Understanding Smegma Pearl: Causes, Safe Removal, and Expert Hygiene Guidelines

Discovering a small, firm nodule in the genital area can be deeply unsettling, yet the medical reality behind a smegma pearl is far less alarming than it initially appears. Many individuals experience anxiety upon noticing unfamiliar textures or bumps on sensitive skin, often jumping to conclusions about infections or serious conditions. In reality, this phenomenon is a straightforward physiological occurrence rooted in the body’s natural cleansing and lubrication processes. Understanding the biological mechanisms that drive its formation demystifies the experience and empowers individuals to approach genital health with confidence and evidence-based practices. By exploring the clinical characteristics, safe management protocols, and preventive strategies, readers can navigate this common concern with clarity and peace of mind.
Understanding Smegma and Its Natural Composition
To fully grasp what a smegma pearl represents, it is essential to first examine the underlying substance responsible for its development: smegma itself. Smegma is a naturally occurring, whitish-to-yellowish secretion composed of exfoliated epithelial cells, sebaceous gland oils, moisture, and resident commensal microflora. Far from being a waste product or a sign of poor health, it serves a vital physiological role in maintaining the delicate moisture balance of genital mucosa. The glans penis and clitoral structures are covered in specialized mucosal tissue that lacks hair follicles but contains numerous modified sebaceous and apocrine glands. These glands continuously produce lubricating oils that reduce friction, prevent micro-abrasions, and protect against environmental irritants.
The Biological Role of Genital Secretions
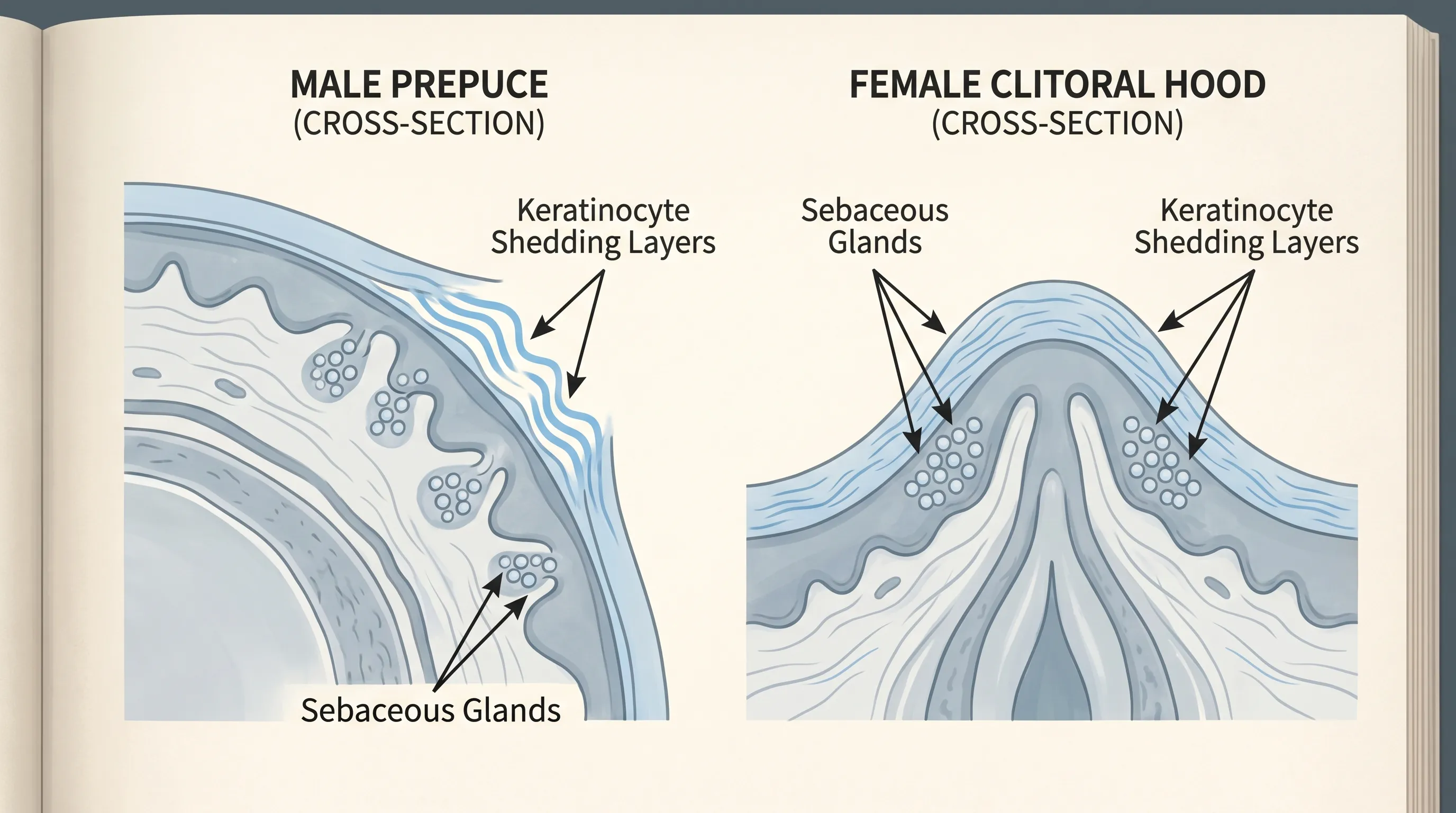
Human skin constantly undergoes cellular turnover. The epidermis sheds millions of keratinocytes daily, a process known as desquamation. In dry, exposed skin areas, these shed cells simply flake away invisibly. However, in intertriginous zones—areas where skin folds over skin—such as beneath the foreskin or within the clitoral hood, these cells cannot easily escape. They mix with localized sebum and ambient moisture, creating a soft, paste-like substance. This natural mixture acts as a biological lubricant, facilitating comfortable movement of the prepuce over the glans during daily activities and sexual function. The resident microbiome, consisting primarily of harmless bacteria and fungi, thrives in this mildly acidic, nutrient-rich environment, contributing to immune defense by outcompeting pathogenic invaders.
How Smegma Accumulates and Hardens
When regular mechanical clearance through gentle hygiene is delayed or insufficient, this natural mixture remains trapped. Prolonged exposure to oxygen, friction, and localized warmth initiates a slow oxidation process. The lipid components begin to solidify, while the keratin proteins compact and cross-link. Over weeks or months, this gradual compaction transforms the soft paste into a discrete, firmer mass. The body’s natural inflammatory and repair mechanisms may respond by laying down a thin layer of stratified squamous epithelium around the mass, effectively walling it off. This encapsulated structure is what clinicians and patients colloquially refer to as a smegma pearl. It is essentially a benign epidermal inclusion or retention cyst formed by trapped physiological secretions.
What Is a Smegma Pearl? Clinical Definition & Features
Clinically, a smegma pearl is defined as a small, localized, benign nodule resulting from the progressive compaction and encapsulation of retained genital secretions. Unlike acute inflammatory lesions or infectious growths, it develops slowly, remains stable in size, and typically causes no systemic symptoms. The term “pearl” derives from its smooth, rounded, and often glistening appearance once exposed. While the terminology is frequently used in patient education materials, it is not a formal ICD-coded diagnosis. Instead, it falls under the broader clinical categories of smegma accumulation or secondary epidermoid cysts of the genitalia.
Appearance and Physical Characteristics
Visually, these nodules range from one to five millimeters in diameter. They present as firm, smooth, well-circumscribed structures with a whitish, yellowish, or occasionally slightly tan hue. They are typically mobile beneath the superficial mucosal layer, meaning gentle palpation will reveal slight movement without attachment to deeper tissues. The overlying skin or mucosa usually appears normal, without erythema, scaling, or ulceration. Because they are composed of compacted keratin and lipids, they lack the vascularity seen in hemangiomas or the pus-filled core characteristic of acute abscesses.
Common Locations in Males and Females
Anatomically, a smegma pearl develops in areas where natural secretions pool and are sheltered from routine washing. In males, the most frequent site is the coronal sulcus—the groove encircling the glans just beneath the foreskin. The subpreputial space provides a warm, moist environment ideal for accumulation. In females, identical processes occur within the clitoral prepuce (hood) and along the inner folds of the labia minora. The anatomical configuration in both sexes creates micro-environments where desquamated cells and sebaceous output naturally collect, making these locations the primary sites for nodule formation.
Smegma Pearl vs. Other Genital Bumps
Distinguishing a benign accumulation from other common dermatological findings requires understanding key morphological differences. Pearly penile papules, for example, are small, dome-shaped, flesh-colored papules that form in regular rows around the corona and are purely physiological. Fordyce spots represent ectopic sebaceous glands visible on the shaft or labia, presenting as multiple tiny yellowish dots without central cores. True epidermoid cysts contain a distinct punctum (opening) and often express cheesy, foul-smelling keratin when ruptured. A smegma pearl lacks a punctum, forms slowly, and remains asymptomatic unless neglected or secondarily inflamed. Recognizing these distinctions prevents unnecessary anxiety and inappropriate self-treatment.
| Feature | Smegma Pearl | Pearly Penile Papules | Fordyce Spots | Epidermoid Cyst |
|---|---|---|---|---|
| Origin | Compacted sebum + keratinocytes | Angiofibromas (benign) | Ectopic sebaceous glands | Follicular infundibulum occlusion |
| Appearance | Single/smooth white-yellow nodule | Multiple uniform dome papules in rows | Tiny scattered yellowish macules/papules | Firm nodule with central punctum |
| Location | Coronal sulcus, clitoral hood | Corona of glans | Shaft, labia, scrotum | Anywhere on shaft, labia, groin |
| Symptoms | Usually asymptomatic | Asymptomatic | Asymptomatic | May become inflamed if infected |
| Management | Hygiene or minor excision if needed | Observation, no treatment needed | Observation or cosmetic removal | Incision/expression or excision |
The Pathophysiology of Cyst Formation
Understanding how a simple accumulation evolves into a structured nodule requires examining cellular turnover, glandular secretion dynamics, and epithelial response mechanisms. The process is gradual, multifactorial, and entirely physiological until mechanical or microbial interference alters the local environment.
Cellular Shedding and Sebum Trapping
The epidermis of the genital mucosa undergoes rapid turnover compared to keratinized skin elsewhere on the body. This accelerated renewal is an adaptive response to friction, moisture, and potential microbial colonization. As older cells detach from the basal layer, they migrate outward. Without adequate clearance, they intermingle with continuous sebum output from Tyson’s glands (in males) and Montgomery glands (in females, though primarily areolar, analogous sebaceous structures exist genitally). This mixture forms a cohesive, viscous matrix that adheres to mucosal folds.
Oxidation, Encapsulation, and Nodule Development
Trapped within a relatively anoxic but warm microenvironment, the lipid-protein matrix undergoes slow dehydration and oxidation. Free radicals from ambient oxygen interact with unsaturated fatty acids in sebum, promoting polymerization. Concurrently, macrophages and local fibroblasts recognize the accumulating debris as foreign material. Rather than triggering acute inflammation, the tissue initiates a chronic, low-grade foreign body response. Fibroblasts deposit a thin collagenous capsule, while the overlying epithelium hyperplasts slightly to seal off the area. This encapsulation prevents the contents from dispersing into surrounding tissue but also traps them permanently until mechanical removal or natural extrusion occurs. The resulting structure is firm, discrete, and clinically classified as a secondary epidermal inclusion cyst.
Symptoms, Warning Signs, and When to Worry
The clinical presentation of a smegma pearl is overwhelmingly benign. Most individuals remain entirely unaware of its presence until it becomes palpable or visible during routine hygiene or intimate activity. However, recognizing the boundary between normal physiological variation and pathological change is crucial for maintaining genital health and preventing secondary complications.
Typical Asymptomatic Presentation
In the vast majority of cases, these nodules produce no discomfort, itching, or functional impairment. They do not interfere with urination, sexual function, or daily mobility. The only noticeable signs may include a slight visual prominence beneath the mucosa or a very mild, characteristic odor if hygiene has been inconsistent. This odor stems from bacterial breakdown of trapped proteins and lipids, not from infection. Proper cleansing typically resolves the scent rapidly.
Red Flags Requiring Medical Attention
While the nodule itself is harmless, certain accompanying symptoms warrant professional evaluation. Sudden onset of pain, localized swelling, or erythema suggests secondary balanitis or cellulitis. Purulent or foul-smelling discharge may indicate bacterial overgrowth or yeast proliferation, particularly in individuals with diabetes or compromised immunity. Inability to retract the foreskin or clitoral hood after prolonged accumulation signals potential preputial adhesions or acquired phimosis. Systemic symptoms such as fever, malaise, or lymphadenopathy in the inguinal region are never associated with uncomplicated accumulation and require immediate clinical assessment to rule out sexually transmitted infections or deeper soft tissue pathology.
Diagnosis and Clinical Evaluation
Medical evaluation for a suspected smegma pearl is straightforward and relies primarily on clinical inspection. Healthcare providers utilize visual examination and gentle palpation to characterize the lesion’s size, mobility, consistency, and relationship to surrounding anatomical structures. No laboratory testing or imaging is necessary unless atypical features are present.
Visual Examination and Differential Diagnosis
During a routine physical exam, a clinician will retract the foreskin or gently part the labial folds to visualize the corona or clitoral hood. The hallmark features—smooth surface, whitish-yellow coloration, mobility, and lack of surrounding inflammation—usually confirm the diagnosis. If the presentation deviates from typical findings, providers consider differential diagnoses including molluscum contagiosum, condyloma acuminatum, lichen sclerosus, or early squamous cell carcinoma in situ. A dermoscope may be used to examine surface architecture, though this is rarely required for clear-cut cases.
Ruling Out Infections and Malignancy
Historically, outdated medical literature speculated that chronic smegma accumulation increased the risk of penile and cervical cancers due to alleged carcinogen production. Rigorous modern epidemiological studies, including longitudinal cohort analyses and meta-analyses, have conclusively debunked this association. The International Agency for Research on Cancer (IARC) does not classify smegma as a carcinogen. Persistent inflammation from poor hygiene, however, can create a microenvironment susceptible to human papillomavirus (HPV) persistence. Therefore, clinicians emphasize that while the accumulation itself is harmless, maintaining healthy tissue integrity supports overall cancer prevention strategies like HPV vaccination and routine screening.
Safe Management, Treatment, and Removal Options
Management strategies for a smegma pearl are heavily weighted toward conservative, hygiene-based approaches. Medical intervention is reserved for cases involving complications, persistent discomfort, or patient preference after thorough counseling.
First-Line Conservative Hygiene Practices
The cornerstone of management involves restoring regular mechanical clearance. Patients are instructed to gently retract the prepuce or clitoral hood to the point of comfort without forcing it. Lukewarm water is applied using clean hands, with light circular motions to soften and rinse away superficial debris. This process should be performed daily during routine bathing. The goal is not aggressive scrubbing but consistent, gentle hydration and rinsing. Over several days, the nodule’s outer layers will naturally soften, allowing gradual dissolution or migration toward the surface.
Medical Interventions and Minor Procedures
If conservative measures fail to resolve a fully encapsulated nodule, or if it causes recurrent irritation, a urologist or dermatologist may recommend a minor in-office procedure. Local anesthesia is administered, followed by a sterile micro-incision. The contents are carefully expressed using blunt dissection to avoid mucosal trauma. For larger, well-defined cysts, complete surgical excision with primary closure may be performed to prevent recurrence. Topical antibiotics or antifungals are only prescribed if swab cultures confirm secondary bacterial or candidal overgrowth. Routine antibiotic therapy without confirmed infection is strongly discouraged to prevent microbiome disruption and antimicrobial resistance.
Why Self-Removal Is Strongly Discouraged
Home extraction attempts carry significant risks. The genital mucosa is thin, highly innervated, and rich in vasculature. Using fingernails, tweezers, or improvised tools frequently causes mucosal lacerations. These micro-wounds breach the epithelial barrier, allowing opportunistic pathogens like Staphylococcus aureus or Candida species to colonize deeper tissues. Repeated trauma can trigger a fibrotic healing response, leading to preputial adhesions, scarring, or functional phimosis. Additionally, improper expression may push contents deeper into the dermis, converting a superficial accumulation into a true inflammatory epidermoid cyst. Clinical guidelines uniformly advise against self-manipulation and recommend professional evaluation for persistent concerns.

Prevention and Daily Genital Care Guidelines
Long-term prevention relies on establishing sustainable, evidence-based hygiene habits that respect the delicate balance of the genital microbiome while ensuring adequate mechanical clearance of natural secretions.
Proper Washing Techniques for All Genders
Effective genital hygiene does not require specialized products or aggressive techniques. During daily showers or baths, individuals should use lukewarm water to cleanse the entire area. Harsh soaps, antibacterial washes, and heavily fragranced cleansers disrupt the natural acidic pH and beneficial flora, increasing susceptibility to irritation and secondary overgrowth. After gentle retraction and rinsing, the area must be thoroughly patted dry with a clean, soft towel. Moisture retention creates a breeding ground for maceration and fungal proliferation. Wearing loose-fitting, breathable cotton underwear further reduces heat and humidity buildup.
Lifestyle and Fabric Choices for Optimal Hygiene
Beyond washing routines, daily lifestyle choices significantly influence genital health. Prolonged sitting, intense exercise without prompt showering, and tight synthetic fabrics create occlusive environments that accelerate secretion trapping and bacterial proliferation. Individuals who sweat heavily during workouts benefit from changing into dry clothing immediately afterward. For uncircumcised males, establishing a consistent, gentle retraction routine from childhood onward prevents chronic accumulation and reduces the risk of adolescent or adult balanoposthitis. Females practicing clitoral hood hygiene should avoid internal douching or vaginal steaming, as these practices force moisture and chemicals into protected spaces, disrupting natural self-cleaning mechanisms.
Frequently Asked Questions
Is a smegma pearl dangerous or a sign of cancer?
No. A smegma pearl is a completely benign accumulation of natural genital secretions, dead skin cells, and moisture. Modern epidemiological research has conclusively debunked historical myths linking chronic smegma accumulation to penile or cervical cancer. It is non-infectious, non-malignant, and poses no oncological risk. Regular hygiene and routine clinical screenings remain the gold standard for long-term genital health.
Can I safely remove a smegma pearl at home by squeezing it?
No. Squeezing, picking, or attempting to puncture a smegma pearl at home is strongly discouraged. The genital mucosa is highly vascular and delicate. Forceful extraction can cause micro-tears, introduce pathogenic bacteria, trigger secondary infection, and lead to painful scarring or preputial adhesions. Professional evaluation ensures sterile, trauma-free removal when necessary.
How long does it take for a smegma pearl to resolve with proper hygiene?
With consistent gentle cleansing using lukewarm water, most superficial accumulations gradually soften and dissipate within one to two weeks. If the nodule is fully encapsulated by an epithelial layer, it may persist until professionally expressed or excised by a healthcare provider. Patience and consistency yield the safest outcomes.
Do smegma pearls occur in women as well as men?
Yes. While more commonly discussed in uncircumcised males due to the preputial space, females can also develop smegma accumulation within the clitoral hood and labial minora folds. The physiological composition and hygiene principles remain identical across anatomical variations. Both sexes benefit from gentle, daily rinsing and moisture management.
When should I see a doctor about a genital nodule?
Seek prompt medical evaluation if you experience sudden pain, rapid enlargement, purulent discharge, spreading redness, fever, foul odor, or inability to retract the foreskin or clitoral hood. These symptoms may indicate secondary balanitis, infection, or an unrelated dermatological condition requiring professional intervention. Early assessment prevents complications and provides peace of mind.
Key Takeaways
A smegma pearl is a harmless, physiologically normal accumulation resulting from trapped keratinocytes, sebum, and moisture beneath genital folds. It is not an infection, not a sexually transmitted condition, and carries no malignant potential. Consistent, gentle hygiene using lukewarm water and avoiding harsh cleansers effectively prevents and resolves most cases. Self-manipulation or aggressive scrubbing should be strictly avoided to prevent mucosal trauma and secondary complications. When in doubt, or if red flag symptoms emerge, consulting a board-certified urologist, dermatologist, or gynecologist ensures accurate diagnosis and safe management. Prioritizing informed, evidence-based genital care fosters long-term comfort, confidence, and optimal reproductive health. For comprehensive, medically reviewed guidance on smegma and hygiene practices, visit Healthline, consult the American Urological Association patient resources, or review standardized NHS recommendations on smegma and genital hygiene.
About the author
Carlos Ruiz, MD, FACS, is a board-certified urologist specializing in minimally invasive and robotic surgery for urologic cancers. He is a senior partner at a large urology group in Houston, Texas, and is involved in clinical trials for new prostate cancer treatments.