persistent symptoms, personalized treatment plans, and comprehensive reproductive care tailored to your unique physiological profile.
Sources: Mayo Clinic - Vaginal Yeast Infection Symptoms & Causes, CDC - Bacterial Vaginosis & Trichomoniasis Overview, American College of Obstetricians and Gynecologists - Vaginal Health Guidelines, National Health Service - Thrush Management

About the author
Sofia Rossi, MD, is a board-certified obstetrician-gynecologist with over 15 years of experience in high-risk pregnancies and reproductive health. She is a clinical professor at a top New York medical school and an attending physician at a university hospital.