When Are You Least Likely to Get Pregnant? A Comprehensive Guide

Key points
- Basal Body Temperature (BBT): Your BBT is your body's lowest resting temperature. It rises slightly (about 0.5°F or 0.3°C) after ovulation occurs due to the thermogenic effect of progesterone produced by the corpus luteum. It stays elevated until your next period or through early pregnancy. By tracking it daily using a specialized digital thermometer (measuring to one-tenth of a degree), you can confirm when ovulation has passed. For accurate readings, temperature must be taken immediately upon waking, before sitting up, talking, or drinking water, at roughly the same time each day. Factors like poor sleep quality, alcohol consumption the night prior, room temperature fluctuations, or illness can skew BBT readings, requiring users to note these disturbances on their charts.
- Cervical Mucus Monitoring: Your vaginal discharge changes throughout your cycle in response to fluctuating estrogen and progesterone levels. Following menstruation, you may experience dry days. As estrogen rises, mucus becomes creamy or lotion-like. As ovulation approaches, it becomes clear, slippery, stretchy, and abundant, like raw egg whites. This peak-quality mucus nourishes sperm, filters out abnormal cells, and facilitates transport through the cervix into the uterus. This indicates peak fertility. After ovulation, progesterone causes mucus to quickly thicken, become cloudy, sticky, or disappear entirely. Observing and recording these changes at least twice daily helps identify the shift from fertile to post-ovulatory infertile phases.
- Sympto-Thermal Method: This method combines BBT charting with cervical mucus monitoring for greater accuracy, often incorporating cervical position changes (the cervix softens, rises, and opens during fertility, then firms and drops post-ovulation). By cross-referencing multiple biomarkers, users can pinpoint ovulation more reliably than with single-sign methods. The fertile period begins when mucus changes indicate rising estrogen and ends three full days after the temperature shift is confirmed. With correct and consistent use, studies show its effectiveness can be as high as 99.6% for pregnancy prevention. However, typical use effectiveness drops to the 75-80% range due to inconsistent charting, misinterpretation of signs, or unprotected intercourse during uncertain transitional days. Learning this method properly typically requires formal instruction from a certified practitioner.
Understanding your menstrual cycle is essential whether you're trying to conceive or prevent pregnancy. While no time is 100% risk-free without a reliable form of contraception, there are specific phases in your cycle when you are significantly less likely to get pregnant. This guide synthesizes expert advice and clinical data to provide a comprehensive look at your fertility.
Understanding Your Menstrual Cycle and Fertility
The menstrual cycle is more than just your period; it's a complex hormonal process that prepares your body for a potential pregnancy each month. A typical cycle lasts about 28 days, but it's normal for it to range from 23 to 35 days. It's divided into four main phases:
- Menstrual Phase (Your Period): This is day 1 of your cycle, when the uterus sheds its lining.
- Follicular Phase: This phase starts on day 1 and lasts until ovulation. The brain signals the ovaries to prepare an egg for release.
- Ovulation: The release of a mature egg from an ovary. This is the peak of fertility and usually happens around day 14 in a 28-day cycle.
- Luteal Phase: This is the time after ovulation and before your next period. The body prepares the uterine lining for a fertilized egg. If pregnancy doesn't occur, the cycle restarts.
To fully grasp how your cycle operates, it is crucial to understand the endocrine system that governs it. The menstrual cycle is orchestrated by the hypothalamic-pituitary-ovarian (HPO) axis. The hypothalamus releases gonadotropin-releasing hormone (GnRH), which prompts the anterior pituitary gland to secrete follicle-stimulating hormone (FSH) and luteinizing hormone (LH). FSH stimulates the growth of ovarian follicles, each containing an immature egg. As these follicles mature, they produce increasing amounts of estradiol (a primary estrogen), which thickens the endometrial lining of the uterus. When estradiol levels reach a critical threshold, they trigger an LH surge that initiates ovulation. Following ovulation, the ruptured follicle transforms into the corpus luteum, which secretes progesterone. Progesterone stabilizes the uterine lining and inhibits further follicular development, effectively closing the fertile window until hormone levels drop and menstruation begins. Understanding this hormonal choreography clarifies why certain phases are naturally less fertile: without the presence of a mature egg or the precise hormonal environment required for implantation, conception is biologically improbable.
Your "fertile window" is the period when you are most likely to conceive. It includes the five days leading up to ovulation and the day of ovulation itself. This is because sperm can survive in the female reproductive tract for up to five days, and an egg is viable for about 12-24 hours after being released.
Beyond the standard 28-day model, cycle length varies significantly across the reproductive lifespan. Adolescents in the first few years post-menarche and perimenopausal individuals in their late 30s to 40s frequently experience irregular cycles due to fluctuating ovarian reserve and hormonal instability. Even healthy adults in their 20s and early 30s can experience natural cycle variations of several days month-to-month. These fluctuations mean that a calendar-based prediction of ovulation or "safe days" is inherently an estimate, not a guarantee. Modern digital period trackers use algorithms based on historical cycle data to predict ovulation, but they cannot account for real-time physiological shifts caused by acute illness, travel, psychological stress, or sudden changes in body composition. Consequently, relying solely on historical data to identify infertile days carries inherent risks, particularly for those seeking highly effective pregnancy prevention.
 Image Source: Flo.health
Image Source: Flo.health
Pinpointing the Times You Are Least Likely to Conceive
Based on the phases of the menstrual cycle, there are three distinct times when your chances of getting pregnant are at their lowest.
During Your Period (Menstrual Phase, Days 1-7)
This is generally considered the "safest" time of the month. The uterine lining is being shed, which makes it a hostile environment for a fertilized egg to implant. For most people, ovulation is still many days away. Additionally, the acidic pH of menstrual blood and the physical expulsion of blood and tissue create conditions that are generally unfavorable to sperm survival and upward motility. The cervix typically remains firm, closed, and lower in the vaginal canal during menstruation, further limiting sperm entry into the uterus.
However, the risk is not zero. Dr. Gina Frugoni, an OB/GYN at UC San Diego Health, confirms that while it's "not very likely, but still possible" to get pregnant during your period. This is especially true for individuals with shorter menstrual cycles (e.g., 21-24 days), as ovulation can occur much closer to the end of their period. According to research cited by Everlywell, the chance of getting pregnant on day 4 of your cycle is about 2%. Furthermore, irregular bleeding can sometimes be mistaken for a true menstrual period. Mid-cycle breakthrough bleeding, ovulation spotting, or bleeding related to cervical polyps, infections, or hormonal imbalances can occur during or near the actual fertile window, creating false confidence about safety.
Immediately After Your Period (Early Follicular Phase)
In the few days immediately following your period, the likelihood of pregnancy remains low because ovulation has not yet occurred. Estrogen levels are beginning to rise to stimulate follicular development, but the endometrial lining is still relatively thin, and cervical mucus typically remains thick, acidic, and impermeable to sperm. These physiological barriers naturally reduce the probability of conception during the first few days after menstruation concludes.
However, this window of low fertility can be very short. Because sperm can survive for up to five days, having unprotected sex during this time could lead to pregnancy if you ovulate earlier than expected. For example, if your period lasts seven days and you have unprotected intercourse on day eight, sperm could remain viable until day thirteen. If you experience an early ovulation due to hormonal fluctuation or stress on day twelve, fertilization could occur. Additionally, cycle tracking errors are common during this phase. Many individuals assume their period is shorter or longer than it actually is, or they miscalculate the start date (which is strictly defined as the first day of full, bright red flow, not light spotting or pre-menstrual discharge).
The Luteal Phase (After Ovulation, Before Your Next Period)
Once ovulation has occurred and the 12-24 hour window for fertilizing the egg has passed, you enter the luteal phase. During this time, your chances of getting pregnant are extremely low for the remainder of your cycle. If the egg is not fertilized, it disintegrates, and you cannot get pregnant until your next cycle begins. The luteal phase is typically the most predictable part of the menstrual cycle, lasting approximately 12 to 14 days in the vast majority of women, regardless of overall cycle length. Progesterone dominates this phase, causing cervical mucus to become thick, tacky, or absent, forming a physiological plug that prevents additional sperm from entering the uterus. The basal body temperature also remains elevated, providing a clear biological marker that the fertile window has closed.
The main challenge with relying on this phase is knowing with certainty that ovulation has already happened. Without consistent tracking of fertility biomarkers like BBT or cervical mucus patterns, individuals cannot definitively distinguish between the late follicular phase (approaching ovulation) and the true post-ovulatory phase. Relying on calendar predictions alone during this window is risky, as delayed ovulation pushes the actual infertile period later than anticipated. Furthermore, rare phenomena like secondary ovulation (the release of a second egg in the same cycle, typically within 24 hours of the first) or luteal phase defects (where progesterone production is insufficient) can complicate fertility calculations. While the post-ovulatory window is biologically the most reliable infertile period, it requires strict, methodical tracking to confirm ovulation has definitively concluded.
How to Identify Your Fertile and Infertile Days: Fertility Awareness-Based Methods (FABMs)
To more accurately identify your fertile window, you can use Fertility Awareness-Based Methods (FABMs). These involve tracking your body's natural fertility signals. However, experts like Dr. Kate O'Connell White of Boston University warn, "Using your cycle as a cheap birth control will get you pregnant. It's not something to take lightly." The effectiveness of FABMs hinges entirely on user consistency, proper education, and strict adherence to rules during fertile windows. When practiced perfectly, some methods rival hormonal contraceptives in efficacy, but real-world application often introduces human error.
If you choose to use FABMs, it's best to combine them and use them alongside a barrier method like condoms during fertile days or during periods of cycle uncertainty. Education from a certified fertility awareness instructor significantly improves success rates and reduces the learning curve associated with interpreting physiological signs.
Calendar Rhythm Method
This involves tracking the length of your menstrual cycles for several months to predict your fertile days. The Mayo Clinic notes this is one of the least effective forms of birth control, especially if your cycles are irregular. The classic Ogino-Knaus method calculates the fertile window by subtracting 18 days from the length of the shortest recorded cycle to find the first fertile day, and subtracting 11 days from the longest cycle to find the last fertile day. This statistical approach requires at least six to twelve months of accurate historical data to be mathematically valid. For a more modern approach, the Standard Days Method is for those with cycles between 26 and 32 days, identifying days 8-19 as fertile. Users of this method typically rely on a color-coded cycle bead system to track their position in the cycle. While simple to implement, the calendar rhythm method fails to account for real-time hormonal shifts, making it vulnerable to failure during months of stress, illness, or lifestyle changes.
Symptom-Based Methods (More Reliable)
These methods rely on observing daily, tangible changes in your body's reproductive physiology. They require dedication, a consistent daily routine, and careful recording of data points.
- Basal Body Temperature (BBT): Your BBT is your body's lowest resting temperature. It rises slightly (about 0.5°F or 0.3°C) after ovulation occurs due to the thermogenic effect of progesterone produced by the corpus luteum. It stays elevated until your next period or through early pregnancy. By tracking it daily using a specialized digital thermometer (measuring to one-tenth of a degree), you can confirm when ovulation has passed. For accurate readings, temperature must be taken immediately upon waking, before sitting up, talking, or drinking water, at roughly the same time each day. Factors like poor sleep quality, alcohol consumption the night prior, room temperature fluctuations, or illness can skew BBT readings, requiring users to note these disturbances on their charts.
- Cervical Mucus Monitoring: Your vaginal discharge changes throughout your cycle in response to fluctuating estrogen and progesterone levels. Following menstruation, you may experience dry days. As estrogen rises, mucus becomes creamy or lotion-like. As ovulation approaches, it becomes clear, slippery, stretchy, and abundant, like raw egg whites. This peak-quality mucus nourishes sperm, filters out abnormal cells, and facilitates transport through the cervix into the uterus. This indicates peak fertility. After ovulation, progesterone causes mucus to quickly thicken, become cloudy, sticky, or disappear entirely. Observing and recording these changes at least twice daily helps identify the shift from fertile to post-ovulatory infertile phases.
- Sympto-Thermal Method: This method combines BBT charting with cervical mucus monitoring for greater accuracy, often incorporating cervical position changes (the cervix softens, rises, and opens during fertility, then firms and drops post-ovulation). By cross-referencing multiple biomarkers, users can pinpoint ovulation more reliably than with single-sign methods. The fertile period begins when mucus changes indicate rising estrogen and ends three full days after the temperature shift is confirmed. With correct and consistent use, studies show its effectiveness can be as high as 99.6% for pregnancy prevention. However, typical use effectiveness drops to the 75-80% range due to inconsistent charting, misinterpretation of signs, or unprotected intercourse during uncertain transitional days. Learning this method properly typically requires formal instruction from a certified practitioner.
Important Factors That Influence Your Chances of Pregnancy
Your cycle is not the only thing that matters. Several other factors play a significant role in modulating fertility and the reliability of cycle-based tracking.
The Critical Role of Cycle Regularity
For individuals with irregular periods, predicting the fertile window is extremely difficult. Stress, illness, travel, and hormonal conditions can all disrupt your cycle, making calendar-based methods highly unreliable. If your cycle is irregular, relying on "safe days" is not a recommended method of contraception. Conditions such as Polycystic Ovary Syndrome (PCOS) disrupt normal follicular development and ovulation, leading to prolonged follicular phases, unpredictable bleeding, and sporadic anovulatory cycles. Thyroid disorders (both hypothyroidism and hyperthyroidism), elevated prolactin levels, premature ovarian insufficiency, and extreme athletic training or eating disorders can similarly suppress or dysregulate ovulation. When ovulation is delayed or absent, the traditional 28-day framework becomes irrelevant, and the luteal phase cannot be reliably projected. In such cases, hormonal bloodwork (FSH, LH, estradiol, progesterone, TSH, and prolactin) and pelvic ultrasound may be necessary to assess reproductive health. Until underlying imbalances are addressed, cycle-based fertility prediction remains highly inaccurate.
It's Not Just About the Egg: Sperm Viability Matters
A key reason the fertile window is several days long is that sperm can survive in the reproductive tract for up to five days. Male fertility is also crucial. A man's lifestyle and health can impact sperm viability, directly influencing the probability of conception regardless of timing.
- Lifestyle: Smoking and heavy alcohol consumption are linked to lower sperm counts, reduced motility, and increased DNA fragmentation in sperm, which can lead to early miscarriage or failed implantation. Illicit drug use, particularly anabolic steroids, can shut down natural testosterone production and spermatogenesis entirely.
- Heat: Spermatogenesis requires a temperature roughly 2-4°C cooler than core body temperature. Exposure to high temperatures from saunas, hot tubs, or even prolonged sitting with a laptop on the lap can temporarily impair sperm production and quality. This thermal sensitivity is why wearing loose-fitting underwear is often recommended for men trying to optimize fertility.
- Environmental Factors: Exposure to endocrine-disrupting chemicals (EDCs) like bisphenol-A (BPA), phthalates, pesticides, heavy metals (lead, cadmium), and industrial solvents can alter hormonal signaling and harm sperm development. Occupational exposures and certain medications (e.g., chemotherapy, some antibiotics, testosterone replacement therapy) can also cause temporary or permanent male factor infertility. Understanding these variables emphasizes that pregnancy prevention or conception planning is a shared responsibility. Male factor infertility accounts for approximately 30-40% of reproductive challenges, making comprehensive reproductive health awareness essential.
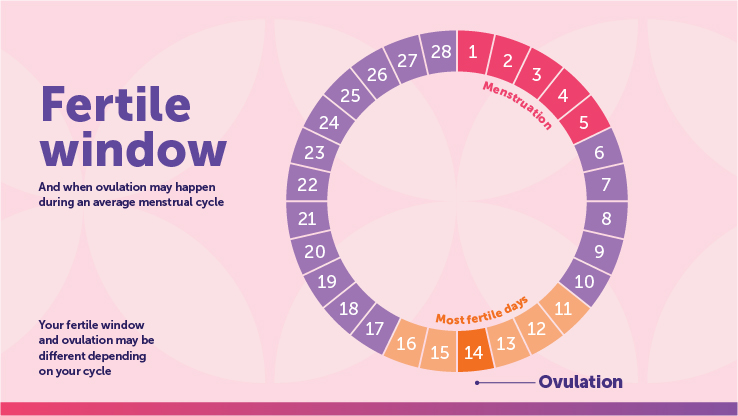 Image Source: HealthPartners
Image Source: HealthPartners
Age and Fertility: A Nuanced Look
While it's widely known that fertility declines with age, the idea of a "fertility cliff" at age 35 is a misconception. According to a detailed report by the BBC, the decline is gradual. It begins to speed up in the late 30s, with a more significant drop after age 40. Female fertility is fundamentally tied to the ovarian reserve, which peaks before birth and declines steadily throughout life. Unlike men who continuously produce new sperm, women are born with all the oocytes they will ever have. Over time, both the quantity and chromosomal quality of these eggs diminish. By age 35, the rate of chromosomal abnormalities in eggs increases, raising the risk of miscarriage and conditions like Down syndrome. However, many women in their mid-to-late 30s conceive naturally without difficulty, particularly if they have regular ovulatory cycles and no underlying reproductive pathology.
Male fertility also declines with age, typically starting in the late 30s, though men remain biologically capable of fathering children well into later adulthood. Advanced paternal age (generally considered over 40 or 45) is associated with decreased semen volume, reduced sperm motility, increased DNA fragmentation, and slightly higher risks of neurodevelopmental conditions in offspring. These age-related changes occur gradually rather than abruptly. For individuals planning pregnancies or assessing contraceptive timelines, understanding the biological reality of aging gametes is crucial. Those who anticipate delaying childbearing into their late 30s or 40s may benefit from preconception counseling, ovarian reserve testing (AMH, antral follicle count), and discussions about fertility preservation options like egg or embryo cryopreservation.
Body Weight, Nutrition, and Metabolic Health
Body composition significantly impacts reproductive hormone balance. Adipose tissue is metabolically active and participates in estrogen production. Both underweight (BMI < 18.5) and obese (BMI > 30) individuals frequently experience menstrual irregularities or anovulation. Excess adipose tissue can lead to insulin resistance and hyperinsulinemia, which stimulate ovarian androgen production and disrupt normal follicular maturation, commonly seen in PCOS. Conversely, extremely low body fat or severe caloric restriction signals metabolic distress to the hypothalamus, reducing GnRH pulsatility and potentially causing functional hypothalamic amenorrhea. Adequate nutrition, including sufficient healthy fats, complex carbohydrates, and essential micronutrients like folate, iron, vitamin D, and omega-3 fatty acids, supports healthy hormone synthesis and endometrial development. Maintaining a balanced diet, managing chronic stress, and engaging in moderate, consistent exercise rather than extreme training regimens optimizes cycle regularity and enhances the reliability of fertility tracking methods.
The Most Reliable Ways to Prevent Pregnancy
While understanding your cycle is empowering, Fertility Awareness-Based Methods have a higher failure rate with typical use than other forms of contraception. If preventing pregnancy is your priority, consider more reliable methods:
- Long-Acting Reversible Contraceptives (LARCs): IUDs and hormonal implants are over 99% effective. Levonorgestrel-releasing IUDs thicken cervical mucus and thin the endometrial lining, while copper IUDs create a localized inflammatory environment that is spermicidal. Hormonal implants (like etonogestrel rods) steadily release progestin to inhibit ovulation. LARCs require minimal user compliance, making them highly effective across diverse lifestyles and eliminating daily tracking or pharmacy refills.
- Hormonal Methods: Birth control pills, patches, and vaginal rings are up to 93% effective with typical use. These methods prevent pregnancy by suppressing the HPO axis, thickening cervical mucus, and altering the endometrium. Consistency is key; missing pills, delayed patch changes, or ring displacement can reduce efficacy. Newer progestin-only options, including the "mini-pill" and subcutaneous injections, offer alternatives for those who cannot tolerate estrogen.
- Barrier Methods: Condoms are 87% effective with typical use and have the added benefit of protecting against STIs. Diaphragms and cervical caps used with spermicide require proper fitting by a healthcare provider and correct placement before intercourse. While barrier methods are less effective at pregnancy prevention alone compared to LARCs, they remain vital for comprehensive sexual health and are often used in conjunction with other methods.
In addition to routine contraception, emergency contraception (EC) serves as a critical backup for contraceptive failure, missed pills, or unprotected intercourse during unexpected fertile windows. Levonorgestrel-based EC pills are most effective when taken within 72 hours, though efficacy diminishes with time and higher body weight. Ulipristal acetate (ella) remains effective up to 120 hours and works better for individuals with higher BMI. The copper IUD is the most effective form of emergency contraception, preventing pregnancy when inserted within 5 days of unprotected sex and providing ongoing highly effective birth control.
Consult with a healthcare provider to discuss the best and most effective contraception options for your body and lifestyle. A comprehensive reproductive health evaluation considers medical history, cardiovascular risk factors, medication interactions, future family planning goals, and personal preferences. Combining methods—such as using condoms alongside a hormonal pill or tracking fertility while on a progestin-only method—provides layered protection, maximizes STI prevention, and builds confidence in your reproductive autonomy.
References
- Mayo Clinic. (2023). Rhythm method for natural family planning.
- Medical News Today. (2021). Safe days for not getting pregnant: Ovulation and more.
- USA Today. (2024). Can you actually get pregnant during your period?
- BBC Future. (2024). Women's fertility is more complicated than you might have heard.
- Utah Department of Health & Human Services. Do you know what your chances of getting pregnant really are?
Frequently Asked Questions
Can I get pregnant if I have sex right after my period ends?
Yes, pregnancy is possible in the days immediately following your period. Sperm can survive inside the female reproductive tract for up to five days under optimal conditions. If you have a shorter cycle (around 21-24 days) or experience an early ovulation due to hormonal fluctuations, sperm deposited just after menstruation may still be viable when the egg is released. Additionally, what appears to be a period might sometimes be mid-cycle spotting or irregular bleeding, which can coincide with actual fertile days. While the statistical probability is lower immediately post-menstruation compared to mid-cycle, it is never zero. Relying on this timing as primary contraception carries a measurable risk, particularly if you do not actively track ovulation signs like basal body temperature or cervical mucus quality.
How accurate are period tracking apps at predicting safe days?
Period tracking apps vary widely in accuracy depending on their underlying algorithm and the quality of user data input. Most consumer apps rely on historical calendar data and statistical averages to predict ovulation, assuming a standard luteal phase and symmetrical follicular development. While these apps are highly useful for awareness and logging symptoms, they cannot detect real-time physiological shifts caused by acute stress, illness, travel, medication changes, or hormonal imbalances. Studies have shown that algorithm-based predictions frequently miscalculate the fertile window in women with irregular cycles or those experiencing delayed ovulation. Some FDA-approved fertility awareness devices incorporate wearable sensors, heart rate variability, or continuous temperature tracking to improve accuracy, but even these require strict user compliance and are generally more effective at confirming ovulation after it happens rather than predicting it in advance. Apps should be used as educational and organizational tools rather as standalone contraceptive methods.
Does having a long or short cycle change when I'm least fertile?
Absolutely. Cycle length directly alters the timing and duration of the fertile and infertile windows. In a short cycle (e.g., 21-24 days), ovulation occurs earlier, sometimes around day 7-10, meaning the post-menstrual "safe" period is drastically shortened or virtually nonexistent. In longer cycles (e.g., 32-40 days), the follicular phase is prolonged, delaying ovulation and extending the pre-ovulatory infertile window. However, longer cycles are more prone to irregularity and anovulatory months, making calendar predictions highly unreliable regardless of length. The luteal phase remains relatively consistent at 12-14 days in most individuals, so the post-ovulatory infertile period is actually more predictable in longer cycles once ovulation is confirmed. Ultimately, cycle length dictates when fertility begins and ends, emphasizing that a one-size-fits-all calendar approach is inadequate for personalized pregnancy prevention.
Can stress or illness shift my ovulation and make "safe" days risky?
Yes, physiological and psychological stressors significantly impact the hypothalamic-pituitary-ovarian axis. Acute stress, severe illness, high fever, surgery, significant travel, sleep deprivation, and extreme emotional events can delay or even suppress ovulation. When ovulation is delayed, the follicular phase extends, and the expected "safe" pre-ovulatory days become fertile. If you rely on a standard calendar and assume ovulation will occur on day 14, a stress-induced delay to day 21 means unprotected intercourse on day 15 could result in pregnancy, as sperm would survive until ovulation occurs. Conversely, chronic high stress or extreme weight loss can cause anovulatory cycles, where no egg is released at all, but irregular bleeding may still occur, creating confusion about cycle phase. Because these variables are unpredictable, stress and illness inherently undermine the reliability of cycle-based contraception, making backup methods essential during uncertain periods.
What should I do if I'm trying to avoid pregnancy but my cycles are irregular?
If your cycles are irregular, relying on calendar tracking or assuming specific days are safe is strongly discouraged by medical professionals. Irregularity indicates unpredictable or absent ovulation, meaning the traditional framework of a fertile window does not apply consistently. In this scenario, you have several medically sound options: 1) Consult a healthcare provider to investigate underlying causes of irregularity, such as PCOS, thyroid dysfunction, hyperprolactinemia, or metabolic imbalances. 2) Consider using a highly effective, non-cycle-dependent contraceptive method such as a copper or hormonal IUD, contraceptive implant, or consistent use of condoms. 3) If you are determined to use a fertility awareness method, seek instruction in a symptom-based approach (like the Sympto-Thermal Method or Creighton Model) from a certified educator, and commit to using barrier methods or abstaining on all days until multiple biomarkers confirm you are post-ovulatory. 4) Always keep emergency contraception accessible as a backup for unprotected intercourse or contraceptive failure. Managing irregular cycles requires a proactive, individualized reproductive health plan developed in partnership with a clinician.
Conclusion
Understanding when you are least likely to get pregnant requires a deep appreciation of your menstrual cycle's hormonal complexity, physiological markers, and inherent variability. While the days during menstruation, immediately following your period, and well into the luteal phase naturally present lower conception probabilities, none of these periods offer absolute protection without reliable contraception. Biological factors like sperm longevity, cycle irregularity, stress, age, and lifestyle continuously influence fertility in ways that calendar estimates cannot accurately capture. Fertility Awareness-Based Methods can empower individuals with intimate knowledge of their reproductive health, but they demand rigorous education, consistent tracking, and disciplined adherence to avoid unintended pregnancy. For those prioritizing highly effective pregnancy prevention, modern contraceptives like LARCs, hormonal methods, and dual-protection strategies provide superior reliability and peace of mind. Ultimately, reproductive planning is deeply personal. By combining accurate physiological awareness with evidence-based medical guidance, you can make informed decisions that align with your health, lifestyle, and family planning goals. Always consult a qualified healthcare provider to tailor contraceptive strategies to your unique biology and ensure comprehensive reproductive care.

About the author
Sofia Rossi, MD, is a board-certified obstetrician-gynecologist with over 15 years of experience in high-risk pregnancies and reproductive health. She is a clinical professor at a top New York medical school and an attending physician at a university hospital.