Sore Breasts and Ovulation: Your Guide to Causes, Symptoms & Relief

Key points
- Estrogen's Role: In the first half of your cycle (the follicular phase), estrogen levels rise to prepare for ovulation. Estrogen stimulates the growth and enlargement of the milk ducts within your breasts. As ductal tissue expands, it increases blood flow to the area and draws additional fluid into the stromal space, leading to a sensation of heaviness.
- Progesterone's Impact: After an egg is released during ovulation, your body enters the luteal phase. Progesterone levels rise significantly to prepare the uterine lining for a potential pregnancy. This hormone causes the milk glands (lobules) in the breasts to swell and can lead to increased tenderness, fullness, and pain. Progesterone also promotes sodium and water retention in the body, which can exacerbate tissue edema and stretch the delicate nerve endings embedded within the breast fascia.
Experiencing sore, tender, or swollen breasts around the middle of your menstrual cycle is a common, and often confusing, symptom. This discomfort, medically known as cyclical mastalgia, is frequently linked to ovulation. While it's usually a normal part of the monthly hormonal rhythm, it can raise questions about fertility, pregnancy, and overall breast health. In fact, clinical studies suggest that up to 70% of individuals who menstruate will experience cyclical breast pain at some point in their reproductive years, with peak prevalence occurring between the ages of 30 and 50. For some, the discomfort is merely a fleeting annoyance, while for others, it can significantly impact daily activities, exercise tolerance, and even sleep quality. Understanding the physiological underpinnings of this symptom is the first step toward distinguishing normal hormonal fluctuations from conditions that may require clinical evaluation.
This comprehensive guide synthesizes medical insights and research to explain why your breasts hurt during ovulation, how to distinguish this symptom from others, and what you can do for relief. By exploring the intricate relationship between reproductive hormones, breast tissue architecture, and lifestyle factors, we aim to provide a clear, evidence-based roadmap for managing ovulation-related breast discomfort and navigating fertility tracking with confidence.
Why Do Breasts Hurt During Ovulation? The Hormonal Connection
The primary reason for breast soreness around ovulation is the fluctuation of key reproductive hormones. Your menstrual cycle orchestrates a complex hormonal dance, and your breast tissue is highly responsive to these changes. To fully grasp why discomfort peaks during this specific window, it helps to understand both the endocrine shifts and the anatomical structure of the breast itself.
Breast tissue is not a static organ; it is a dynamic, hormone-responsive structure composed of glandular tissue (milk-producing lobules and ducts), fibrous connective tissue (Cooper’s ligaments that provide structural support), and adipose (fat) tissue. Throughout your menstrual cycle, the balance between estrogen, progesterone, and prolactin directly influences the proliferation and fluid dynamics within these tissues.
- Estrogen's Role: In the first half of your cycle (the follicular phase), estrogen levels rise to prepare for ovulation. Estrogen stimulates the growth and enlargement of the milk ducts within your breasts. As ductal tissue expands, it increases blood flow to the area and draws additional fluid into the stromal space, leading to a sensation of heaviness.
- Progesterone's Impact: After an egg is released during ovulation, your body enters the luteal phase. Progesterone levels rise significantly to prepare the uterine lining for a potential pregnancy. This hormone causes the milk glands (lobules) in the breasts to swell and can lead to increased tenderness, fullness, and pain. Progesterone also promotes sodium and water retention in the body, which can exacerbate tissue edema and stretch the delicate nerve endings embedded within the breast fascia.
This hormonal combination creates the perfect conditions for the dull, achy soreness many experience. According to research from Johns Hopkins Medicine, this type of cyclical pain is the most common form of breast discomfort and is nearly always hormonal [[3]]. The discomfort is fundamentally driven by physiological proliferation and stromal edema, which mechanically stimulate the rich network of sensory nerves in the breast.
Interestingly, a study from the University of British Columbia found that mild breast tenderness and swelling are more common in cycles with normal ovulation than in those with ovulatory disturbances, suggesting it can be a sign of a healthy, functioning cycle [news source 1]. This correlation exists because adequate progesterone production is a direct marker of successful ovulation. Without the luteinizing hormone (LH) surge triggering follicular rupture and subsequent corpus luteum formation, progesterone remains low, and the characteristic post-ovulatory breast fullness often fails to materialize.
Individual sensitivity also plays a crucial role. Genetic factors influence how densely packed hormone receptors are within breast tissue, meaning two people with identical hormone levels may experience drastically different levels of discomfort. Additionally, factors that affect hormonal metabolism and clearance, such as liver function, alcohol consumption, stress-induced cortisol elevation, and body fat percentage, can subtly alter the estrogen-to-progesterone ratio, further modulating symptom severity.
 Breast tenderness often peaks during the luteal phase, after ovulation, due to a rise in progesterone. Source: Tuune Blog
Breast tenderness often peaks during the luteal phase, after ovulation, due to a rise in progesterone. Source: Tuune Blog
What Does Ovulation Breast Soreness Feel Like?
The sensation of ovulation-related breast pain can vary from person to person and even from cycle to cycle. Common descriptions include:
- A dull, heavy, or aching pain.
- General tenderness to the touch.
- A feeling of fullness or swelling.
- Increased sensitivity, especially in the nipples.
- Pain that affects both breasts, often in the upper, outer quadrants.
- Discomfort that can sometimes radiate into the underarm area.
The pain typically begins around the time of ovulation and lasts through the luteal phase, usually subsiding when your period starts and hormone levels drop.
Understanding the qualitative nature of this pain can help differentiate it from other conditions. Cyclical mastalgia is typically bilateral, meaning it affects both sides, though one breast may be noticeably more sensitive than the other. The discomfort often feels diffuse rather than localized to a precise, pinpoint spot. It is frequently accompanied by a granular or "rope-like" texture when palpated, which reflects the swollen lobular and fibrous tissue rather than an abnormal growth. Some individuals report heightened sensitivity to vibration, sudden movements, or even the brush of clothing. The pain can also be referred; because the upper outer quadrant of the breast shares nerve pathways with the axillary (underarm) region and the pectoral muscles, soreness may feel as though it extends into the shoulder, collarbone, or armpit. This referred pain is completely benign and stems from the dense innervation of the intercostobrachial nerve.
Tracking these sensations over several months can reveal a clear pattern. Keeping a simple symptom diary or using a cycle-tracking application allows you to map the onset, duration, and intensity of breast tenderness relative to your menstrual dates. Over time, this data helps establish your personal "baseline," making it easier to recognize when a deviation occurs that might warrant medical consultation.
Ovulation vs. PMS vs. Early Pregnancy: How to Tell the Difference
Because hormonal shifts are responsible for breast soreness in multiple scenarios, it can be difficult to pinpoint the cause based on this symptom alone. However, subtle differences in timing and accompanying symptoms can offer clues.
| Symptom Feature | Ovulation / PMS Soreness | Early Pregnancy Soreness |
|---|---|---|
| Timing | Starts mid-cycle (ovulation) or 1-2 weeks before your period (PMS). It resolves when or shortly after your period begins. | Starts around the time of a missed period or slightly before. It persists and may intensify instead of disappearing. |
| Sensation | Often a dull, heavy ache. Breast tissue may feel dense or "lumpy." | Frequently described as more intense, tingly, or sensitive. Breasts may feel fuller and heavier. |
| Other Symptoms | Accompanied by typical PMS symptoms like bloating, mood swings, food cravings, and headaches. | May be accompanied by a missed period, light spotting (implantation bleeding), nausea, fatigue, and darkening of the areolas. |
The physiological divergence between these states becomes apparent in the luteal phase. If fertilization does not occur, the corpus luteum degrades, progesterone plummets, and the menstrual cycle begins. The rapid withdrawal of progesterone and estrogen triggers the shedding of the uterine lining and simultaneously reduces breast tissue edema, which is why cyclical pain typically vanishes as bleeding starts.
In early pregnancy, however, the developing embryo implants into the uterine lining and begins producing human chorionic gonadotropin (hCG). hCG signals the corpus luteum to persist and continue pumping out progesterone at elevated levels. Sustained high progesterone, alongside rising estrogen and prolactin, drives continued mammary gland development and increased vascularity, which is why pregnancy-related breast tenderness not only lingers past the expected period date but often escalates in intensity. Some individuals notice prominent blue veins beneath the skin and darkening of the areolas (Montgomery's tubercles becoming more pronounced) as early as 3-4 weeks post-conception.
The most reliable way to determine if you are pregnant is to take a home pregnancy test after a missed period. Modern tests are highly sensitive to hCG and can typically detect pregnancy with 99% accuracy from the first day of a delayed period. Testing too early may result in a false negative, as hCG concentrations double approximately every 48 hours in early gestation.
Is Breast Soreness a Reliable Way to Track Ovulation?
While breast tenderness is linked to the hormonal events following ovulation, it is not considered a reliable method for tracking your fertile window. The American Pregnancy Association lists it as a secondary, less common symptom of ovulation [2].
The main reasons it's unreliable are:
- Timing: The pain typically starts after ovulation has already occurred, meaning you have already passed your most fertile days. The fertile window actually encompasses the five days leading up to ovulation plus the day of ovulation itself, as sperm can survive in the female reproductive tract for up to five days. Relying on post-ovulatory symptoms effectively misses the window for conception.
- Subjectivity: The experience and intensity of the pain are highly individual and can change from month to month. Factors like stress, travel, dietary changes, or illness can alter symptom perception, making it an inconsistent biomarker.
- Overlap: The symptom is too similar to PMS and early pregnancy signs to be a definitive indicator of ovulation. Without corroborating data, it's easy to misinterpret late-cycle soreness as PMS when it might actually indicate early pregnancy, or vice versa.
More Accurate Fertility Tracking Methods
For those trying to conceive, relying on primary fertility signs is far more effective:
- Ovulation Predictor Kits (OPKs): These tests detect the surge in luteinizing hormone (LH) that triggers ovulation. The LH surge typically occurs 24 to 36 hours before the follicle ruptures, providing a precise warning that your fertile window is closing. Digital OPKs can offer clearer interpretation and sometimes track estrogen trends alongside LH for enhanced accuracy.
- Basal Body Temperature (BBT) Charting: Tracking your temperature first thing in the morning can confirm that ovulation has occurred. Progesterone is thermogenic, causing a sustained temperature rise of approximately 0.5–1.0°F (0.3–0.6°C) that persists through the luteal phase. While excellent for confirming ovulation retrospectively, it doesn't predict the fertile window in advance, so it's best paired with OPKs.
- Cervical Mucus Monitoring: Observing changes in your cervical mucus throughout your cycle can help identify your most fertile days. Estrogen causes cervical fluid to transition from thick and sticky to clear, slippery, and stretchy (often compared to raw egg whites) as ovulation approaches. This "peak day" mucus provides an optimal environment for sperm survival and motility.
- Hormone Monitor Wearables & Apps: Emerging technology, including wearable fertility trackers and continuous hormone sensors, can measure luteinizing hormone, estrogen metabolites, and progesterone metabolites via urine or saliva, providing data-driven fertile window predictions that surpass traditional calendar methods.
 While breast soreness is a common symptom, more reliable methods like ovulation tests and temperature charting are recommended for accurate fertility tracking. Source: Mother & Baby
While breast soreness is a common symptom, more reliable methods like ovulation tests and temperature charting are recommended for accurate fertility tracking. Source: Mother & Baby
How to Manage and Relieve Ovulation Breast Pain
For many, cyclical breast pain is a manageable annoyance. If you're looking for relief, several lifestyle adjustments and home remedies can help. A multi-modal approach that addresses diet, physical support, and pain management pathways typically yields the best results.
Lifestyle and Home Remedies
- Wear a Supportive Bra: A well-fitting bra can significantly reduce discomfort by minimizing movement. During the luteal phase, breast volume can increase by up to a full cup size. Consider a supportive sports bra for exercise or even for sleeping if the pain is severe. Professional bra fitting every 6-12 months is highly recommended, as body shape and tissue density change over time.
- Apply Warm Compresses: A warm cloth or heating pad applied to the breasts can soothe aches and pains by increasing local blood circulation and relaxing tense pectoral muscles. For acute swelling, alternating with a cold pack (wrapped in a thin towel) can help constrict blood vessels and reduce inflammatory edema.
- Adjust Your Diet: Some evidence suggests that reducing intake of caffeine, salt, and high-fat foods in the two weeks before your period may lessen symptoms for some women. Caffeine can heighten nerve sensitivity and act as a mild diuretic that disrupts fluid balance, while excess sodium promotes water retention. Increasing consumption of anti-inflammatory foods, such as fatty fish rich in omega-3 fatty acids (salmon, mackerel), walnuts, flaxseeds, and leafy greens, can help modulate systemic inflammation and support healthy hormone metabolism.
- Consider Supplements: Some studies suggest that supplements like Vitamin E and magnesium may help, but you should always consult your doctor before starting any new supplement regimen. Evening primrose oil (EPO), which contains gamma-linolenic acid (GLA), has been traditionally used to alleviate cyclical breast pain by potentially altering prostaglandin pathways, though clinical trial results remain mixed. Vitamin B6 may also support hepatic estrogen metabolism. Dosages and efficacy vary, so medical guidance is essential to avoid interactions with other medications.
Medical Options
If the pain is severe and interferes with your daily life, over-the-counter anti-inflammatory medications like ibuprofen or naproxen can provide relief by inhibiting cyclooxygenase (COX) enzymes and reducing prostaglandin synthesis, which are key mediators of pain and inflammation. Topical NSAID gels can also be applied directly to the breast tissue, offering localized relief with minimal systemic absorption.
For persistent and debilitating cases, a doctor may discuss hormonal treatments, such as oral contraceptives, which can help regulate the hormonal fluctuations that cause the pain. By providing a steady, low-dose combination of synthetic estrogen and progestin, combined oral contraceptives prevent the natural mid-cycle hormone spikes that trigger cyclical mastalgia. In rare, refractory cases, a specialist might prescribe medications that modulate estrogen receptors or suppress ovarian function, though these are generally reserved for severe, quality-of-life-limiting cases due to potential side effects.
Additionally, some individuals find relief through complementary approaches like transcutaneous electrical nerve stimulation (TENS), acupuncture, or myofascial release therapy targeting the pectoralis major and minor muscles. Stress reduction is also critically important; chronic stress elevates cortisol, which can disrupt the hypothalamic-pituitary-ovarian axis, prolong the luteal phase, and exacerbate hormonal imbalances. Incorporating mindfulness practices, gentle yoga, or consistent moderate exercise can help maintain endocrine equilibrium and lower overall pain perception.
 Lifestyle adjustments and self-care can help manage cyclical breast discomfort. Source: Kiindred
Lifestyle adjustments and self-care can help manage cyclical breast discomfort. Source: Kiindred
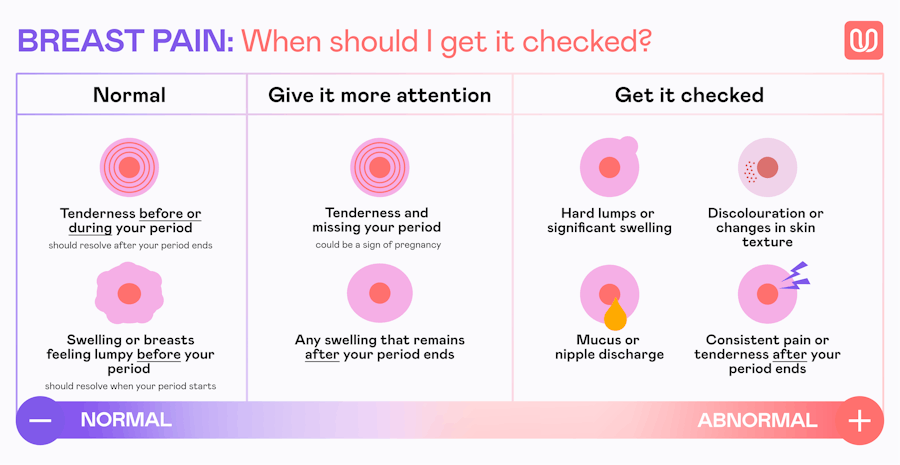
When to See a Doctor: Understanding 'Normal' vs. Atypical Symptoms
It's important to remember that cyclical breast pain is extremely common and rarely a sign of breast cancer. However, you should always consult a healthcare provider if you experience symptoms that deviate from the typical cyclical pattern. While hormonal fluctuations account for the vast majority of breast pain cases, non-cyclical pain (accounting for roughly one-third of clinical presentations) warrants a different diagnostic approach.
Seek medical advice if you notice:
- A new or changing lump in your breast or underarm that does not fluctuate with your menstrual cycle. While many lumps are benign cysts or fibroadenomas, any persistent mass requires clinical evaluation.
- Pain that is severe, persistent, or not related to your menstrual cycle (non-cyclical pain). Pain originating from musculoskeletal structures (costochondritis, muscle strain, or spinal nerve compression) or localized breast conditions often feels sharper and more localized.
- Pain localized to one specific spot rather than a general ache. Focal pain can sometimes indicate an underlying cyst, infection, or in rare cases, an inflammatory process that needs imaging.
- Skin changes on the breast, such as redness, dimpling, puckering, or an orange-peel texture (peau d'orange). These can be signs of underlying structural changes, infection, or, in rare instances, inflammatory breast cancer.
- Nipple changes, such as an inverted nipple or unusual discharge (especially if it's bloody, clear, spontaneous, and unilateral). Galactorrhea or bloody discharge requires prompt evaluation to rule out intraductal papillomas or pituitary issues.
- Signs of infection, like redness, warmth, swelling, and fever. Mastitis or abscesses can occur outside of breastfeeding due to cracked skin, bacterial entry, or underlying duct ectasia.
During a clinical evaluation, your provider will typically perform a thorough breast exam and review your personal and family medical history. Depending on your age and symptoms, imaging may be recommended. Ultrasound is often the first-line imaging modality for individuals under 30, as it excels at differentiating fluid-filled cysts from solid masses in dense breast tissue. For those over 30 or 40, a diagnostic mammogram combined with targeted ultrasound provides a comprehensive structural assessment. Understanding fibrocystic breast changes—a common, benign condition where breasts feel lumpy or rope-like due to hormonal stimulation—can also alleviate anxiety, as this condition mimics cyclical pain but often requires only monitoring and symptomatic management.
A healthcare professional can provide a proper evaluation and peace of mind. While cyclical soreness is a normal part of life for many, you should never hesitate to get checked if something feels wrong. Early consultation not only rules out pathological conditions but also opens the door to personalized pain management strategies tailored to your unique hormonal profile and lifestyle.
Frequently Asked Questions (FAQ)
Q: How many days does breast tenderness from ovulation last? A: Breast tenderness linked to ovulation can vary, but it typically starts a few days before ovulation and continues until your period begins. For many, the discomfort subsides or disappears once menstruation starts. Tracking your symptoms can help you identify your personal pattern. The duration usually spans 7 to 14 days, aligning with the luteal phase.
Q: Can only one breast hurt during ovulation? A: Yes, it is completely normal for cyclical breast pain to be more pronounced in one breast than the other. Hormonal changes affect your entire body, but the response in your breast tissue may not be perfectly symmetrical. Asymmetrical glandular distribution or localized fluid retention often explains the imbalance in sensitivity.
Q: Do breasts get bigger or swell during ovulation? A: Yes, some women experience noticeable breast swelling, fullness, or a feeling of heaviness around ovulation and in the days leading up to their period. This is caused by hormonal changes that lead to the growth of milk glands and increased blood flow to the area. Temporary size increases of up to a full cup size are not uncommon during peak progesterone days.
Q: Is it normal for nipple soreness to be the main symptom? A: Yes, for some individuals, the sensitivity is concentrated in the nipples rather than the entire breast. Sore, achy, or sensitive nipples are a common variation of cyclical breast pain and are caused by the same hormonal shifts. The nipples and areolae contain a high concentration of nerve endings and smooth muscle fibers that react strongly to estrogen and progesterone fluctuations.
Q: Does age affect how much breast soreness I feel during ovulation? A: Yes, symptom intensity can fluctuate throughout different life stages. Many people report increased sensitivity in their 30s due to changes in the ratio of glandular to fatty tissue. As perimenopause approaches and cycles become more erratic, breast pain can intensify due to unpredictable estrogen surges before eventually tapering off post-menopause when hormone levels stabilize at a lower baseline.
Q: Can exercise make ovulation breast pain worse? A: High-impact exercise without proper support can temporarily exacerbate discomfort by stretching the Cooper's ligaments. However, moderate aerobic activity and strength training can actually improve long-term hormone metabolism, reduce systemic inflammation, and alleviate PMS-related symptoms over time. Opting for low-impact activities like swimming, cycling, or walking during peak tenderness days is a practical compromise.
References
- Villines, Z. (2020). Sore nipples: Ovulation, pregnancy, or another cause? Medical News Today. https://www.medicalnewstoday.com/articles/sore-nipples-ovulation
- Mira Fertility. (2025). Do Breasts Hurt During Ovulation? (What to Expect when TTC). https://shop.miracare.com/blogs/resources/breasts-hurt-ovulation
- Johns Hopkins Medicine. Breast Pain (Mastalgia). https://www.hopkinsmedicine.org/health/conditions-and-diseases/mastalgia-breast-pain
- Clearblue. (2024). Five common ovulation questions and answers. https://www.clearblue.com/menstrual-cycle/5-common-ovulation-health-questions
- Health.com. (2025). Breast Changes 101: What To Expect During the Menstrual Cycle. Breast pain and changes during the menstrual cycle
- [News Source 1] Contemporary OB/GYN. (2025). Breast tenderness and swelling found in normal ovulation. https://www.contemporaryobgyn.net/view/breast-tenderness-and-swelling-found-in-normal-ovulation
Conclusion
Sore, swollen, or tender breasts around the time of ovulation are a widespread and fundamentally physiological response to the natural ebb and flow of reproductive hormones. Driven primarily by estrogen-induced ductal proliferation in the follicular phase and progesterone-driven lobular swelling and fluid retention in the luteal phase, this cyclical discomfort serves as a visible reminder of your body's intricate endocrine orchestration. While it can be unsettling or uncomfortable, cyclical mastalgia is rarely a sign of underlying pathology and frequently correlates with healthy, ovulatory cycles.
Understanding the distinction between normal hormonal soreness, PMS, and early pregnancy relies on recognizing timing, symptom trajectory, and accompanying signs. Breast tenderness alone, however, remains an imprecise tool for fertility tracking; those actively monitoring their fertile window will achieve far more reliable results by combining primary indicators like LH surge tests, basal body temperature charting, and cervical mucus observation. When discomfort disrupts daily life, a layered management approach—encompassing supportive garments, dietary modifications, targeted supplementation, stress reduction, and, when necessary, medical interventions—can provide substantial relief and improve quality of life.
Crucially, maintaining awareness of atypical symptoms ensures that normal cyclical changes are never confused with conditions requiring prompt clinical attention. By tracking patterns, listening to your body, and partnering with healthcare providers for persistent or atypical pain, you can navigate your reproductive health with confidence, clarity, and proactive self-care.

About the author
Sofia Rossi, MD, is a board-certified obstetrician-gynecologist with over 15 years of experience in high-risk pregnancies and reproductive health. She is a clinical professor at a top New York medical school and an attending physician at a university hospital.