What Age Do Breasts Stop Growing? A Complete Medical Timeline
Breast development represents one of the most visible and clinically significant transformations during female adolescence, marking a pivotal milestone in physiological maturation. For many young individuals, parents, and healthcare providers, navigating the physical, emotional, and psychological shifts of puberty raises a fundamental clinical question: what age do breasts stop growing? While popular media and cultural narratives often suggest a rigid, uniform timeline for physical maturation, medical science reveals a highly individualized developmental trajectory that is governed by complex endocrine signaling, genetic predisposition, and environmental health factors. The primary growth phase typically spans four to five years following menarche, with most individuals reaching full architectural development around age eighteen. However, subtle tissue remodeling, fat redistribution, and hormonal stabilization frequently continue well into the early to mid-twenties. Understanding this natural variability is essential for promoting body confidence, recognizing clinical red flags, and supporting healthy tissue maturation. This comprehensive medical guide will examine the biological mechanisms driving mammary growth, outline the standardized Tanner staging system used by pediatric endocrinologists, clarify evidence-based benchmarks for pubertal completion, and provide actionable strategies for navigating developmental changes. By distinguishing clinical realities from widespread myths, we can establish a clear, scientifically grounded framework for understanding what age do breasts stop growing, how normal asymmetry functions, and why lifelong tissue responsiveness remains a vital aspect of women's health.
Understanding the Biological Timeline of Mammary Development
The physiological journey of breast maturation is orchestrated by a highly synchronized neuroendocrine network that responds to both internal genetic blueprints and external environmental cues. To fully appreciate what age do breasts stop growing, it is necessary to examine the foundational biological drivers that initiate, sustain, and eventually stabilize tissue growth. Mammary development does not occur in isolation; it is deeply integrated with skeletal maturation, metabolic regulation, and reproductive system readiness. The entire process relies on precise hormonal gradients, receptor distribution patterns, and cellular differentiation mechanisms that unfold gradually across multiple years. Recognizing these underlying mechanisms provides valuable context for caregivers and adolescents who may feel anxious about perceived deviations from standard developmental charts.
The Hypothalamic Trigger and Hormonal Orchestration
Puberty begins when a small but powerful structure at the base of the brain, known as the hypothalamus, initiates the pubertal cascade. This region releases gonadotropin-releasing hormone (GnRH) in a pulsatile pattern, which signals the anterior pituitary gland to secrete follicle-stimulating hormone (FSH) and luteinizing hormone (LH). These gonadotropins travel through the bloodstream and stimulate the ovaries to begin synthesizing estrogen, the primary driver of mammary ductal elongation, branching, and vascularization. Progesterone follows shortly thereafter, promoting lobuloalveolar development, stromal expansion, and the formation of milk-producing units. This hormonal orchestration is what fundamentally answers the clinical inquiry regarding what age do breasts stop growing, as the gradual rise, peak, and eventual stabilization of these sex hormones dictate the duration and intensity of tissue proliferation. According to expert reviews from Flo Health, this endocrine activation typically begins between ages eight and thirteen, establishing a predictable yet flexible window for pubertal initiation.
Genetic Programming and Polygenic Influence
While hormones provide the biochemical signal for growth, genetics establish the structural blueprint. Hereditary influences account for approximately forty to sixty percent of final breast size determination, functioning as a polygenic trait much like adult height, bone density, and eye color. Multiple genes regulate estrogen receptor sensitivity, progesterone receptor density, and adipocyte proliferation patterns within the mammary stroma. Research consistently demonstrates that daughters often develop breast tissue volumes and contour characteristics that closely mirror maternal or maternal-line relatives, though nutritional status and metabolic health can modulate this expression. No external intervention can override this predetermined genetic programming, which is why clinical professionals emphasize patience and physiological acceptance during developmental transitions. When individuals wonder what age do breasts stop growing, understanding that genetic timelines are highly individualized helps alleviate unnecessary anxiety about peer comparisons or societal expectations.
The Interplay of Adipose and Glandular Tissues
Breast volume is composed of two primary components: fibroglandular tissue and adipose (fat) tissue. Estrogen actively promotes fat deposition within the mammary region, which accounts for the significant volume increase observed during stages three through five. Concurrently, glandular structures undergo extensive branching and ductal network expansion to prepare for potential future lactation. This dual-tissue architecture explains why fluctuations in body weight, nutritional intake, and metabolic rate can temporarily alter breast appearance even after primary growth concludes. Because adipose distribution patterns continue shifting throughout early adulthood, many individuals notice subtle contour changes well past the typical completion window. Medical literature confirms that understanding this tissue composition is essential when evaluating what age do breasts stop growing, as the glandular framework may mature earlier while fat redistribution patterns stabilize much later in the twenties.

Mapping Development Through the Tanner Stages
To standardize the assessment of pubertal progression across clinical settings, pediatricians and endocrinologists utilize the Tanner staging system, developed by British pediatrician Dr. James Mourilyan Tanner in the 1950s. This five-stage classification remains the gold standard for tracking sexual maturation, providing a structured framework for evaluating whether developmental pacing falls within normal physiological parameters. The system evaluates both breast contour and areolar morphology, allowing healthcare providers to objectively measure progression without relying on subjective age expectations alone. When addressing what age do breasts stop growing, clinicians reference Tanner stage five as the definitive marker of mature tissue architecture, though individual pacing through earlier stages varies significantly based on genetic, metabolic, and environmental factors.
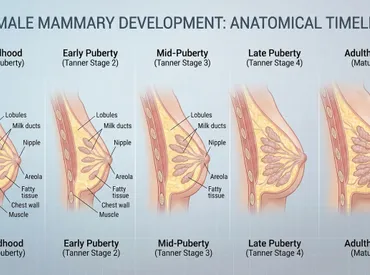
Stage 1 to Stage 2: The Initiation Phase
Stage one represents the prepubertal baseline, characterized by a flat chest wall with minimal tissue elevation and only slight nipple protrusion. The onset of stage two marks thelarche, typically occurring between ages eight and thirteen, though clinically normal variations can range from seven to fourteen years. The earliest visible sign is the formation of a breast bud, a small, firm, disc-shaped mound of glandular tissue that develops directly beneath the nipple-areolar complex. This initial elevation reflects rising estrogen levels and the beginning of ductal sprouting. The areola typically widens slightly during this phase, and some adolescents report localized tenderness or heightened sensitivity due to rapid cellular proliferation and increased blood flow. Stage two generally precedes menarche by approximately two years, establishing a predictable timeline for anticipating subsequent pubertal milestones. Monitoring progression from stage one to two provides early clinical indicators of hypothalamic-pituitary-ovarian axis activation.
Stage 3 to Stage 5: Peak Growth and Architectural Maturation
Stage three represents the period of most active proliferation, usually occurring between ages ten and fourteen. During this phase, the breast and areola continue to enlarge without a clear separation in contour, and internal lobular structures begin forming as progesterone levels rise. Estrogen-driven ductal branching accelerates, while stromal connective tissue reorganizes to support expanding glandular architecture. Stage four introduces a distinct morphological change: the areola and nipple elevate to form a secondary mound above the primary breast contour. This phase reflects peak hormonal fluctuations and maximal cellular activity, typically occurring between ages eleven and fifteen. Finally, stage five achieves the mature adult breast profile, with a smooth contour where the areola and nipple recede back into the generalized breast mound. Hormonal stabilization, reduced growth factor activity, and completed lobuloalveolar development characterize this final stage, which most individuals reach between twelve and eighteen years of age. Understanding these progressive milestones clarifies what age do breasts stop growing, as the transition to stage five represents the clinical endpoint of primary developmental expansion.
| Stage | Typical Age Range | Physical Characteristics | Hormonal Activity |
|---|---|---|---|
| Stage 1 | Pre-puberty (under 8) | Flat chest, minimal tissue, slight nipple elevation | Low estrogen, baseline GnRH |
| Stage 2 | 8-13 years | Breast bud forms, areola widens, localized tenderness | Initial estrogen surge |
| Stage 3 | 10-14 years | Continued enlargement, lobes develop, smooth contour | Rising estrogen & progesterone |
| Stage 4 | 11-15 years | Secondary mound of areola/nipple, peak proliferation | Maximum hormonal fluctuation |
| Stage 5 | 12-18 years | Mature contour, areola recedes into breast mound | Hormonal stabilization |
Answering the Core Question: What Age Do Breasts Stop Growing?
The central clinical inquiry regarding what age do breasts stop growing does not yield a single, universal answer, but rather a statistically established range that accommodates normal physiological variability. Extensive pediatric research and longitudinal developmental studies indicate that the majority of individuals complete primary mammary maturation between seventeen and eighteen years of age. This timeline aligns with broader skeletal and reproductive system readiness, reflecting the body's prioritization of structural stability before full tissue maturation concludes. However, clinical professionals consistently emphasize that subtle morphological adjustments, adipose redistribution, and hormonal fine-tuning frequently extend into the early twenties. Recognizing this extended maturation window helps prevent unnecessary concern among adolescents who may observe minor volume or contour changes during late high school or early college years.
The Typical Eighteen-Year Milestone
By age eighteen, the vast majority of females have reached Tanner stage five, indicating that ductal branching, lobular differentiation, and stromal organization have achieved their genetically predetermined architecture. Estrogen and progesterone receptors stabilize, cyclical menstrual patterns regulate, and growth hormone secretion declines from pubertal peaks to adult maintenance levels. This milestone correlates closely with other developmental markers, such as growth plate closure in long bones, pelvic maturation, and metabolic rate stabilization. Clinical data from Medical News Today confirms that eighteen serves as a reliable benchmark for primary growth completion, though it should be viewed as a statistical median rather than a rigid biological deadline. Understanding what age do breasts stop growing at this median point provides a helpful reference frame while acknowledging that individual timelines may naturally extend several months or even a few years beyond it.
Continued Subtle Maturation in the Early Twenties
Even after primary architectural development concludes, mammary tissue remains highly responsive to endocrine fluctuations. Many individuals experience gradual volume adjustments, slight contour softening, and areolar pigment stabilization well into their early to mid-twenties. These changes are driven by the complete stabilization of the hypothalamic-pituitary-ovarian axis, consistent menstrual cycling, and adult metabolic patterns. Weight fluctuations, physical activity levels, stress management, and nutritional habits during this period can influence perceived size without representing active glandular proliferation. The Doctor Network clinical review notes that mammary tissue reaches full architectural development in the early twenties, meaning what age do breasts stop growing should be conceptualized as a transitional plateau rather than an abrupt cessation. This extended maturation phase is entirely normal and reflects the body's final optimization of tissue composition before entering long-term adult maintenance.
Post-Menarche Correlation and Skeletal Development
A commonly referenced clinical correlation links menarche to remaining height growth and overall pubertal pacing. On average, females grow approximately seven centimeters (2.75 inches) in stature after their first menstrual cycle, with adult height typically achieved by ages fourteen to fifteen. This skeletal maturation timeline runs parallel to breast development, reinforcing the concept that systemic growth processes operate on synchronized biological schedules. When healthcare providers evaluate developmental concerns, they often cross-reference menarche timing, height velocity, and Tanner staging to determine whether progression aligns with normal physiological parameters. Understanding this correlation provides additional clarity when assessing what age do breasts stop growing, as it demonstrates that mammary maturation follows a coordinated timeline with broader adolescent growth patterns rather than functioning in isolation.
Navigating Early and Late Developmental Patterns
While the average developmental window provides a useful clinical reference, pediatric endocrinology recognizes that biological systems operate within a spectrum of normal variation. Early initiation or delayed progression of pubertal changes can trigger legitimate questions regarding developmental health, necessitating evidence-based guidelines for when observation is sufficient versus when clinical evaluation is warranted. Addressing what age do breasts stop growing requires acknowledging that both accelerated and delayed timelines can represent healthy variations, provided they fall within established medical parameters and lack underlying pathological indicators.
Precocious Puberty: When Development Begins Before Age Eight
Breast development or the appearance of breast buds prior to age eight is classified as precocious puberty. This early activation may stem from premature hypothalamic triggering, adrenal gland irregularities, ovarian cysts, or exposure to exogenous hormonal compounds. While many cases represent benign familial early maturation, precocious development can occasionally lead to premature epiphyseal closure, resulting in shorter adult stature. Clinical guidelines recommend comprehensive endocrine evaluation, including bone age radiography, hormone panel testing, and neuroimaging when indicated. Early intervention, when medically necessary, focuses on safely modulating gonadotropin activity to allow age-appropriate developmental pacing. Parents and caregivers should consult pediatric specialists if secondary sexual characteristics emerge well before the typical eight-to-thirteen window, ensuring that underlying physiological factors are appropriately assessed.
Delayed Puberty and Clinical Evaluation Thresholds
Conversely, the absence of any breast budding by age thirteen qualifies as delayed puberty and warrants medical assessment. Potential contributors include constitutional growth delay, low body fat percentages from athletic training or restrictive nutrition, chronic systemic illness, thyroid dysfunction, or primary ovarian insufficiency. Delayed menarche beyond age fifteen, regardless of breast development status, also requires clinical investigation to rule out anatomical variations, hormonal deficiencies, or genetic conditions. Pediatric providers typically conduct growth curve analysis, nutritional assessment, and targeted hormone testing to identify reversible factors. Reassurance remains crucial for most adolescents experiencing late-onset development, as constitutional delay often resolves spontaneously once the endocrine axis naturally activates. Understanding what age do breasts stop growing includes recognizing that late starters often complete maturation later, following the same four-to-five-year post-onset timeline without indicating pathology.
When Benign Variations Require No Intervention
The vast majority of early or late developmental patterns fall within the realm of normal biological diversity. Family history plays a significant predictive role; if maternal or paternal female relatives experienced early or delayed puberty, similar patterns frequently appear in subsequent generations. Clinical evaluation focuses primarily on ruling out systemic illness, ensuring adequate nutritional intake, and monitoring for psychological distress related to peer differences. Healthcare professionals emphasize that interventions are rarely necessary unless underlying medical conditions are identified or developmental progression completely stalls. Providing accurate education about natural variability helps reduce anxiety and promotes healthy body image during potentially confusing transitional periods.

Debunking Growth Myths: Medical Realities vs. Popular Claims
The internet is saturated with commercially driven claims promising accelerated breast enlargement, targeted tissue expansion, and rapid contour alteration through supplements, topical applications, or specialized exercise regimens. These claims consistently contradict established endocrine physiology and lack rigorous scientific validation. Addressing what age do breasts stop growing requires actively dispelling misinformation that preys on adolescent insecurities and promotes unsafe or financially exploitative products. Medical consensus firmly establishes that mammary tissue growth cannot be artificially manipulated without disrupting natural hormonal balance or causing unintended systemic side effects.
The Science Behind Supplements, Creams, and Targeted Exercises
Phytoestrogen-rich supplements, herbal formulations, and massage-based techniques frequently market themselves as natural growth accelerants. However, clinical research demonstrates that oral supplements do not selectively target mammary tissue and instead exert systemic effects that may disrupt menstrual regularity, trigger hormonal imbalances, or interact with existing medications. Topical creams cannot penetrate deep enough to stimulate glandular proliferation or ductal branching, while exercises targeting the pectoralis major merely strengthen underlying muscle fibers without altering overlying breast volume or shape. The Doctor Network explicitly states that no interventions can accelerate this natural developmental timeline, as mammary tissue growth follows predetermined genetic programming. Recognizing these physiological limitations protects individuals from fraudulent products and redirects focus toward evidence-based wellness practices.
Understanding Natural Asymmetry and Receptor Distribution
Approximately eighty-eight percent of women exhibit noticeable size or shape differences between breasts, a completely normal anatomical variation rooted in asymmetric hormone receptor distribution and localized blood flow patterns during development. One breast may initiate growth up to six months before its counterpart, and minor discrepancies often persist throughout adulthood. Media portrayals frequently obscure this reality, fostering unrealistic expectations of perfect symmetry. Clinical professionals reassure patients that asymmetry rarely requires surgical correction unless differences cause significant physical discomfort or psychological distress. Accepting natural anatomical variation is a crucial component of healthy adolescent development and long-term body confidence.
Lifelong Tissue Responsiveness Beyond Adolescence
Even after primary development concludes, breast tissue remains highly dynamic throughout the lifespan. Menstrual cycle fluctuations cause predictable cyclical swelling and tenderness due to transient progesterone and estrogen shifts. Pregnancy triggers massive lobuloalveolar expansion, lactation alters tissue density, and menopause initiates gradual glandular involution replaced by adipose tissue. Weight gain and loss similarly impact perceived volume because fat cells within the stroma readily expand or shrink in response to metabolic changes. Understanding what age do breasts stop growing therefore requires recognizing that primary architectural completion does not equate to permanent structural stasis. Lifelong hormonal responsiveness ensures continuous, predictable tissue adaptation aligned with reproductive and metabolic phases.
Supporting Healthy Breast Tissue Throughout Adolescence
While biological timelines dictate the natural pace of development, lifestyle choices, nutritional habits, and supportive care significantly influence overall tissue health, comfort, and long-term wellness. Implementing evidence-based strategies during pubertal transitions promotes optimal endocrine balance, minimizes physical discomfort, and fosters positive body awareness. Healthcare providers recommend a holistic approach that prioritizes physiological support over artificial modification, ensuring that developmental changes occur naturally and sustainably.
Nutritional Foundations for Optimal Hormonal Balance
Adequate caloric intake, balanced macronutrients, and micronutrient density are essential for healthy pubertal progression. Severe caloric restriction, excessive athletic training, or eating disorders can suppress GnRH pulsatility, delaying breast development and menstrual onset. Conversely, diets rich in healthy fats, lean proteins, complex carbohydrates, and essential vitamins (particularly vitamins A, D, E, and B-complex) support robust hormone synthesis and cellular proliferation. Omega-3 fatty acids help modulate inflammation and support tissue remodeling, while adequate hydration maintains optimal connective tissue elasticity. Registered dietitians emphasize that nutrition should fuel natural development rather than attempt to accelerate or alter it. Maintaining a balanced, sustainable eating pattern establishes lifelong metabolic health and ensures that the body possesses the biochemical resources necessary to complete developmental milestones without interruption.
Proper Supportive Garments and Postural Considerations
As breast volume increases, adequate support becomes crucial for preventing musculoskeletal strain, minimizing localized discomfort, and promoting healthy posture during rapid growth phases. Professionally fitted bras, particularly those with wide shoulder straps, adjustable bands, and moisture-wicking fabrics, distribute weight evenly across the thoracic cage and upper back. Transitioning from training bras to supportive everyday styles should occur when adolescents report physical discomfort or when tissue expansion impacts daily activities. Postural awareness is equally important, as forward shoulder rounding often develops as a compensatory response to changing center of gravity. Incorporating gentle thoracic mobility exercises, scapular stabilization routines, and core strengthening movements counteracts postural strain and supports long-term spinal health. Proper support does not alter growth trajectories but significantly enhances comfort during active maturation periods.
Recognizing Abnormal Symptoms and When to Seek Guidance
While cyclical tenderness, mild asymmetry, and temporary contour shifts are entirely normal, certain symptoms warrant prompt medical evaluation. Sudden, painful lumps, skin dimpling, nipple discharge unrelated to lactation, localized warmth or redness, or rapid unilateral enlargement require clinical assessment to rule out cystic formations, fibroadenomas, or inflammatory conditions. Additionally, persistent pain that disrupts sleep, school attendance, or physical activity should be evaluated by a pediatric provider or adolescent medicine specialist. Routine self-awareness and periodic clinical breast examinations during adolescent wellness visits establish baseline familiarity with personal tissue architecture, making it easier to identify genuine deviations from normal developmental patterns. Healthcare access remains essential for addressing physical concerns and providing accurate, age-appropriate education that empowers informed health decisions.
Frequently Asked Questions
At what exact age do breasts typically stop growing?
Breast development generally concludes around age 18, following a 4 to 5 year progression after menarche. However, subtle tissue remodeling, hormonal stabilization, and adipose redistribution frequently continue into the early twenties. The timeline is highly individualized and governed by genetic programming and endocrine pacing.
Can breast size be accurately predicted based on family genetics?
Hereditary factors determine approximately 40-60% of final breast volume, making family history a strong predictive baseline. Maternal lineage patterns often mirror closely, though nutritional status, metabolic health, and environmental factors can modulate final expression. Genetics establish potential ranges rather than exact measurements.
Is it clinically normal for one breast to develop faster than the other?
Yes, asymmetry is exceptionally common, affecting roughly 88% of women. Differences in localized hormone receptor sensitivity and blood flow distribution frequently cause one side to initiate growth up to six months earlier. Minor contour variations typically persist harmlessly throughout adulthood.
Do targeted exercises, supplements, or creams safely increase breast size?
No. Scientific evidence does not support the efficacy of topical applications, herbal formulations, or localized exercises for increasing mammary volume. These methods cannot override predetermined genetic and hormonal pathways and may disrupt menstrual regularity or trigger unintended systemic effects.
When should early or delayed development prompt a professional medical evaluation?
Clinical assessment is recommended if breast development begins before age 8, if no budding occurs by age 13, or if menarche is absent by age 15. Additionally, sudden painful lumps, rapid asymmetric swelling, persistent discomfort, or skin changes warrant timely evaluation to rule out underlying conditions.
Conclusion
Understanding what age do breasts stop growing requires looking beyond rigid cultural expectations and embracing the nuanced reality of human developmental biology. Primary mammary maturation typically concludes between ages seventeen and eighteen, following a predictable four-to-five-year trajectory that begins with thelarche and aligns closely with broader pubertal milestones. However, the early twenties bring continued hormonal stabilization, adipose refinement, and subtle architectural optimization that reflect the body's natural completion phase. Genetics establish foundational parameters, hormones orchestrate cellular proliferation, and environmental health factors modulate overall pacing, creating a highly individualized developmental experience. Recognizing normal asymmetry, debunking commercially driven growth myths, and prioritizing supportive lifestyle practices empower adolescents and caregivers to navigate this transition with confidence and clinical accuracy. When development falls outside standard age windows, pediatric evaluation ensures that underlying physiological factors are appropriately addressed while preserving natural progression. Ultimately, mammary tissue remains dynamic throughout life, responding predictably to reproductive, metabolic, and hormonal cycles. By focusing on evidence-based health strategies, proper support, and realistic anatomical expectations, individuals can foster lifelong breast wellness, body confidence, and physiological resilience across every stage of development.
For further medically reviewed guidance on pubertal development and adolescent wellness, consult resources from Medical News Today, Flo Health, and the comprehensive clinical analysis provided by Doctor Network. Always discuss developmental concerns with a qualified pediatric endocrinologist or adolescent medicine specialist to receive personalized, evidence-based care.

About the author
Sofia Rossi, MD, is a board-certified obstetrician-gynecologist with over 15 years of experience in high-risk pregnancies and reproductive health. She is a clinical professor at a top New York medical school and an attending physician at a university hospital.