Puffy Breast Nipples: Causes, Hormonal Links, and Evidence-Based Management Strategies

When examining the wide spectrum of human breast anatomy, few features prompt as many questions as areolar contour and nipple presentation. Many individuals notice that their nipples appear slightly rounded, elevated, or full around the edges, often describing this as having puffy breast nipples. While the internet frequently fuels unnecessary anxiety, the reality is that this presentation is remarkably common and usually falls within the range of normal physiological variation. Understanding the underlying tissue architecture, hormonal drivers, and potential clinical triggers can transform uncertainty into informed awareness. This comprehensive guide explores the medical science behind areolar puffiness, outlines when professional evaluation is warranted, and provides evidence-based strategies for management, comfort, and long-term breast health. Whether you are navigating developmental changes, hormonal shifts, or simply seeking clarity about your body, you will find actionable insights grounded in current clinical literature and dermatological best practices.
Understanding Puffy Breast Nipples: Anatomy and Physiology
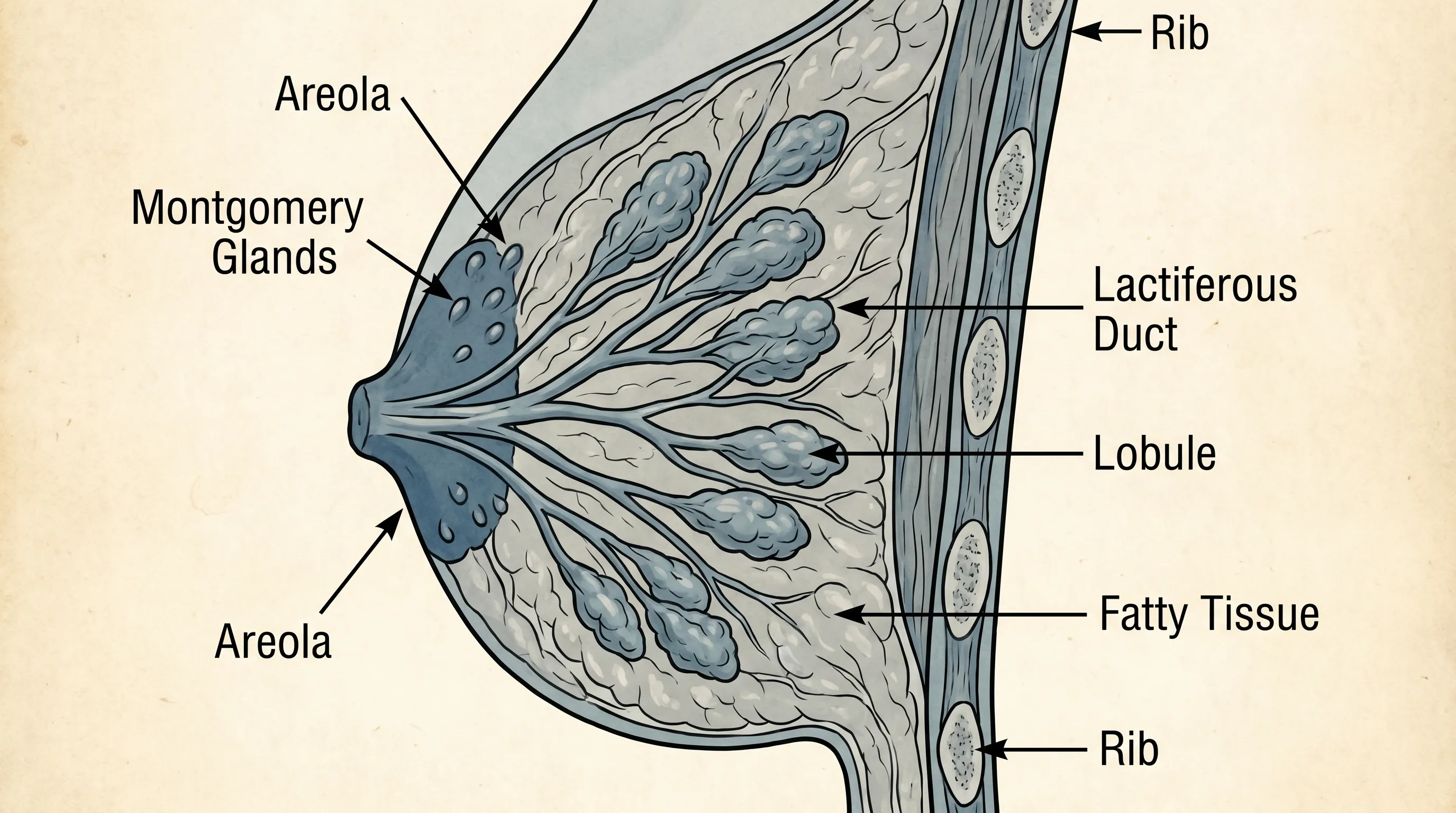
The human breast is a complex organ composed of glandular tissue, adipose tissue, connective ligaments, blood vessels, lymphatic channels, and specialized sensory structures. At the center lies the nipple-areolar complex (NAC), which serves as both a functional and aesthetic focal point. The areola itself is a circular pigmented area surrounding the nipple, containing Montgomery glands (also known as areolar glands), which secrete a lubricating, antimicrobial oil. When discussing puffy breast nipples, it is essential to recognize that the contour of the areola can naturally vary from flat and flush with the surrounding skin to slightly domed or pronounced. This variation is primarily dictated by the underlying distribution of glandular and connective tissue, as well as localized vascular and lymphatic flow.
What Are Puffy Nipples? Defining the Term
Medically speaking, puffiness refers to a soft, rounded elevation of the areolar margin that may extend slightly beyond the nipple base. Unlike inverted or retracted nipples, puffy breast nipples protrude gently and maintain a consistent shape under normal conditions. In clinical settings, dermatologists and breast specialists classify this as a benign anatomical variant unless accompanied by erythema, scaling, discharge, or rapid asymmetry. The Montgomery glands often become more prominent in these cases, contributing to the textured, slightly raised appearance. Research published by the American College of Obstetricians and Gynecologists confirms that areolar morphology shifts throughout life, with puffiness being a frequently documented and normal finding in adolescents, pregnant individuals, and premenopausal women.
The Role of Areolar and Montgomery Glands
The areolar tissue is rich in smooth muscle fibers and specialized sebaceous glands. Montgomery glands are modified sweat glands that respond to temperature, hormonal fluctuations, and tactile stimulation. When these glands become engorged with secretions or when the surrounding stromal tissue retains mild interstitial fluid, the areola assumes a fuller, more convex shape. This physiological response is entirely normal and often serves to protect the nipple from friction, infection, or environmental irritation. In many cases, individuals with naturally denser glandular architecture in the NAC will exhibit puffy breast nipples without any underlying disease process. The vascular supply to this region is highly responsive, meaning that temporary puffiness can also result from changes in ambient temperature, physical activity, or emotional states.
Normal Variations vs. Clinical Concerns
Distinguishing between physiological variation and pathological changes requires a clear understanding of baseline anatomy versus progressive symptoms. Normal puffy breast nipples are typically symmetrical, painless, and stable over months or years. They do not discharge fluid, ulcerate, or cause persistent itching. Conversely, clinical concerns arise when puffiness develops rapidly, occurs unilaterally, or is accompanied by skin changes such as thickening, redness, or a rash resembling eczema. Conditions like Paget’s disease of the breast or localized infections can mimic benign puffiness but require prompt medical intervention. Maintaining regular self-awareness and scheduling routine clinical breast exams remain the most effective strategies for early detection and peace of mind.
Hormonal Influences and Developmental Changes
Hormonal regulation plays a central role in breast development, tissue remodeling, and areolar contour. Estrogen, progesterone, prolactin, and testosterone interact in complex feedback loops that directly influence the volume, density, and elasticity of mammary tissue. When hormone levels fluctuate—whether due to natural life stages, pharmacological interventions, or endocrine dysregulation—the appearance of puffy breast nipples can become more pronounced or change temporarily.
Puberty and Breast Development Stages
During Tanner stage breast development, which typically occurs between ages 8 and 13 in individuals assigned female at birth, the areola often expands and becomes slightly raised. This is part of the normal maturation process as glandular ducts proliferate and stromal tissue accumulates. For many adolescents, this transitional phase presents as puffy breast nipples that gradually flatten as development stabilizes. In males, transient breast tissue stimulation during puberty can also cause mild areolar prominence due to temporary estrogen-to-androgen ratio shifts. Pediatric endocrinologists emphasize that these changes are self-limiting and rarely require intervention unless they persist beyond typical developmental windows or cause significant psychosocial distress.
Pregnancy, Lactation, and Postpartum Shifts
Pregnancy triggers profound hormonal and structural adaptations in the breast. Rising levels of human chorionic gonadotropin (hCG), estrogen, and progesterone stimulate ductal branching and alveolar growth in preparation for milk production. The areola frequently darkens, enlarges, and adopts a fuller, puffed contour as Montgomery glands increase in size and secretory activity. During lactation, milk ducts become distended, further contributing to areolar elevation. Postpartum, as prolactin levels normalize and involution occurs, the tissue gradually returns to its pre-pregnancy state, though some degree of permanent structural change may remain. Mayo Clinic guidelines highlight that monitoring for signs of mastitis or blocked ducts is essential during this phase, as localized inflammation can exaggerate puffiness.
Menstrual Cycle Fluctuations
The monthly menstrual cycle creates a rhythmic pattern of hormonal exposure that directly affects breast tissue. During the luteal phase (after ovulation), progesterone levels peak, promoting fluid retention and glandular swelling in the breasts and areola. Many individuals notice increased fullness, tenderness, and a more pronounced areolar contour one to two weeks before menstruation begins. This cyclical variation is entirely physiological and typically resolves within a few days of menses onset. Tracking symptoms across multiple cycles can help differentiate normal hormonal puffiness from persistent changes that warrant evaluation. Lifestyle modifications, including caffeine reduction and targeted nutritional support, can mitigate discomfort associated with these monthly fluctuations.
Hormonal Imbalances: PCOS, Thyroid, and Estrogen Dominance
Chronic endocrine disruptions can significantly alter breast morphology. Polycystic ovary syndrome (PCOS) often presents with relative androgen excess but can also involve insulin resistance and altered estrogen metabolism, leading to unpredictable breast tissue responses. Hypothyroidism or hyperthyroidism affects systemic metabolic rate and prolactin clearance, sometimes resulting in breast swelling and areolar fullness. Additionally, conditions termed estrogen dominance—where estrogen activity outpaces progesterone—can promote glandular proliferation and fluid retention in the NAC. Functional medicine practitioners and endocrinologists recommend comprehensive hormone panels, including fasting insulin, SHBG, and free estradiol, to identify underlying drivers. The Cleveland Clinic provides extensive clinical protocols for evaluating and managing these hormonal patterns through targeted lifestyle and medical therapies.
Common Causes of Puffy Nipples in Different Demographics
Breast anatomy and hormonal landscapes differ across age groups and biological sexes, making demographic-specific context essential for accurate assessment. Recognizing how puffy breast nipples present in various populations helps clinicians tailor evaluation strategies and reduces unnecessary anxiety for patients.
Adolescents and Teenagers
During the rapid growth phases of early adolescence, areolar tissue frequently appears fuller and more prominent. This is part of normal mammary gland maturation and typically resolves or stabilizes within two to four years. Parental education and adolescent healthcare visits should normalize these changes, emphasizing that puffy breast nipples in teens rarely indicate pathology. If accompanied by rapid unilateral growth, hard nodules, or significant pain, a pediatrician or adolescent medicine specialist should conduct an ultrasound to rule out rare conditions like juvenile fibroadenoma or phyllodes tumor.
Adult Women: When Puffiness Is Normal
For adult women, areolar contour naturally evolves with age, weight fluctuations, pregnancies, and menopause. Many individuals maintain mild to moderate areolar fullness throughout their reproductive years without issue. Post-menopausal women often experience tissue atrophy and decreased glandular density, leading to flatter areolar profiles. However, those on hormone replacement therapy (HRT) may notice renewed glandular stimulation and temporary puffiness. Routine clinical breast examinations and age-appropriate mammographic screening remain the cornerstone of preventive care, ensuring that benign variations are distinguished from early neoplastic changes.
Gynecomastia and Puffy Nipples in Men
Gynecomastia is characterized by benign proliferation of ductal and stromal tissue beneath the areola, frequently presenting as puffy breast nipples in males. It affects up to 65% of boys during mid-puberty and persists in approximately 30% of adult men. The condition results from an imbalance between estrogenic stimulation and androgenic inhibition. Medications such as spironolactone, finasteride, antipsychotics, and certain antidepressants are well-documented contributors. Additionally, excessive adipose tissue, alcohol consumption, and liver dysfunction can elevate systemic estrogen levels. Clinical evaluation typically involves physical examination, hormone profiling, and occasionally breast ultrasound to confirm glandular enlargement. Endocrine Society guidelines recommend a conservative approach for pubertal cases and targeted medical or surgical intervention for persistent, symptomatic adult presentations.
Medication-Induced Breast Changes
Numerous prescription medications influence breast tissue architecture through dopaminergic inhibition, prolactin elevation, or direct hormonal receptor modulation. Antipsychotics like risperidone and olanzapine frequently cause hyperprolactinemia, leading to galactorrhea and areolar swelling. Cardiovascular agents, proton pump inhibitors, and anti-androgens also carry breast tissue side effects. When puffy breast nipples develop shortly after initiating a new medication, patients should consult their prescribing physician rather than discontinuing treatment independently. Dose adjustments, therapeutic substitution, or adjunctive dopamine agonists can often resolve the issue while maintaining primary treatment efficacy.
Identifying Underlying Medical Conditions
While most cases of areolar fullness are benign, certain clinical red flags necessitate prompt diagnostic evaluation. Understanding the differential diagnosis helps patients communicate effectively with healthcare providers and ensures that serious conditions are not overlooked.
Paget’s Disease and Nipple Changes
Mammary Paget’s disease is a rare form of breast cancer that presents with eczematous changes of the nipple and areola. Symptoms include persistent itching, burning, crusting, and a puffy or thickened appearance that does not respond to topical steroids. Unlike benign puffiness, Paget’s disease typically involves one side and may be associated with an underlying ductal carcinoma. Biopsy remains the gold standard for diagnosis. Early detection dramatically improves prognosis, making it essential to seek dermatological or surgical evaluation for any chronic, treatment-resistant nipple changes.
Fibroadenomas and Benign Breast Conditions
Fibroadenomas are the most common benign breast tumors, particularly in women under 30. While they usually present as discrete, mobile masses in the breast parenchyma, larger lesions near the NAC can cause secondary areolar distortion and puffiness. Fibrocystic breast changes, driven by hormonal sensitivity, also contribute to cyclical swelling and texture irregularities. Ultrasound imaging is highly effective at differentiating solid masses from cysts, guiding appropriate management from watchful waiting to minimally invasive aspiration.
Hormonal Disorders and Endocrine Disruptors
Beyond natural fluctuations, environmental endocrine disruptors (e.g., bisphenol-A, phthalates, and certain pesticides) can mimic estrogenic activity and subtly alter breast tissue responsiveness over time. While direct causal links to isolated puffy breast nipples remain under investigation, minimizing exposure to known xenoestrogens supports overall endocrine health. Clinicians increasingly incorporate environmental history into breast assessments, particularly for patients with unexplained tissue changes or concurrent menstrual irregularities.
Management and Treatment Options
Addressing puffy breast nipples requires a personalized approach based on underlying etiology, symptom severity, and patient goals. Conservative management remains the first-line strategy for most individuals, while surgical intervention is reserved for structural, symptomatic, or psychologically impactful cases.
When to Seek Professional Medical Evaluation
A comprehensive clinical evaluation should be pursued if you experience sudden asymmetry, persistent pain, nipple retraction, bloody or serous discharge, skin ulceration, or rapid tissue enlargement over weeks to months. Initial assessment typically includes a detailed history, physical examination, and targeted imaging such as diagnostic mammography or high-resolution breast ultrasound. Laboratory testing for prolactin, thyroid function, and sex hormone binding globulin may be ordered if endocrine dysfunction is suspected. Establishing a baseline with a board-certified gynecologist or breast specialist provides clarity and prevents diagnostic delays.
Non-Surgical and Conservative Approaches
For hormonally driven or fluid-related puffiness, lifestyle modifications form the foundation of conservative care. Wearing well-fitted, supportive bras with adequate cup depth and wide straps reduces mechanical strain on the NAC and prevents friction-related irritation. Compression garments or sports bras during exercise minimize tissue movement and discomfort. Topical emollients containing calendula, chamomile, or vitamin E can soothe dry or sensitive areolar skin, though they do not alter underlying tissue structure. Patients should avoid aggressive massage, exfoliation, or unregulated topical creams claiming to shrink areolar tissue, as these can cause microtears, dermatitis, or unintended hormonal absorption.
Medical Interventions and Hormonal Therapy
When puffy breast nipples stem from documented endocrine imbalances, targeted medical therapy can yield significant improvement. Prolactin-lowering agents such as cabergoline or bromocriptine are prescribed for hyperprolactinemia-induced breast changes. In males with gynecomastia, selective estrogen receptor modulators (SERMs) like tamoxifen or aromatase inhibitors may be considered off-label under specialist supervision. For PCOS-related symptoms, combined oral contraceptives or metformin can restore ovulatory cycles and reduce glandular stimulation. All pharmacological interventions require careful risk-benefit analysis and regular follow-up laboratory monitoring.
Surgical Correction: Areolar Reduction and Nipple Reshaping
When conservative and medical approaches fail to address structural concerns, surgical options become viable. Areolar reduction surgery involves excising a concentric ring of pigmented skin and tightening the remaining tissue to create a smaller, flatter contour. Glandular tissue excision or liposuction may be combined for patients with dense fibroglandular tissue or significant adipose accumulation. These procedures are typically performed under local anesthesia with intravenous sedation, featuring incisions along the areolar border to minimize visible scarring. Recovery involves wearing a surgical compression garment for 4-6 weeks, avoiding strenuous upper body activity, and attending postoperative visits for suture removal and wound assessment. Complications, while uncommon, can include altered nipple sensation, asymmetry, or delayed healing, emphasizing the importance of selecting a board-certified plastic surgeon with extensive breast contour experience.
Lifestyle Modifications and Home Care Strategies
Daily habits profoundly influence systemic inflammation, hormonal equilibrium, and tissue responsiveness. Integrating evidence-based self-care practices can complement medical management and enhance overall breast comfort.
Supportive Undergarments and Posture
Proper bra fitting is foundational for individuals experiencing areolar fullness or breast heaviness. Underwire, wireless, or sports bras should be professionally sized to ensure complete breast encapsulation without digging into the inframammary fold or constricting lymphatic drainage. Poor posture exacerbates mechanical stress on the chest wall, potentially worsening perceived puffiness and discomfort. Strengthening the upper back, shoulder girdle, and core muscles through targeted resistance training improves thoracic alignment and distributes weight more evenly.
Nutritional Adjustments for Hormonal Balance
Dietary patterns directly impact endocrine function and fluid retention. Prioritize whole foods rich in omega-3 fatty acids (salmon, flaxseed, walnuts), cruciferous vegetables (broccoli, cauliflower), and high-fiber plant sources to support hepatic estrogen metabolism and insulin sensitivity. Reduce refined carbohydrates, excessive sodium, and alcohol intake, which promote systemic inflammation and interstitial fluid accumulation. Staying adequately hydrated paradoxically reduces water retention by signaling the kidneys to optimize electrolyte balance. Consultation with a registered dietitian specializing in hormonal health can provide individualized macronutrient guidance and supplement recommendations, such as myo-inositol or magnesium glycinate.
Skin Care and Topical Considerations
The areolar skin is thinner and more sensitive than surrounding breast tissue, requiring gentle cleansing and moisturization. Avoid harsh soaps, alcohol-based toners, and heavily fragranced products that can compromise the epidermal barrier. After bathing, apply a thin layer of fragrance-free, ceramide-rich moisturizer to maintain hydration and elasticity. If experiencing dryness or mild irritation from friction, consider applying a hypoallergenic barrier cream before physical activity. Consistent skin care supports tissue integrity and reduces the likelihood of secondary dermatitis that can mimic or exacerbate puffiness.
| Feature | Normal Physiological Variation | Concerning Clinical Change |
|---|---|---|
| Symmetry | Typically bilateral and consistent | Often unilateral or rapidly asymmetric |
| Duration | Stable over months or fluctuates predictably with menstrual cycle | Progressive enlargement over weeks to months |
| Pain Level | Mild cyclical tenderness or asymptomatic | Persistent, sharp, or localized pain |
| Skin Changes | Smooth, uniform pigmentation, visible Montgomery glands | Scaling, crusting, ulceration, or dimpling |
| Discharge | None or clear/milky with pregnancy/lactation | Spontaneous bloody, brown, or purulent discharge |
| Response to Lifestyle | May improve with hydration, support, and cycle tracking | Unaffected by conservative measures |

Frequently Asked Questions
Are puffy breast nipples a normal anatomical variation?
Yes, puffy breast nipples are frequently a normal anatomical variation influenced by genetics, hormonal fluctuations, and developmental stages. For many individuals, the areolar tissue naturally retains more fluid or glandular density, resulting in a rounded, slightly elevated contour without any underlying pathology. Clinical guidelines emphasize that isolated puffiness, when symmetrical and asymptomatic, falls within the spectrum of healthy breast diversity.
When should I see a doctor for puffy nipples?
You should schedule a medical evaluation if you notice sudden onset, unilateral swelling, persistent pain, nipple discharge (especially bloody or clear), skin dimpling, itching that does not resolve, or if the puffiness is accompanied by a palpable breast lump. These symptoms warrant clinical assessment to rule out hormonal imbalances, benign tumors, or malignant conditions. Early consultation ensures accurate diagnosis and timely intervention when necessary.
Can puffy nipples in males indicate a medical condition?
Yes, puffy nipples in males often point to gynecomastia, a benign enlargement of glandular breast tissue caused by an imbalance between estrogen and testosterone. It can result from puberty, aging, medications, liver disease, or endocrine disorders. A healthcare provider can differentiate true glandular growth from excess adipose tissue through physical examination and, if indicated, imaging or hormone panels.
Do lifestyle changes or diet help reduce puffy nipples?
While structural or hormonal puffiness often requires medical management, lifestyle adjustments like reducing sodium intake to minimize fluid retention, maintaining a stable weight, limiting alcohol and processed foods, and managing stress can support overall hormonal equilibrium and may gradually reduce mild areolar swelling. Consistent hydration, adequate fiber intake, and regular physical activity further promote systemic detoxification and endocrine regulation.
Is surgical correction available for puffy breast nipples?
Yes, surgical options such as areolar reduction, nipple reshaping, or glandular tissue excision are available for individuals experiencing significant physical discomfort or psychological distress. Procedures are typically performed by board-certified plastic surgeons or breast specialists and require careful preoperative hormonal and clinical screening. Recovery protocols and long-term outcomes should be thoroughly discussed during consultation.
Conclusion
Navigating changes in breast anatomy requires a blend of anatomical literacy, hormonal awareness, and proactive healthcare engagement. The presence of puffy breast nipples is overwhelmingly a benign reflection of your body's natural design, shaped by developmental milestones, endocrine rhythms, and genetic predisposition. By distinguishing between physiological variation and clinical warning signs, you can make informed decisions about self-monitoring, lifestyle optimization, and medical consultation. Whether your goal is enhanced comfort, hormonal balance, or cosmetic refinement, evidence-based strategies exist to support your wellness journey. Prioritize routine clinical evaluations, maintain open communication with qualified healthcare providers, and approach breast health with both scientific understanding and compassionate self-care. Remember that every individual's anatomy tells a unique story, and recognizing the difference between normal variation and genuine medical concern is the cornerstone of long-term reproductive and systemic health.

About the author
Sofia Rossi, MD, is a board-certified obstetrician-gynecologist with over 15 years of experience in high-risk pregnancies and reproductive health. She is a clinical professor at a top New York medical school and an attending physician at a university hospital.