BV vs Yeast Infection: Which Is Worse and How to Find Relief

Navigating the complexities of vaginal health can be overwhelming, especially when faced with common yet distinctly different conditions like bacterial vaginosis and vaginal candidiasis. Many individuals struggle to identify their symptoms accurately, often leading to delayed or incorrect self-treatment. Understanding the underlying mechanisms, symptom profiles, and clinical implications of each condition is essential for restoring balance and preventing long-term complications. When evaluating which is worse bv or yeast infection, it becomes clear that the answer is not straightforward. Both conditions disrupt the delicate vaginal ecosystem, but they do so in fundamentally different ways. While one typically stems from a bacterial imbalance and the other from a fungal overgrowth, their impact on daily life, reproductive health, and psychological well-being varies significantly. This comprehensive guide explores the science behind both infections, compares their severity, outlines evidence-based treatment protocols, and provides actionable strategies for long-term prevention and optimal vaginal wellness.
Understanding Bacterial Vaginosis and Yeast Infections
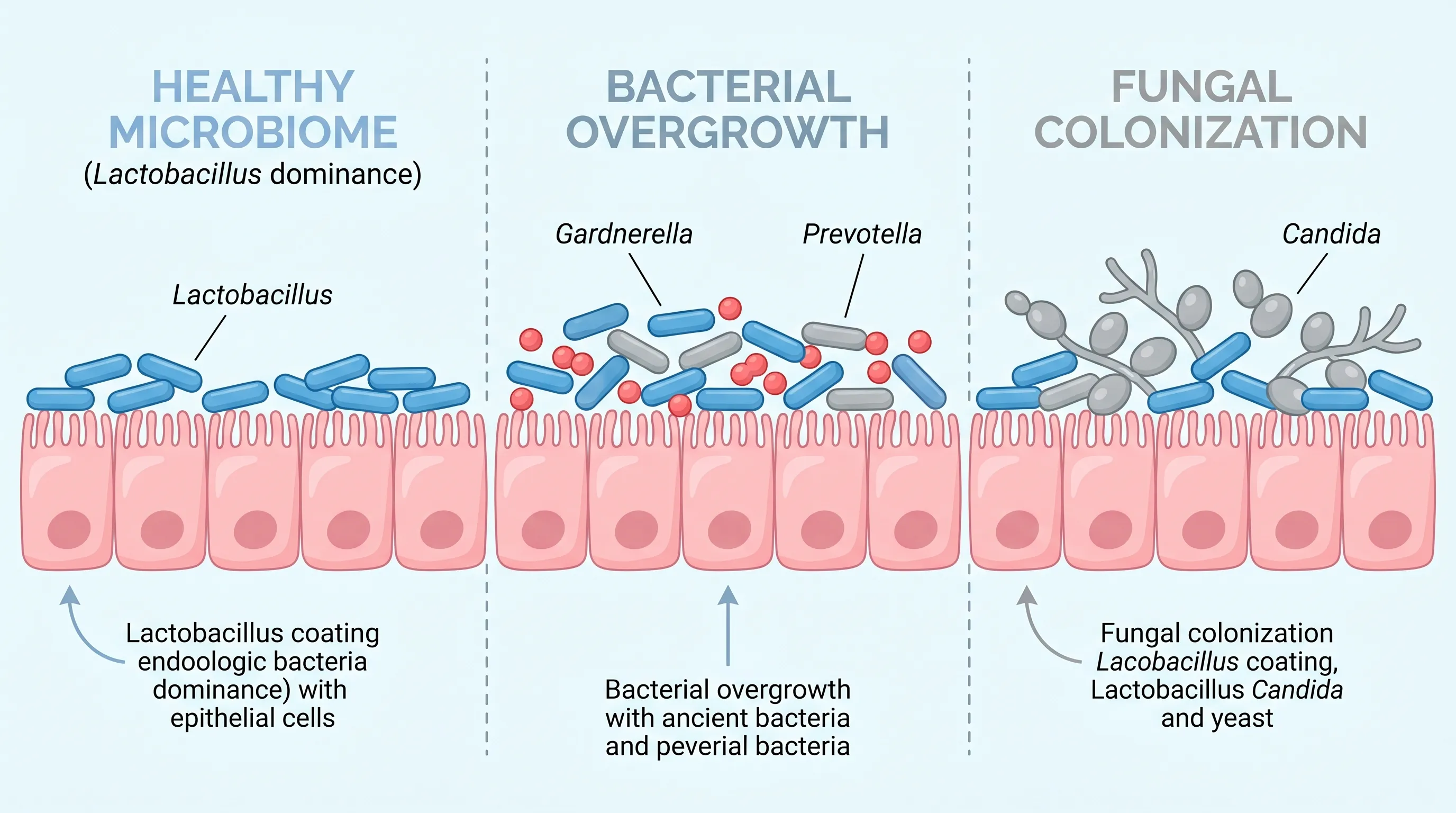
The human vagina hosts a highly complex and dynamic ecosystem of microorganisms that work synergistically to maintain optimal pH levels, produce antimicrobial compounds, and protect against pathogenic invasion. Under healthy conditions, Lactobacillus species dominate this environment, producing lactic acid that keeps vaginal pH between 3.8 and 4.5. When this balance is disrupted, opportunistic organisms can multiply unchecked, leading to inflammation, discomfort, and altered discharge. Determining which is worse bv or yeast infection requires examining how each condition originates, how it manifests, and how it responds to clinical intervention.
What Is Bacterial Vaginosis?
Bacterial vaginosis is the most common cause of abnormal vaginal discharge in women of reproductive age. Unlike traditional infections, BV is classified as a polymicrobial syndrome characterized by a decrease in beneficial Lactobacilli and an overgrowth of anaerobic bacteria, including Gardnerella vaginalis, Prevotella species, Mycoplasma hominis, and Mobiluncus. The exact trigger for this dysbiosis remains multifactorial, but known catalysts include unprotected sexual activity, frequent vaginal washing, inconsistent condom use, and smoking. BV is not classified as a sexually transmitted infection, though sexual contact can disrupt microbial equilibrium. The condition fundamentally represents a shift from an aerobic, acidic environment to an anaerobic, alkaline state.
What Is a Yeast Infection?
Vaginal candidiasis, commonly known as a yeast infection, occurs when the fungus Candida albicans (or less frequently, Candida glabrata or Candida tropicalis) proliferates beyond normal colonization levels. Unlike BV, which involves multiple bacterial species, yeast infections are predominantly fungal. Candida normally resides in the vagina in small, harmless quantities. When immune function declines, estrogen levels fluctuate, or blood sugar rises, the fungal cells can transition from yeast to hyphal forms that penetrate vaginal epithelial cells, causing intense inflammation. Understanding which is worse bv or yeast infection often comes down to the speed of onset and the severity of localized symptoms, as candidiasis typically produces more acute physical discomfort.
Key Differences in Causes and Triggers
The etiological pathways for these two conditions diverge significantly. BV is strongly linked to lifestyle and behavioral factors that raise vaginal pH above 4.5, creating an environment where anaerobic bacteria thrive. Douching, using scented hygiene products, and having multiple or new sexual partners are well-documented triggers. Conversely, yeast infections are frequently driven by hormonal shifts (pregnancy, birth control pills, menstrual cycles), prolonged antibiotic use that kills protective bacteria, uncontrolled diabetes, and tight, non-breathable clothing. While both conditions share some overlapping risk factors, recognizing their distinct triggers is essential for effective prevention and long-term management. Learn more about vaginal health triggers from the Mayo Clinic
Symptom Comparison: How to Tell Them Apart
Accurate symptom identification is the first critical step toward appropriate treatment. Misdiagnosis is common, and many women mistakenly apply antifungal treatments for bacterial issues or vice versa. By examining the characteristic signs of each condition, patients can make more informed decisions and seek timely professional care.
Common BV Symptoms
Bacterial vaginosis often presents subtly but consistently. The hallmark symptom is a thin, grayish-white discharge that coats the vaginal walls and frequently carries a distinct fishy odor, particularly noticeable after intercourse or during menstruation due to the alkaline nature of semen and blood. Unlike fungal infections, BV typically causes minimal itching or swelling. Some individuals report mild burning during urination, but intense irritation is uncommon. Vaginal pH testing in BV cases usually reveals a reading of 4.5 or higher, and wet mount microscopy often shows clue cells (epithelial cells covered with bacteria).
Common Yeast Infection Symptoms
Vaginal candidiasis produces a dramatically different clinical picture. The most recognizable sign is a thick, white, cottage cheese-like discharge that is generally odorless or has a faint yeast-like smell. Intense pruritus (itching) around the vulva and vaginal opening is nearly universal, often accompanied by erythema, edema, and burning sensations during urination or intercourse. The inflamed tissue may develop tiny fissures from scratching, leading to soreness. A vaginal pH test typically returns normal (3.8-4.5), as Candida does not significantly alkalinize the environment.
Overlapping and Confusing Signs
Despite their distinct profiles, both conditions can cause discomfort during daily activities and intercourse, leading many to wonder which is worse bv or yeast infection when symptoms appear. Mild burning, general vaginal soreness, and disrupted intimacy affect patients with either diagnosis. Additionally, mixed infections occur frequently enough that relying solely on self-assessment can be unreliable. When symptoms deviate from classic presentations, clinical evaluation becomes necessary. Healthcare providers utilize Amsel criteria for BV and microscopic wet mount or culture testing for candidiasis to ensure accurate differentiation. Review symptom guidelines from the CDC
Which Is Worse: Weighing the Severity and Complications
Severity in vaginal conditions is multidimensional, encompassing acute discomfort, recurrence potential, reproductive implications, and systemic health risks. Evaluating which is worse bv or yeast infection requires moving beyond immediate symptoms to analyze long-term clinical trajectories.
Short-Term Discomfort vs. Long-Term Risks
In the immediate term, yeast infections are widely considered more distressing due to intense itching, raw tissue irritation, and visible inflammation. The physical discomfort often disrupts sleep, exercise, and intimacy. However, BV carries a quieter but more profound set of long-term risks. The persistent alkaline environment and absence of protective Lactobacilli compromise the mucosal immune defense. This makes BV a significant risk factor for ascending infections, including endometritis and salpingitis. While yeast infections rarely ascend beyond the vagina or cervix, BV bacteria can migrate upward, triggering pelvic inflammatory disease.
Impact on Fertility and Pregnancy
The reproductive implications heavily influence which is worse bv or yeast infection from a clinical perspective. BV is strongly associated with adverse pregnancy outcomes, including preterm labor, premature rupture of membranes, low birth weight, and postpartum endometritis. The inflammatory cytokines produced by bacterial overgrowth can stimulate uterine contractions prematurely. Pregnant individuals diagnosed with BV are routinely prescribed safe antibiotics to mitigate these risks. Yeast infections during pregnancy are common due to hormonal shifts but rarely threaten fetal development. They can cause severe maternal discomfort and occasionally lead to neonatal thrush during delivery, but they do not increase miscarriage or preterm birth rates.
Recurrence Rates and Chronic Management
Both conditions demonstrate frustrating recurrence patterns, but their frequencies and management complexities differ. Approximately 50% of women with BV experience recurrence within 12 months of treatment, largely because antibiotics suppress symptoms without permanently restoring microbial dominance. Chronic or refractory BV may require extended maintenance regimens. Recurrent vulvovaginal candidiasis affects roughly 5-8% of women, defined as four or more episodes annually. Long-term management involves weekly antifungal therapy for up to six months. When weighing which is worse bv or yeast infection in terms of persistence, BV generally presents a greater challenge to permanent resolution, while recurrent yeast infections are more responsive to structured suppressive protocols.
Diagnosis and Medical Treatment Options
Effective treatment begins with precise identification. Over-the-counter availability of antifungal medications has led to widespread self-prescribing, but evidence consistently supports professional diagnosis before initiating therapy. Understanding the clinical pathways ensures appropriate, timely intervention.
Clinical Testing and Diagnosis
Healthcare providers utilize several diagnostic modalities to differentiate between conditions. The Amsel criteria require three of four clinical findings for BV diagnosis: homogeneous discharge, pH above 4.5, positive whiff test (fishy odor with potassium hydroxide), and presence of clue cells on microscopy. The Nugent score offers a more objective Gram-stain evaluation of bacterial species distribution. For yeast infections, potassium hydroxide preparation reveals pseudohyphae and budding yeast. Culture testing is reserved for atypical or treatment-resistant cases to identify non-albicans species that may require alternative antifungals. Vaginal pH remains a simple, immediate differentiator at the point of care.
Antibiotics for BV
First-line therapy for symptomatic bacterial vaginosis includes metronidazole (oral or vaginal gel) and clindamycin cream. Metronidazole effectively targets anaerobic bacteria and trichomonads while sparing most Lactobacilli when used intravaginally. A standard regimen lasts seven days. Tinidazole serves as an alternative for patients experiencing gastrointestinal side effects from metronidazole. Importantly, sexual partners are not routinely treated, as evidence does not support partner therapy improving outcomes or preventing recurrence. Patients are advised to avoid alcohol during and shortly after oral metronidazole to prevent disulfiram-like reactions. See CDC treatment guidelines for BV
Antifungals for Yeast Infections
Uncomplicated vulvovaginal candidiasis responds rapidly to topical azoles such as clotrimazole, miconazole, or terconazole administered intravaginally for 1 to 7 days. Oral fluconazole (single 150 mg dose) is equally effective and preferred by many patients for convenience. Complicated or recurrent infections require longer induction therapy (7-14 days) followed by maintenance dosing (weekly fluconazole for 6 months). Non-albicans Candida species often exhibit azole resistance and may require boric acid suppositories or nystatin therapy under strict medical supervision. Topical treatments can cause mild local burning, which typically resolves quickly.
Prevention and Lifestyle Modifications
While medical interventions clear active infections, sustainable prevention hinges on daily habits that support microbial resilience. Implementing evidence-based lifestyle modifications significantly reduces recurrence and promotes long-term vaginal wellness.
Hygiene and Clothing Choices
The external vulvar region requires minimal, gentle care. Harsh soaps, scented washes, bubble baths, and vaginal deodorants disrupt pH and strip protective lipids. Washing the external area with warm water and a mild, fragrance-free cleanser is sufficient. Wiping front to back prevents fecal bacteria from entering the vaginal opening. Clothing choices directly impact moisture and temperature regulation. Cotton underwear, loose-fitting pants, and avoiding prolonged exposure to damp swimwear or workout attire allow proper ventilation and reduce fungal proliferation. Changing out of sweaty clothes immediately after exercise is a simple yet highly effective preventive measure.

Probiotics and Gut-Vaginal Axis
Emerging research highlights the interconnectedness of gastrointestinal and vaginal microbiomes through the gut-vaginal axis. Orally administered probiotics containing specific Lactobacillus strains (particularly L. rhamnosus GR-1 and L. reuteri RC-14) have demonstrated clinical efficacy in preventing BV and yeast infection recurrence by colonizing the vaginal tract and producing bacteriocins. Dietary fiber supports beneficial gut bacteria, which indirectly modulate immune responses and estrogen metabolism. Minimizing high-glycemic foods and excessive sugar intake deprives Candida of its primary energy source. Consistent hydration supports mucosal integrity and natural cleansing mechanisms.
When to See a Healthcare Provider
Self-management is appropriate only after a condition has been professionally diagnosed and typical symptoms recur. New-onset symptoms, pregnancy, fever, pelvic pain, abnormal bleeding, or treatment failure within 3-4 days mandate clinical evaluation. When questioning which is worse bv or yeast infection during active flare-ups, remember that persistent or worsening discomfort indicates possible mixed infection, atypical pathogen involvement, or non-infectious conditions like contact dermatitis or lichen sclerosus. Early professional assessment prevents unnecessary tissue damage, inappropriate medication exposure, and potential reproductive complications.
Frequently Asked Questions
Can you have both BV and a yeast infection at the same time?
Yes, it is entirely possible to develop both bacterial vaginosis and a vaginal yeast infection simultaneously or in rapid succession. The vaginal environment is highly sensitive, and treatments for one condition (like broad-spectrum antibiotics) can sometimes disrupt the natural flora enough to trigger the other. Mixed infections require targeted medical evaluation because standard over-the-counter remedies will only address one pathogen. A healthcare provider can perform a comprehensive microscopic exam and pH testing to prescribe combination therapy safely.
How long does it take for BV and yeast infections to heal with treatment?
With appropriate prescription or over-the-counter treatment, symptom relief typically begins within 48 to 72 hours for both conditions. However, complete eradication of yeast infections generally takes 3 to 7 days for mild cases and up to 14 days for moderate or severe infections. Bacterial vaginosis usually requires a full 7-day antibiotic course (oral or vaginal) to prevent rapid recurrence. It is critical to complete the entire prescribed treatment regimen even if symptoms disappear early, as stopping prematurely significantly increases the risk of resistant or chronic dysbiosis.
Is it safe to use over-the-counter yeast medication if I suspect BV?
No, using antifungal creams or suppositories for bacterial vaginosis will not be effective and may worsen symptoms by irritating already inflamed tissue or delaying proper treatment. BV is caused by bacterial overgrowth, not fungus, so antifungal medications do not target the underlying pathogen. Self-treating without confirmation can also mask symptoms, making accurate clinical diagnosis more difficult. Always consult a healthcare provider or utilize at-home microbiome testing before initiating therapy when symptoms overlap or are unclear.
Does having BV or a yeast infection increase STI risk?
Yes, both conditions can alter the vaginal environment in ways that increase susceptibility to sexually transmitted infections. Bacterial vaginosis is particularly linked to a higher risk of acquiring HIV, chlamydia, gonorrhea, and pelvic inflammatory disease due to the thinning of the protective mucosal barrier and altered immune cell response. While yeast infections primarily cause localized inflammation and micro-tears from scratching, they can also create entry points for pathogens. Using barrier protection and maintaining a healthy vaginal pH are essential preventive measures.
Can diet and probiotics permanently cure recurrent infections?
While diet and targeted probiotics cannot guarantee a permanent cure, they play a clinically validated role in reducing recurrence rates. Consuming fermented foods, minimizing refined sugars, and supplementing with Lactobacillus rhamnosus and Lactobacillus reuteri strains can help restore microbial balance and support the production of protective lactic acid and hydrogen peroxide. However, probiotics work best as an adjunct to prescribed antimicrobial therapy and consistent lifestyle modifications rather than a standalone treatment for active infections.
Conclusion
The question of which is worse bv or yeast infection ultimately depends on the metrics used for evaluation: acute discomfort, recurrence frequency, or long-term reproductive consequences. Yeast infections deliver intense, immediate physical irritation that disrupts daily routines but rarely pose systemic threats. Bacterial vaginosis operates more insidiously, frequently causing mild or even asymptomatic presentations while quietly increasing the risk of pelvic inflammatory disease, adverse pregnancy outcomes, and heightened susceptibility to other infections. Both conditions are highly manageable with accurate diagnosis and appropriate medical intervention, yet both demand respect for their underlying microbiological complexity.
Achieving lasting vaginal health requires moving beyond reactive treatment toward proactive ecological support. Prioritizing breathable clothing, avoiding disruptive hygiene practices, maintaining balanced blood sugar levels, and incorporating evidence-based probiotics can significantly strengthen the natural defense system. When symptoms arise, resisting the urge to self-diagnose and seeking professional evaluation ensures that therapy aligns with the actual pathogen driving the imbalance. By understanding the distinct mechanisms, recognizing overlapping signs, and committing to sustainable preventive habits, individuals can confidently navigate vaginal health challenges. Remember that consistent education, open communication with healthcare providers, and mindful lifestyle choices remain the most powerful tools in preventing both conditions and maintaining optimal reproductive wellness throughout every stage of life.

About the author
Sofia Rossi, MD, is a board-certified obstetrician-gynecologist with over 15 years of experience in high-risk pregnancies and reproductive health. She is a clinical professor at a top New York medical school and an attending physician at a university hospital.