Pink Eye vs. Allergies: Symptoms, Causes, and Treatment

Key points
- Infectious Conjunctivitis (Pink Eye): Caused by a viral or bacterial infection. This type is contagious. Pathogens invade the conjunctival epithelium, triggering a localized immune response that results in cellular exudation and increased mucous production. The severity often correlates with the specific strain and the host's immune competence.
- Allergic Conjunctivitis: Caused by an allergic reaction to substances like pollen, pet dander, or dust. This type is not contagious. It involves a Type I hypersensitivity reaction where mast cells in the conjunctiva release histamine and other inflammatory mediators upon allergen exposure.
- Irritant Conjunctivitis: Caused by exposure to irritants like smoke, chlorine, or chemicals. This type is also not contagious. Unlike allergic responses, irritant conjunctivitis is a direct physical or chemical reaction that does not involve the adaptive immune system, though it produces remarkably similar clinical symptoms due to mechanical tissue disruption.
Waking up to red, itchy, and watery eyes can be alarming and uncomfortable. The immediate question is often: Is it contagious pink eye or just allergies? While both conditions cause inflammation of the conjunctiva—the thin membrane covering your eye and inner eyelid—they stem from different causes and require different treatments. Misdiagnosing the condition at home can lead to unnecessary spread of infection, prolonged discomfort, or delayed treatment for more serious underlying issues. In an era where health information is readily available but often conflicting, understanding the nuanced differences between these two common eye conditions is essential for proper self-care and knowing when to seek professional medical intervention.
This comprehensive guide will help you understand the key differences in symptoms, causes, and treatments for pink eye and allergies, explore other conditions that can mimic them, and know when it's time to see a doctor. By breaking down the medical science, clinical presentation, and practical management strategies, you will be equipped to make informed decisions about your eye health and protect those around you from potential exposure to contagious pathogens.
What is Conjunctivitis? The Common Ground
Both pink eye and eye allergies are forms of conjunctivitis. This condition occurs when the conjunctiva becomes inflamed, causing the tiny blood vessels within it to become more visible, giving the eye a pink or reddish color. The conjunctiva serves as a critical protective barrier, producing tears and mucus to keep the eye moist, deliver essential nutrients, and trap foreign particles before they reach the cornea. When this delicate tissue becomes irritated, the body’s inflammatory response kicks in, leading to vasodilation, increased vascular permeability, and the classic clinical signs of redness, swelling, tearing, and discharge. According to the CDC, there are three to six million cases in the US annually, making it one of the most frequently diagnosed ocular conditions in both pediatric and adult populations.
The cause of this inflammation is what separates these conditions:
- Infectious Conjunctivitis (Pink Eye): Caused by a viral or bacterial infection. This type is contagious. Pathogens invade the conjunctival epithelium, triggering a localized immune response that results in cellular exudation and increased mucous production. The severity often correlates with the specific strain and the host's immune competence.
- Allergic Conjunctivitis: Caused by an allergic reaction to substances like pollen, pet dander, or dust. This type is not contagious. It involves a Type I hypersensitivity reaction where mast cells in the conjunctiva release histamine and other inflammatory mediators upon allergen exposure.
- Irritant Conjunctivitis: Caused by exposure to irritants like smoke, chlorine, or chemicals. This type is also not contagious. Unlike allergic responses, irritant conjunctivitis is a direct physical or chemical reaction that does not involve the adaptive immune system, though it produces remarkably similar clinical symptoms due to mechanical tissue disruption.
Understanding the underlying pathophysiology is crucial because it dictates the treatment pathway. While allergic and irritant conjunctivitis share overlapping symptoms with infectious forms, their management diverges significantly. For instance, antihistamines are highly effective for allergic responses but do nothing to combat bacterial replication or viral shedding. Similarly, applying antibiotic ointment to an allergic reaction provides zero therapeutic benefit and may even exacerbate irritation due to preservatives in the formulation.
Pink Eye vs. Allergies: Key Symptom Differences
Distinguishing between infectious pink eye and allergies often comes down to a few key symptoms. While there can be overlap, paying attention to the details can provide important clues. Clinical presentation often varies depending on the patient’s age, immune status, and the specific pathogen or allergen involved. Children may present with more pronounced swelling, fussiness, and reluctance to open their eyes in bright light, while adults often report a gritty, foreign-body sensation that severely interferes with screen time, driving, or reading. The temporal progression of symptoms also offers diagnostic value: allergic flares typically follow a predictable seasonal or environmental pattern, whereas infectious cases often escalate rapidly over 24 to 72 hours.
Here’s a side-by-side comparison to help you tell them apart:
| Symptom | Allergic Conjunctivitis | Infectious Pink Eye (Viral/Bacterial) |
|---|---|---|
| Itching | Intense and persistent. This is a hallmark symptom. The itch often feels deep within or just beneath the eyelid, prompting constant rubbing that can worsen inflammation and potentially cause corneal micro-abrasions. | Mild to moderate. Patients often describe a burning, stinging, or gritty sensation rather than true pruritus. |
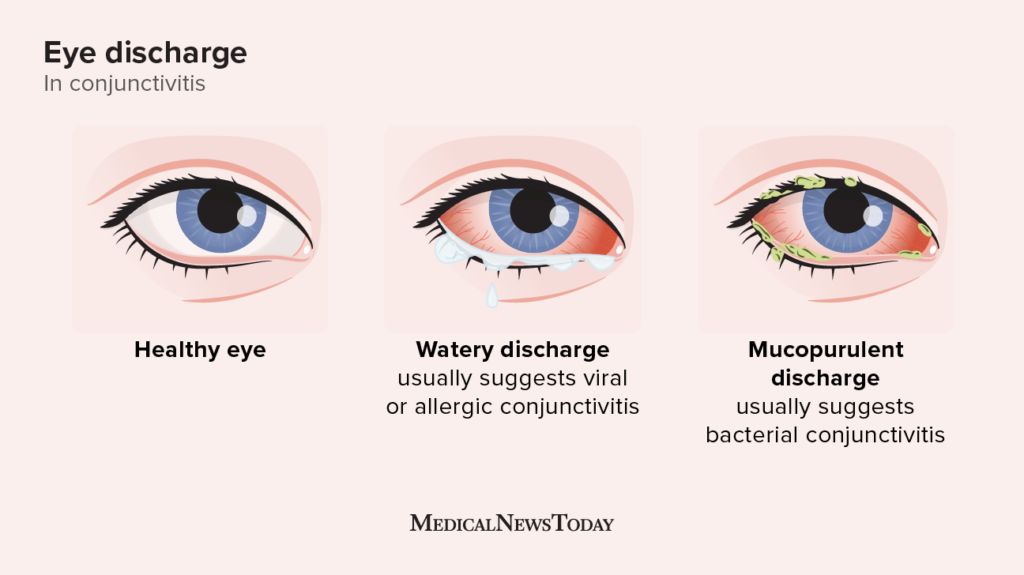
| Discharge | Clear, watery, or stringy white mucus. The discharge rarely crusts heavily and typically clears up with blinking or the application of preservative-free artificial tears. | Viral: Watery discharge that may become slightly mucoid as the infection progresses. Bacterial: Thick, yellow, green, or white pus that can cause eyelids to crust and stick together, especially upon waking. |
| Eye Involvement | Usually affects both eyes at the same time. Allergens circulate in the air or contact both ocular surfaces nearly simultaneously, leading to bilateral presentation. | Often starts in one eye and may spread to the other within a few days. Unilateral onset is a classic diagnostic clue for infectious etiologies, as pathogens are frequently transferred by hand-rubbing one eye before touching the other. |
| Other Symptoms | Often accompanied by sneezing, a runny or stuffy nose, and a history of seasonal allergies. May also include itchy skin, nasal congestion, throat irritation, and fatigue due to poor sleep from nocturnal itching. | Viral: May occur with cold, flu, or sore throat symptoms, along with tender preauricular lymph nodes. Bacterial: Can sometimes accompany an ear infection (otitis-conjunctivitis syndrome), particularly in young children under age 5. |
| Eyelid Appearance | Often puffy and swollen. The swelling is usually soft, diffuse, and bilateral, with minimal to no crusting around the lashes. | Eyelids can be swollen. With bacterial infections, they are often crusted or matted shut. Periorbital edema may be more localized, firm, and tender to the touch. |
| Contagiousness | Not contagious. Safe to attend school, work, or public spaces, though visibility and comfort may be temporarily compromised. | Highly contagious. Viral strains remain contagious as long as symptoms persist, while bacterial strains typically lose contagion after 24 hours of consistent antibiotic therapy. |
Diving Deeper: Causes and Triggers
Infectious Pink Eye (Viral and Bacterial)
Commonly known as "pink eye," this condition is an infection that can spread easily through direct contact or contaminated surfaces. Understanding the microbiology behind these infections helps explain why certain environments, like schools, daycare centers, nursing homes, and open-plan offices, become hotspots for rapid outbreaks. Poor ventilation, shared communal items, and inadequate hand hygiene create ideal conditions for pathogen transmission.
- Viral Conjunctivitis: This is the most common type and is highly contagious. It's often caused by the same viruses responsible for the common cold and sore throat, most notably adenoviruses, which account for up to 90% of viral cases. Other culprits include herpes simplex virus (HSV), varicella-zoster virus, and enteroviruses. Viral conjunctivitis typically presents with watery eyes, photophobia, and preauricular lymph node swelling. The incubation period ranges from 5 to 12 days, and patients can remain contagious for up to two weeks. Epidemic keratoconjunctivitis (EKC), a severe adenoviral strain, can lead to corneal infiltrates and prolonged visual disturbances requiring specialist management.
- Bacterial Conjunctivitis: This type is caused by bacteria like Staphylococcus aureus or Streptococcus pneumoniae, as well as Haemophilus influenzae and Moraxella catarrhalis. It is also very contagious and can be transmitted through direct contact with an infected person's eye discharge, respiratory droplets, or contaminated surfaces like doorknobs, shared towels, swimming pool areas, or improperly sanitized makeup applicators. Bacterial forms tend to progress rapidly, with purulent discharge peaking within 48 hours of symptom onset. Hyperacute bacterial conjunctivitis caused by Neisseria gonorrhoeae is rare but medical emergency, presenting with copious purulent discharge and rapid corneal melting within 24-48 hours.
Allergic Conjunctivitis
This condition is a direct result of your body's immune system overreacting to a harmless substance, or allergen. When an allergen comes into contact with your eyes, your body releases histamines, which cause inflammation, itching, and watering. The pathophysiology involves IgE antibodies binding to mast cells on the conjunctival surface. Upon re-exposure, these cells degranulate, releasing histamine, leukotrienes, and prostaglandins that cause vasodilation, increased vascular permeability, and direct nerve stimulation. This rapid-phase response typically occurs within minutes of exposure, while a late-phase response involving eosinophils and lymphocytes can cause symptoms to linger for hours or days.
Allergic conjunctivitis is categorized into two main subtypes:
- Seasonal Allergic Conjunctivitis: Triggered by outdoor allergens that fluctuate with the weather and regional pollen counts. Symptoms typically spike during spring (tree pollen), summer (grass pollen), and fall (weed pollen).
- Perennial Allergic Conjunctivitis: Persists year-round and is driven by indoor allergens that remain consistently present in the living environment.
Common triggers include:
- Outdoor allergens: Pollen from trees, grass, and weeds.
- Indoor allergens: Dust mites, pet dander, and mold spores.
- Irritants: Perfume, cosmetics, vehicle exhaust, and secondhand smoke.
Environmental factors such as wind, low humidity, and high pollution levels can significantly exacerbate both viral spread and allergic responses. For instance, dry eyes compromise the tear film’s protective mucin and lipid layers, making the conjunctiva more vulnerable to airborne allergens and pathogens. Heating and air conditioning systems, if poorly maintained or equipped with dirty filters, can recirculate dust mites, pet dander, and mold spores throughout the home. Additionally, wearing contact lenses during high-allergen days can trap irritants directly against the ocular surface, intensifying the inflammatory cascade.
Treatment and Relief Strategies
The right treatment depends entirely on the cause. Using the wrong approach can be ineffective and may prolong discomfort or lead to complications. Self-management strategies should always align with clinical guidelines, be tailored to the individual's medical history, and be adjusted promptly if symptoms persist or worsen.
Treating Allergic Conjunctivitis
The goal is to reduce inflammation, break the histamine-driven inflammatory cascade, and restore ocular surface comfort.
- Avoid Triggers: The most effective step is to minimize exposure to your known allergens. Stay indoors on high-pollen days, keep windows and doors closed, use a HEPA air purifier in frequently used rooms, and wash your hands and face after petting animals. Shower and change clothes after outdoor activities to remove settled pollen. Frequently wash bedding in hot water (at least 130°F) to eliminate dust mites, and consider using allergen-proof mattress and pillow encasements.
- Cool Compresses: Applying a cool, damp cloth to your eyes can soothe itching and reduce swelling. Cold therapy causes localized vasoconstriction, temporarily limiting histamine and inflammatory mediator delivery to the conjunctival tissue and providing immediate, drug-free symptomatic relief.
- Over-the-Counter (OTC) Relief:
- Artificial Tears: These eye drops can help flush allergens from your eyes, dilute inflammatory mediators, and restore the tear film. Preservative-free formulations are highly recommended for frequent use (more than four times daily) to prevent chemical toxicity from preservatives like benzalkonium chloride.
- Antihistamines: Oral antihistamines (like Zyrtec, Claritin, or Allegra) or topical antihistamine eye drops can provide significant relief from itching. Second-generation antihistamines are preferred due to their lower risk of sedation and longer duration of action.
- Mast Cell Stabilizers & Dual-Action Agents: Drops containing ketotifen, olopatadine, or azelastine prevent mast cell degranulation while also blocking histamine receptors. They are highly effective and work best when used prophylactically before anticipated allergen exposure.
- Prescription Treatments: For severe, chronic, or treatment-resistant symptoms, a doctor may recommend prescription-strength eye drops containing short-acting corticosteroids (for acute flare-ups, with strict monitoring to prevent glaucoma or cataract formation), immunomodulators like cyclosporine, or long-term allergen immunotherapy (sublingual drops or allergy shots) for systemic desensitization.
Treating Infectious Pink Eye
For infectious pink eye, the focus is on easing symptoms, supporting the immune system, preventing complications, and strictly halting transmission to others or your own unaffected eye.
- Viral Pink Eye: Since antibiotics don't work on viruses, treatment focuses on supportive care and immune system support. It typically resolves on its own in 7 to 14 days. Warm compresses can help soften and clean away crusts, while chilled artificial tears can soothe surface irritation. In severe adenoviral cases, an ophthalmologist might prescribe mild topical corticosteroids to reduce severe stromal inflammation and prevent subepithelial corneal infiltrates, though this requires careful monitoring of intraocular pressure.
- Bacterial Pink Eye: A doctor will likely prescribe antibiotic eye drops or ointment such as polymyxin-trimethoprim, erythromycin, azithromycin, or fluoroquinolones like moxifloxacin. It's crucial to complete the full prescribed course of medication even if symptoms improve rapidly, to prevent the infection from recurring and to minimize the risk of antimicrobial resistance. Symptoms usually improve markedly within 24 to 48 hours of starting treatment.
- Hygiene is Critical: To avoid spreading the infection to others or your other eye:
- Wash your hands frequently and thoroughly with soap and warm water for at least 20 seconds, especially before and after touching your face or applying eye medication.
- Avoid touching or rubbing your eyes. If you must apply medication, wash your hands meticulously and use a clean cotton swab if needed to remove discharge before instilling drops.
- Do not share towels, washcloths, pillowcases, or eye makeup. Discard any mascara, liquid eyeliner, or eye creams used while infected to eliminate bacterial reservoirs.
- Temporarily stop wearing contact lenses until a doctor says it's safe. Dispose of your current lenses, disinfect rigid lenses per protocol, and thoroughly clean or replace your contact lens case. Daily disposable lenses are generally recommended during recovery to prevent reinfection and biofilm buildup.
When It's Not Pink Eye or Allergies: Other Possibilities
Sometimes, red and irritated eyes aren't caused by allergies or a typical infection. Several other conditions can present with similar symptoms, making clinical evaluation essential for accurate management. Misdiagnosis can delay critical interventions, particularly for sight-threatening or autoimmune-mediated conditions.
- Dry Eye Syndrome (DES): A chronic lack of sufficient lubrication and tear film stability on the surface of the eye, causing a gritty sensation, intermittent redness, and fluctuating blurry vision. DES is often exacerbated by prolonged digital screen use, aging, hormonal changes, autoimmune disorders (like Sjögren’s syndrome or rheumatoid arthritis), and certain medications (antihistamines, antidepressants, beta-blockers, isotretinoin). Unlike infectious conjunctivitis, DES lacks significant purulent discharge and typically worsens progressively throughout the day rather than presenting with heavy morning crusting. Management includes environmental modifications, warm compresses, lid massage, omega-3 fatty acid supplementation, punctal plugs, and prescription anti-inflammatory drops (like lifitegrast or cyclosporine).
- Blepharitis: Chronic inflammation of the eyelid margins, leading to redness, itching, and dandruff-like scales or greasy crusts at the base of the eyelashes. It is frequently associated with Demodex mite colonization, seborrheic dermatitis, rosacea, or meibomian gland dysfunction (MGD). Patients often report persistent burning, foreign-body sensation, chronic dry eye, and eyelash misdirection. Treatment involves daily warm compresses to melt hardened meibomian secretions, meticulous eyelid hygiene with commercial hypochlorous acid wipes or diluted baby shampoo, and sometimes topical or oral antibiotics for secondary bacterial overgrowth.
- Iritis (Anterior Uveitis): Inflammation of the iris and anterior chamber, which can cause deep, aching eye pain, significant light sensitivity (photophobia), and a distinct pattern of redness. The redness often appears as a violet or brownish ring immediately surrounding the iris (ciliary flush) rather than the diffuse pinkness seen in conjunctivitis. This condition is strongly associated with autoimmune diseases (ankylosing spondylitis, psoriatic arthritis, inflammatory bowel disease, sarcoidosis) and requires prompt medical attention to prevent synechiae (adhesions between the iris and lens), secondary glaucoma, cataract formation, and permanent vision loss.
- Keratitis: Inflammation of the cornea, which can be infectious (bacterial, viral like herpes simplex, fungal, or acanthamoeba) or non-infectious (UV exposure, trauma, severe dryness). Contact lens wearers, especially those who sleep in lenses, swim with them, or use non-sterile solutions, are at exceptionally high risk for microbial keratitis. It can be severely painful, cause marked vision changes, intense photophobia, and visible corneal opacities or ulcers. Untreated keratitis can rapidly lead to corneal scarring, thinning, perforation, and blindness, necessitating aggressive, culture-guided antimicrobial therapy and urgent ophthalmologic care.
- Stye (Hordeolum) & Chalazion: A stye is a painful, acute, red lump near the edge of the eyelid caused by an infected eyelash follicle or oil gland, typically Staphylococcus aureus. A chalazion is a non-infectious, chronic, painless granuloma that develops further back on the eyelid from a blocked meibomian gland. While uncomfortable and visually noticeable, styes are usually localized and resolve with consistent warm compresses, gentle massage, and strict lid hygiene. If a lesion persists, enlarges, or obstructs the visual axis, it may require incision and drainage or corticosteroid injection.
When to See a Doctor
While many mild cases of conjunctivitis can be managed safely at home, it's essential to seek professional medical advice to get an accurate diagnosis, rule out sight-threatening mimics, and receive appropriate treatment. Self-diagnosis, while convenient, carries risks of misinterpreting symptoms or inadvertently delaying care for underlying pathology. Contact a doctor, optometrist, or ophthalmologist if you experience:
- Severe, sharp, or throbbing eye pain that isn't relieved by over-the-counter pain relievers or warm compresses.
- Any changes in your vision, such as persistent blurriness, halos around lights, shadowed vision, or double vision that doesn't improve with blinking or cleaning.
- Intense sensitivity to light that forces you to keep your eyes closed even in dimly lit indoor environments.
- A persistent foreign-body sensation or feeling that something is stuck in your eye that doesn't wash out with artificial tears.
- Symptoms that actively worsen or show zero improvement after 2 to 3 days of diligent home care and OTC management.
- A thick, copious, pus-like discharge from the eye that recurs despite completing a full course of prescribed antibiotics.
- Any eye symptoms in a newborn or infant, as this can be a sign of a serious, vision-threatening infection (like gonococcal or chlamydial conjunctivitis acquired during delivery) that requires immediate systemic or intravenous antibiotics.
- You wear contact lenses, have a compromised immune system, recently underwent eye surgery, or have pre-existing eye conditions like glaucoma or diabetic retinopathy.
During your visit, your eye care professional will perform a comprehensive slit-lamp examination to meticulously evaluate the cornea, conjunctiva, eyelids, and anterior chamber. They may apply fluorescein dye to highlight microscopic corneal abrasions, ulcers, or dendritic lesions characteristic of herpes simplex keratitis. In atypical, severe, or non-responsive cases, a conjunctival swab may be collected for bacterial culture and sensitivity testing, viral PCR panels, or cytological analysis to guide targeted, narrow-spectrum therapy. Telehealth consultations can provide valuable initial triage and OTC guidance, but an in-person, magnified evaluation remains the clinical gold standard for definitive diagnosis, particularly when contact lens use, significant pain, or visual changes are involved.
Getting the right diagnosis is the first step toward finding relief, preventing transmission, and ensuring the long-term health of your eyes.
References
- CDC - Conjunctivitis (Pink Eye)
- American Academy of Ophthalmology - What Is Pink Eye?
- NEAII - Allergies or Pink Eye: How to Tell the Difference
- Medical News Today - Pink eye or allergies? Symptoms and how to tell
Frequently Asked Questions
How long does it take for pink eye to clear up on its own?
The duration depends heavily on the underlying etiology and the individual's immune response. Viral conjunctivitis typically peaks around days three to five, remains highly symptomatic for about a week, and resolves completely within one to two weeks as the immune system naturally clears the viral particles. Bacterial conjunctivitis usually shows marked clinical improvement within 24 to 48 hours after initiating prescribed antibiotic drops, with full resolution of redness and discharge occurring in approximately 5 to 7 days. Allergic conjunctivitis, however, lacks a fixed timeline; it will persist or recur indefinitely as long as environmental exposure to the triggering allergen continues, making consistent environmental control and prophylactic medication essential for long-term symptom management.
Can I wear makeup while I have red or irritated eyes?
It is strongly advised to avoid all eye makeup, including mascara, liquid or gel eyeliner, eyeshadow, and cream-based concealers, during any active eye infection or severe allergic flare-up. Makeup products act as reservoirs that can harbor bacteria, trap infectious discharge against the eyelid margin, and introduce additional chemical irritants or preservatives that exacerbate existing inflammation. If you suspect you were using eye cosmetics when your symptoms first began, discard them immediately upon recovery to prevent self-reinfection. Wait at least 24 to 48 hours after all clinical signs have completely resolved and you have finished your treatment course before reintroducing new, unexpired products, and always clean applicators thoroughly before use.
Is it safe to use leftover antibiotic eye drops from a previous prescription?
No, it is never medically safe to self-prescribe, share, or use expired leftover antibiotic eye drops. Different bacterial species and strains require highly specific antibiotics for effective eradication, and using the wrong medication, incorrect concentration, or incomplete course can severely delay recovery, promote the development of multidrug-resistant organisms, and mask underlying serious pathology. Furthermore, once a multi-dose bottle is opened, its sterility is generally compromised after 28 days due to airborne contamination and preservative degradation, significantly increasing the risk of introducing new, opportunistic pathogens to an already compromised ocular surface. Always consult a qualified healthcare provider for a proper clinical evaluation and a fresh, targeted prescription if antibiotic therapy is clinically indicated.
Can chronic stress or severe fatigue trigger allergic conjunctivitis or pink eye?
Stress and fatigue do not directly cause the initial onset of infectious conjunctivitis or create de novo allergic sensitization to external environmental allergens. However, chronic psychological stress, anxiety, and severe sleep deprivation profoundly dysregulate the hypothalamic-pituitary-adrenal (HPA) axis and weaken systemic and localized immune surveillance, making you significantly more susceptible to acquiring viral or bacterial pathogens upon exposure. Additionally, prolonged stress elevates circulating cortisol and pro-inflammatory cytokines, which can exacerbate pre-existing allergy symptoms, destabilize the tear film, worsen ocular surface dryness, and heighten neurogenic inflammation, thereby amplifying the subjective perception of eye discomfort, grittiness, and itching. Prioritizing adequate restorative sleep, hydration, and evidence-based stress management techniques remains a vital, often overlooked component of comprehensive ocular health.
How do I safely clean my eyes if they are heavily crusted shut in the morning?
To safely and hygienically remove infectious discharge or allergen buildup, first wash your hands thoroughly with soap and warm water for at least 20 seconds. Use a clean, soft, lint-free washcloth or sterile gauze pad soaked in comfortably warm water (not hot, to avoid burns or worsening vasodilation). Gently wipe your closed eyelids starting from the inner canthus (near the nose) and sweeping outward toward the temple to avoid dragging potential pathogens or debris across the sensitive corneal surface. Always use a fresh, clean section of the cloth or a completely new wipe for each eye to absolutely prevent cross-contamination. You can also apply a warm, damp compress and hold it gently against the closed eye for 2 to 3 minutes to soften stubborn, hardened crusts before wiping. Never forcefully pry or pull the eyelids open; allow the moisture and gentle heat to gradually dissolve the material so the lids separate naturally without risking microscopic epithelial tearing.
Conclusion
Navigating the clinical differences between pink eye and allergic conjunctivitis is essential for implementing effective treatment, minimizing discomfort, and preventing the widespread transmission of infection. While both conditions share the hallmark presentation of a red, irritated, and often watery eye, distinct diagnostic clues in symptomatology—such as intense histamine-driven itching versus viral gritty discomfort, simultaneous bilateral onset versus initial unilateral presentation, and clear stringy mucus versus thick purulent exudate—provide highly reliable indicators for accurate home triage and clinical identification. Allergic conjunctivitis fundamentally stems from a localized immune hypersensitivity response to environmental triggers and is optimally managed through rigorous allergen avoidance, targeted antihistamines, mast cell stabilizers, and consistent tear film restoration. Infectious conjunctivitis, conversely, results from active viral or bacterial colonization, demanding strict hygiene protocols, supportive symptomatic care, or precise, culture-guided antibiotic therapy to achieve complete resolution and eliminate contagious shedding.
Equally critical is recognizing the clinical warning signs that point toward more severe, sight-threatening ocular pathologies like advanced dry eye syndrome, chronic blepharitis, anterior uveitis, or microbial keratitis. The presence of severe localized pain, objective vision changes, profound photophobia, corneal clouding, or a complete lack of clinical improvement after several days of appropriate conservative care necessitates immediate, in-person evaluation by a licensed eye care professional. By deeply understanding the underlying immunological and microbiological mechanisms, employing evidence-based at-home relief strategies, maintaining strict ocular hygiene, and knowing precisely when to escalate care to a specialist, you can effectively protect your visual acuity, minimize systemic disruption, and actively prevent the unnecessary community transmission of contagious pathogens. Prioritizing proactive environmental control, staying meticulously informed about your personal allergy triggers, and consistently consulting an eye care professional when clinical boundaries are crossed remain the undisputed cornerstones of lifelong ocular health and visual preservation.

About the author
Aisha Khan, MD, is a board-certified pediatrician with a focus on adolescent medicine and developmental disorders. She runs a private practice in Austin, Texas, and is a vocal advocate for child mental health services.