Loose Molar in Adults: Causes, Symptoms, and How to Save Your Tooth

Key points
- Bone Loss (Osteoporosis): This condition weakens bones throughout the body, including the jawbone, making teeth more susceptible to loosening. Systemic bone mineral density directly correlates with alveolar bone health. Furthermore, medications used to treat osteoporosis, such as bisphosphonates or denosumab, carry a risk of medication-related osteonecrosis of the jaw (MRONJ), which can manifest as tooth mobility, exposed bone, and delayed healing following dental procedures.
- Hormonal Changes: Fluctuations in hormones, particularly during pregnancy, can temporarily affect the ligaments and bones supporting the teeth, causing them to feel loose. Elevated progesterone levels increase vascular permeability and alter the subgingival microbiome, leading to "pregnancy gingivitis." During menopause, declining estrogen levels can accelerate osteoclastic activity in the jawbone and cause mucosal thinning, further compromising periodontal stability.
- Ill-fitting Dental Appliances: Poorly fitted braces or dentures can exert improper pressure on teeth, leading to mobility. Orthodontic movement intentionally creates temporary mobility by remodeling bone, but uncontrolled or poorly planned forces can cause irreversible root resorption and periodontal breakdown.
- Medication Side Effects: Some people taking GLP-1 drugs like Ozempic have reported dental side effects, dubbed "Ozempic teeth," which can include dry mouth and other issues that may contribute to tooth decay and looseness, as reported by Healthline. Xerostomia (dry mouth) reduces the protective, buffering, and antimicrobial properties of saliva, creating a highly cariogenic and periodontally hostile environment. Other medications, such as calcium channel blockers, anticonvulsants, and immunosuppressants, can induce gingival hyperplasia, creating pseudopockets that trap bacteria and accelerate bone loss.
- Cysts or Tumors: In rare cases, a growth in the jawbone can displace a tooth or destroy the bone around it. The New York Post notes that a persistent loose tooth can be a lesser-known sign of oral cancer. Squamous cell carcinomas, ameloblastomas, and odontogenic keratocysts can present with unexplained tooth mobility, unexplained bleeding, or persistent ulcerations. Any unexplained loosening that does not correlate with trauma or classic periodontitis warrants thorough imaging and possibly a biopsy.
- Nutritional Deficiencies: Severe deficiencies in vitamin C (scurvy), vitamin D, or calcium can impair collagen synthesis and bone mineralization. Vitamin C is essential for healthy periodontal ligament formation, while vitamin D regulates calcium homeostasis and modulates the immune response in gingival tissues.
Feeling that unnerving wiggle in a back tooth can be alarming. While a loose tooth is a rite of passage for a child, a loose molar in an adult is a clear warning sign from your body that something is wrong. It is not something that will fix itself and requires immediate attention from a dental professional. Understanding the underlying biology is crucial: your teeth are not simply embedded in your jawbone like nails in wood. Instead, each permanent tooth is suspended in its bony socket by the periodontal ligament (PDL), a highly vascularized network of collagen fibers that acts as both a shock absorber and a proprioceptive sensor. When these fibers are compromised or the surrounding alveolar bone resorbs, mobility occurs.
Understanding the root cause is the first step toward saving your tooth and protecting your overall health. This comprehensive guide synthesizes expert advice, current clinical data, and periodontal research to explain why your molar might be loose, what you should do right now, and what treatments can restore your smile and function.
Why Your Adult Molar is Loose: Uncovering the Common Causes
A permanent molar is anchored securely in your jawbone by a network of ligaments and tissue. When it becomes loose, it means this support system has been compromised. The vast majority of cases can be traced back to a few key culprits, each with distinct pathophysiological mechanisms and clinical presentations.
Periodontal (Gum) Disease: The Primary Culprit
According to the Cleveland Clinic, the most common cause of loose adult teeth is periodontal disease. This is a serious gum infection that damages the soft tissue and, without treatment, can destroy the bone that supports your teeth. Periodontitis is fundamentally a dysbiotic microbial condition, where the normal balance of oral bacteria shifts toward pathogenic species like Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola. These anaerobic bacteria trigger a chronic inflammatory immune response. Over time, the body's own immune cells release matrix metalloproteinases and inflammatory cytokines (such as IL-1β, TNF-α, and prostaglandins) that inadvertently break down collagen and resorb bone in an attempt to control the infection.
It progresses in stages:
- Plaque Buildup: Bacteria-filled plaque hardens into tartar (calculus), which acts as a physical irritant and a porous reservoir for bacterial colonization that cannot be removed by brushing alone.
- Gingivitis: Gums become inflamed, red, and may bleed easily. At this stage, the disease is confined to the gingival tissues, and no irreversible bone loss has occurred. With professional intervention and improved home care, it is completely reversible.
- Periodontitis: The gums pull away from the tooth, forming infected pockets. As the infection spreads below the gum line, it attacks the bone, causing irreversible bone loss and loosening the tooth. Chronic periodontitis can remain asymptomatic for years until significant structural damage has occurred, making regular periodontal charting essential.
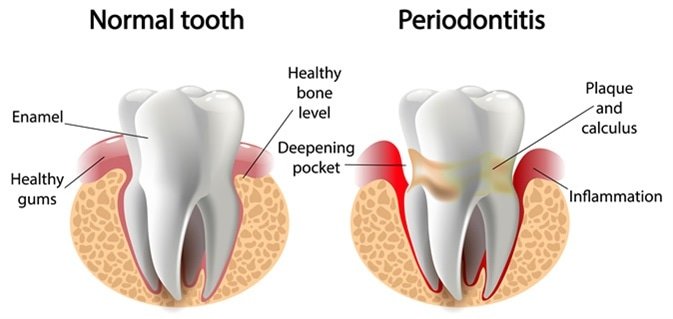 Image Source: Lotus Dental and Aesthetics Clinic
Image Source: Lotus Dental and Aesthetics Clinic
Physical Trauma or Injury
A direct blow to the face from an accident, a fall, or a sports injury can stretch or damage the periodontal ligaments that hold your tooth in place, causing it to become loose instantly. Clinically, this is categorized under dental luxation injuries. Depending on the force vector and magnitude, trauma can cause subluxation (increased mobility without displacement), extrusion (partial displacement out of the socket), intrusion (displacement into the alveolar bone), or even alveolar bone fractures that take the tooth with them.
Beyond acute injuries, chronic microtrauma from habitual behaviors like chewing ice, biting fingernails, or using teeth as tools can gradually fatigue the periodontal fibers. In dentistry, this is referred to as primary occlusal trauma, where excessive biting forces overwhelm a tooth that otherwise has normal periodontal support. The body responds to this mechanical overload with a widened periodontal ligament space on radiographs, increased tooth mobility, and sometimes tooth wear or enamel craze lines.
Teeth Grinding and Clenching (Bruxism)
Many people grind their teeth, often unconsciously during sleep. This constant, excessive force can gradually weaken the periodontal ligaments and supporting bone over time, leading to tooth mobility. Sleep bruxism is increasingly recognized by sleep medicine specialists as a sleep-related movement disorder, often linked to micro-arousals, sympathetic nervous system hyperactivity, and sometimes associated with obstructive sleep apnea.
When bruxism forces exceed the physiological tolerance of the periodontium, it creates secondary occlusal trauma. In this scenario, normal chewing forces or mild grinding become destructive because the underlying support (bone and ligament) is already compromised by periodontitis. This combination creates a vicious cycle: inflammation weakens the support, bruxism applies destructive force, and the mobility increases further. Additionally, chronic clenching can lead to masseter muscle hypertrophy, temporomandibular joint (TMJ) dysfunction, tension headaches, and cracked tooth syndrome, all of which complicate the clinical picture.
Other Contributing Factors
While less common, other conditions can lead to a loose molar:
- Bone Loss (Osteoporosis): This condition weakens bones throughout the body, including the jawbone, making teeth more susceptible to loosening. Systemic bone mineral density directly correlates with alveolar bone health. Furthermore, medications used to treat osteoporosis, such as bisphosphonates or denosumab, carry a risk of medication-related osteonecrosis of the jaw (MRONJ), which can manifest as tooth mobility, exposed bone, and delayed healing following dental procedures.
- Hormonal Changes: Fluctuations in hormones, particularly during pregnancy, can temporarily affect the ligaments and bones supporting the teeth, causing them to feel loose. Elevated progesterone levels increase vascular permeability and alter the subgingival microbiome, leading to "pregnancy gingivitis." During menopause, declining estrogen levels can accelerate osteoclastic activity in the jawbone and cause mucosal thinning, further compromising periodontal stability.
- Ill-fitting Dental Appliances: Poorly fitted braces or dentures can exert improper pressure on teeth, leading to mobility. Orthodontic movement intentionally creates temporary mobility by remodeling bone, but uncontrolled or poorly planned forces can cause irreversible root resorption and periodontal breakdown.
- Medication Side Effects: Some people taking GLP-1 drugs like Ozempic have reported dental side effects, dubbed "Ozempic teeth," which can include dry mouth and other issues that may contribute to tooth decay and looseness, as reported by Healthline. Xerostomia (dry mouth) reduces the protective, buffering, and antimicrobial properties of saliva, creating a highly cariogenic and periodontally hostile environment. Other medications, such as calcium channel blockers, anticonvulsants, and immunosuppressants, can induce gingival hyperplasia, creating pseudopockets that trap bacteria and accelerate bone loss.
- Cysts or Tumors: In rare cases, a growth in the jawbone can displace a tooth or destroy the bone around it. The New York Post notes that a persistent loose tooth can be a lesser-known sign of oral cancer. Squamous cell carcinomas, ameloblastomas, and odontogenic keratocysts can present with unexplained tooth mobility, unexplained bleeding, or persistent ulcerations. Any unexplained loosening that does not correlate with trauma or classic periodontitis warrants thorough imaging and possibly a biopsy.
- Nutritional Deficiencies: Severe deficiencies in vitamin C (scurvy), vitamin D, or calcium can impair collagen synthesis and bone mineralization. Vitamin C is essential for healthy periodontal ligament formation, while vitamin D regulates calcium homeostasis and modulates the immune response in gingival tissues.
Recognizing the Warning Signs: Symptoms of a Loose Molar
The wiggling sensation is the most obvious sign, but it's rarely the only one. Be aware of these accompanying symptoms, which can help your dentist diagnose the cause:
- Pain, soreness, or tenderness, especially when chewing
- Red, swollen, or bleeding gums
- Gum recession, which makes teeth appear longer
- Pus or signs of infection around the tooth and gums (periodontal abscess)
- Persistent bad breath or a foul taste in your mouth
- A noticeable change in how your teeth fit together when you bite (occlusal shift)
Beyond these patient-noticed symptoms, dental professionals utilize specific diagnostic criteria to assess mobility and disease severity. The Miller Classification is the standard for grading tooth mobility: Class I indicates slight horizontal movement (less than 1 mm), Class II denotes greater horizontal movement (1-2 mm) but no vertical depressibility, and Class III signifies severe horizontal movement exceeding 2 mm combined with vertical depressibility in the socket. Additionally, clinicians use a periodontal probe to measure pocket depths. Healthy sulci measure 1-3 mm. Pockets measuring 4-5 mm indicate early bone loss, while depths of 6 mm or greater suggest advanced periodontitis with significant attachment loss. Furcation involvement, where bone loss has extended between the roots of a multi-rooted molar, is graded from I (early probe penetration) to IV (complete through-and-through passage), and is a critical prognostic indicator for molar salvageability.
Radiographic evaluation, including periapical X-rays and cone-beam computed tomography (CBCT), reveals the true extent of alveolar bone destruction, furcation defects, root fractures, and the relationship of the tooth to vital anatomical structures like the inferior alveolar nerve or maxillary sinus. These diagnostic tools, combined with clinical mobility assessment and occlusal analysis, create a comprehensive picture necessary for accurate treatment planning.
What to Do Immediately for a Loose Molar (And What NOT to Do)
A loose adult molar is a dental emergency. The sooner you act, the better your chances of saving the tooth. Delaying care often transforms a salvageable Class I or II mobility case into a Class III extraction scenario. In acute situations, particularly following trauma or sudden severe pain with swelling, the inflammatory cascade is actively damaging tissues. Early intervention halts this progression and stabilizes the periodontal environment.
First-Aid Steps Before Your Dental Appointment
- Call Your Dentist Immediately: Schedule an emergency appointment. Time is critical. If you experience facial swelling that affects your breathing, swallowing, or vision, seek emergency medical care or go to an urgent care facility immediately, as these are signs of a spreading odontogenic infection that can become life-threatening.
- Avoid Wiggling It: Do not touch, push, or wiggle the tooth with your tongue or fingers. This can further damage the weakened ligaments. Constant mechanical manipulation disrupts the natural healing response, re-tears newly forming collagen fibers, and increases the risk of introducing secondary bacterial contamination.
- Switch to a Soft-Food Diet: Avoid chewing on the affected side of your mouth. Stick to soft foods like yogurt, soup, and smoothies to minimize pressure. Avoid sticky, chewy, or extremely hot/cold foods that could aggravate inflamed nerves or dislodge temporary clotting. Nutritional intake should remain high in protein, vitamins C and D, and calcium to support tissue repair.
- Keep the Area Clean: Gently rinse your mouth with a warm salt-water solution (1/2 teaspoon of salt in a glass of warm water) two to three times a day. This helps reduce bacteria and soothe inflammation without being abrasive. Avoid aggressive mouthwashes containing high concentrations of alcohol, as they can desiccate oral tissues. If prescribed by a dentist, a 0.12% chlorhexidine gluconate rinse can provide powerful antimicrobial action but should only be used for short-term therapeutic periods (typically 1-2 weeks) to prevent tooth staining and altered taste sensation.
Additional supportive measures include applying a cold compress externally to the cheek for 15-minute intervals if trauma or acute inflammation is present, and elevating your head while sleeping to reduce localized blood flow and throbbing pain. Over-the-counter analgesics like ibuprofen or naproxen can help manage discomfort and reduce prostaglandin-mediated inflammation, provided they are not contraindicated for your specific health profile.
Critical Mistake to Avoid: Do Not Pull Your Own Tooth
While it might be tempting to resolve the issue yourself, you should never attempt to pull a loose adult tooth. As Colgate explains, unlike baby teeth, permanent teeth are not designed to fall out. Pulling it yourself can lead to excruciating pain, uncontrolled bleeding, severe damage to the surrounding gum and bone, and a high risk of infection.
Root anatomy is highly complex; permanent molars typically possess two, three, or even four divergent roots with curved or hooked shapes. Attempting extraction without proper surgical technique, radiographic visualization, and appropriate instrumentation frequently results in root fracture, leaving fragments embedded in the jawbone that require complex surgical retrieval. Furthermore, unsanitary extraction attempts can drive oral flora deep into the periapical bone and facial spaces, precipitating a severe cellulitis or abscess. Even if the tooth is severely compromised, a controlled professional extraction allows for proper socket debridement, bone grafting if necessary, and immediate planning for tooth replacement.
Can a Loose Molar Be Saved? Understanding the Salvageability Spectrum
Whether a loose molar can be saved depends entirely on the underlying cause and the extent of the damage. A dentist will assess its mobility, which is often graded in stages. Prognosis determination is a multi-factorial calculation that considers patient compliance, systemic health, anatomical crown-to-root ratio, periodontal attachment levels, occlusal forces, and the strategic value of the tooth in your dental arch.
The Stages of Tooth Mobility
- Initial Mobility: The tooth has very slight, subtle movement. At this stage, if the cause is treated promptly (e.g., a deep cleaning for early gum disease, or a simple occlusal adjustment for bruxism), the prognosis for saving the tooth is excellent. The periodontal ligament retains remarkable regenerative capacity when the inflammatory or traumatic insult is removed.
- Moderate Mobility: The tooth's movement is more noticeable. This indicates more significant damage to the supporting structures, and intervention is urgently needed. Treatment becomes more complex, often requiring combined approaches such as periodontal therapy, splinting, and occlusal rehabilitation. Success depends heavily on patient adherence to meticulous oral hygiene and maintenance schedules.
- Advanced Mobility: The tooth moves visibly and may be unstable even when speaking. This signifies extensive bone loss or damage, and the tooth is at high risk of being lost. While advanced mobility does not automatically mandate extraction, it signals a hopeless or questionable prognosis unless aggressive regenerative procedures or strategic splinting are viable. At this stage, the tooth may also become a bacterial reservoir that jeopardizes adjacent teeth and overall oral health.
When a Molar is Likely Unsalvageable
A dentist will likely recommend extraction if they find:
- Extensive Bone Loss: Too much of the supporting jawbone has been destroyed by advanced periodontitis. When bone loss reaches the apical third of the root, or when horizontal bone loss exceeds 50-60% of the root length, the tooth often lacks adequate leverage to withstand masticatory forces.
- Severe Tooth Fracture: The tooth has a vertical root fracture, where the crack runs from the crown down through the root. VRFs are notoriously difficult to diagnose early but are almost universally fatal to the tooth because they create an inseparable pathway for bacteria to invade the periodontium, leading to isolated deep probing defects and rapid localized bone destruction.
- Advanced, Untreatable Infection: The infection has caused too much damage to the tooth and surrounding bone, resulting in a non-restorable crown or a periapical lesion that does not resolve with endodontic therapy. Non-vital teeth with persistent fistulas, severe external root resorption, or extensive caries that undermines the structural integrity beyond the gumline typically require extraction to prevent systemic spread of infection.
Professional Treatments to Save Your Molar
Your dentist's treatment plan will be tailored to address the specific cause of the looseness. Modern periodontics and restorative dentistry utilize a combination of non-invasive, minimally invasive, and surgical modalities to stabilize teeth and regenerate lost tissue whenever possible.
Treating Gum Disease
- Scaling and Root Planing: This non-surgical deep cleaning is the first line of defense. It removes plaque and tartar from below the gumline and smooths the tooth roots to help the gums reattach. Performed under local anesthesia, SRP debrides the root surface of bacterial endotoxins and calculus, creating a biocompatible surface for periodontal attachment. Follow-up evaluations at 4-6 weeks post-treatment assess pocket depth reduction and tissue healing. Adjunctive therapies may include localized antibiotic delivery (e.g., doxycycline microspheres or minocycline gels) directly into residual pockets.
- Surgery: For advanced cases, surgical options like flap surgery (to clean roots directly and reduce pocket depths), bone and gum grafts (to regenerate lost tissue), or guided tissue regeneration (GTR) may be necessary, according to Medical News Today. Bone grafting utilizes autografts (patient's own bone), allografts (human donor bone), xenografts (bovine-derived), or synthetic bioactive materials to scaffold new bone growth. GTR employs biocompatible barrier membranes to prevent fast-growing epithelial cells from migrating into the wound site, allowing slower-growing bone and ligament cells to repopulate the defect.
 Image Source: Dear Doctor
Image Source: Dear Doctor
Stabilizing the Tooth
- Dental Splinting: The loose molar can be temporarily or permanently bonded to adjacent, stable teeth with a composite resin and fiber-reinforced splint or a bonded wire. This distributes occlusal forces across multiple teeth, holds the mobile tooth in a functional position, and allows the periodontal ligament to heal without the stress of independent movement. Extracoronal splints are highly effective but require meticulous oral hygiene to prevent plaque accumulation at the splint margins. In some cases, intracoronal splints (using precision attachments within crowns) offer improved aesthetics and cleansability.
- Occlusal Adjustment: If secondary occlusal trauma is contributing to mobility, a clinician may perform selective grinding to eliminate premature contacts and distribute chewing forces evenly. This is always conservative and reversible, focusing on functional pathways rather than arbitrary tooth reduction.
Addressing Bruxism
- Night Guards: A custom-fitted hard acrylic occlusal guard worn during sleep protects teeth from the immense pressure of grinding. Unlike over-the-counter boil-and-bite guards, custom appliances are precisely fabricated on models to ensure even force distribution, prevent super-eruption of unopposed teeth, and reduce masseter muscle hyperactivity.
- Behavioral and Pharmacological Interventions: For severe awake bruxism, cognitive behavioral therapy, biofeedback, and stress management techniques are highly effective. In refractory cases involving muscle hypertrophy and joint pain, targeted botulinum toxin (Botox) injections into the masseter and temporalis muscles can significantly reduce clenching force and provide symptomatic relief, though this is typically considered an adjunct rather than a first-line treatment.
If the Tooth Cannot Be Saved: Extraction and Replacement
If the molar is deemed unsalvageable, your dentist will recommend extraction followed by a replacement option to prevent bone loss and shifting of other teeth. The human body naturally resorbs alveolar bone once a tooth root is removed, at a rate of approximately 0.5-1 mm per year in the first few years. Timely replacement is critical to maintaining facial structure and arch integrity.
These include:
- Dental Implants: A titanium or zirconia post that acts as an artificial root, providing a strong, permanent foundation for a crown. Implants offer the highest success rates, prevent bone resorption through functional loading, and do not require altering adjacent teeth. Success depends on adequate bone volume and density, good systemic health, and controlled periodontal status prior to placement.
- Dental Bridges: A prosthetic tooth anchored by crowns placed on the adjacent teeth. Traditional bridges are a reliable, faster alternative to implants but require reduction of healthy abutment teeth. Maryland (resin-bonded) bridges offer a more conservative approach for specific clinical scenarios, particularly when adjacent teeth are unrestored.
- Partial Dentures: A removable appliance with acrylic or metal frameworks that fills the gap. Modern removable partial dentures with precision attachments or flexible nylon frameworks offer improved comfort and aesthetics. While less stable and functional than fixed options, they remain a viable, cost-effective solution for patients with multiple missing teeth or contraindications for surgery.
The Broader Picture: How a Loose Molar Connects to Your Overall Health
A loose molar is more than a dental issue; it's a window into your systemic health. The chronic inflammation from periodontal disease—the number one cause of loose teeth—is linked to a host of serious health conditions through shared inflammatory pathways and bacteremic episodes.
The bacteria and inflammation from your gums can enter your bloodstream and contribute to:
- Cardiovascular Disease: Increased risk of heart attack and stroke. Oral pathogens like P. gingivalis have been isolated within atherosclerotic plaques. Chronic systemic inflammation elevates C-reactive protein (CRP), fibrinogen, and homocysteine levels, promoting endothelial dysfunction, platelet aggregation, and arterial plaque formation.
- Diabetes: Gum disease can make it harder to control blood sugar levels, creating a well-documented bidirectional relationship. Hyperglycemia impairs neutrophil function and collagen synthesis, worsening periodontal destruction. Conversely, severe periodontitis increases systemic insulin resistance. Successful periodontal therapy has been shown to modestly improve glycemic control (HbA1c reduction of 0.3-0.6%).
- Respiratory Infections: Bacteria can be inhaled into the lungs, causing pneumonia, particularly in hospitalized, elderly, or immunocompromised individuals. Aspiration of periodontal pathogens is a recognized risk factor for community-acquired and ventilator-associated pneumonia.
- Cognitive Decline: Emerging research links poor oral health to an increased risk of conditions like Alzheimer's. Chronic periodontal pathogens and their neuroinflammatory mediators (such as lipopolysaccharides and amyloid-beta cross-reactive antibodies) may breach the blood-brain barrier or stimulate microglial activation, contributing to neurodegeneration.
- Cancer: Studies have shown a correlation between tooth loss from gum disease and an increased risk of certain cancers, including esophageal, gastric, pancreatic, and lung cancer. Proposed mechanisms involve nitrosamine formation from nitrate-reducing oral bacteria, chronic immune dysregulation, and direct bacterial oncogenic properties.
- Adverse Pregnancy Outcomes: Periodontitis is associated with an increased risk of preeclampsia, low birth weight, and preterm delivery. Inflammatory mediators (prostaglandins and cytokines) can trigger premature uterine contractions and placental dysfunction.
Taking care of a loose tooth is not just about saving your smile—it's about protecting your long-term health. Managing periodontal disease effectively requires a multidisciplinary approach, integrating dental care with primary medicine, particularly for patients managing diabetes, cardiovascular conditions, autoimmune disorders, or preparing for pregnancy.
Frequently Asked Questions
Can a slightly loose tooth tighten up on its own without dental treatment?
A tooth with very minor, transient mobility caused by temporary trauma or acute localized inflammation may stabilize if the irritant is removed and the area is kept meticulously clean. However, this is the exception rather than the rule. Once periodontal bone loss has occurred, it does not regenerate spontaneously. The periodontal ligament requires a biologically clean and stable environment to reorganize and heal. Without professional debridement to remove subgingival calculus and biofilm, the inflammatory cascade continues, and mobility will progressively worsen. Any adult tooth exhibiting noticeable mobility beyond a day or two requires a clinical and radiographic evaluation to determine the underlying cause and appropriate intervention.
How long does it take for a splinted or treated loose molar to feel fully stable again?
Healing timelines depend heavily on the treatment modality and initial severity. Following scaling and root planing, initial tissue healing and reduced inflammation occur within 2-4 weeks. However, true periodontal attachment and bone remodeling take 3-6 months to mature. If a dental splint is placed, patients often experience immediate functional improvement, but the splint typically remains in place for 4-8 weeks to allow the periodontal ligament fibers to reorganize under controlled stress. For teeth affected by occlusal trauma or bruxism, symptom resolution may be noticed within days of wearing a properly adjusted night guard, but long-term stabilization requires ongoing compliance and occlusal management. Regular re-evaluations at 1, 3, and 6 months post-treatment are standard to monitor attachment gains and adjust the therapeutic plan accordingly.
Is dental implant placement painful, and what is the typical recovery process?
Modern dental implant placement is performed under local anesthesia, and often with supplemental sedation for anxious patients or complex cases. The procedure itself is not painful; post-operative discomfort is typically mild to moderate and well-managed with over-the-counter analgesics or prescribed medications for a few days. Swelling and bruising peak at 48-72 hours and gradually subside. The osseointegration phase, where the bone biologically fuses to the titanium or zirconia implant, takes 3-6 months. During this period, patients wear a temporary prosthetic and must adhere to a soft-food diet while avoiding excessive pressure on the surgical site. Strict oral hygiene, chlorhexidine rinses (if prescribed), and attending all follow-up appointments are crucial for preventing peri-implantitis and ensuring long-term success. Most patients report that the discomfort of healing is significantly less than enduring chronic dental infections or struggling with ill-fitting dentures.
Can hormonal changes during pregnancy cause permanent tooth looseness?
Pregnancy-induced hormonal fluctuations, particularly elevated estrogen and progesterone, significantly increase gingival vascularity and alter the subgingival microbiome, leading to pregnancy gingivitis or, in severe cases, pregnancy epulis (pyogenic granuloma). These conditions can cause temporary tooth mobility due to severe gum inflammation, edema, and transient ligamentous laxity. In the vast majority of cases, this mobility resolves naturally postpartum once hormone levels stabilize and dedicated periodontal care is implemented. However, pregnancy does not protect against periodontal destruction. If pre-existing plaque and calculus are present, pregnancy can accelerate underlying periodontitis. Therefore, maintaining rigorous oral hygiene, continuing with professional cleanings during pregnancy (which are safe in all trimesters, ideally in the second), and monitoring mobility closely are essential to prevent temporary physiological changes from becoming permanent pathological bone loss.
What steps can I take to prevent my other teeth from becoming loose in the future?
Preventing further tooth mobility requires a comprehensive, lifelong commitment to periodontal maintenance. First, adhere to a meticulous daily oral hygiene routine: brush twice daily with a soft-bristled or electric toothbrush using the modified Bass technique, clean interdentally daily with floss or interdental brushes, and consider using an ADA-approved antimicrobial toothpaste if prone to inflammation. Second, attend professional dental cleanings and periodontal maintenance appointments every 3-4 months (or as recommended by your provider) rather than annually, as biofilm reforms and hardens into calculus within weeks. Third, address modifiable risk factors: quit smoking or vaping, as tobacco use severely compromises gingival blood flow and immune response; manage systemic conditions like diabetes through tight glycemic control; and wear a professionally fabricated night guard if you grind your teeth. Finally, maintain a nutrient-dense diet rich in antioxidants, vitamin C, vitamin D, and calcium, and stay hydrated to promote optimal salivary function. Early detection through regular exams is your strongest defense against progressive periodontal breakdown.
Conclusion
Discovering that your adult molar has become loose is undoubtedly distressing, but it is a highly treatable condition when addressed promptly and appropriately. A loose permanent tooth is never a normal occurrence; it is a critical clinical sign indicating that the foundational support system of your tooth—the periodontal ligament and alveolar bone—has been compromised by infection, trauma, biomechanical stress, or systemic factors. Ignoring the symptom or attempting home remedies can rapidly accelerate bone loss, turning a salvageable tooth into a dental extraction and potentially jeopardizing your overall systemic health.
Modern dentistry offers a robust arsenal of diagnostic tools and therapeutic interventions, from minimally invasive deep cleanings and custom occlusal guards to advanced periodontal surgery and strategic tooth splinting. When a tooth cannot be saved, predictable and highly functional replacement options like dental implants, bridges, and modern partial dentures ensure that you never have to live with compromised chewing function or an incomplete smile.
The key takeaway is clear: time is your most valuable asset in managing a loose molar. Seek professional evaluation at the first sign of abnormal mobility, adhere strictly to prescribed treatment protocols, and commit to lifelong periodontal maintenance. By doing so, you not only preserve your natural teeth for as long as biologically possible, but you also actively protect your heart, your metabolic health, and your long-term well-being. Schedule that dental appointment today, take control of your oral health, and step confidently toward a stable, functional, and pain-free smile.
References
- Cleveland Clinic. (2024). Loose Tooth: Causes & What To Do. https://my.clevelandclinic.org/health/diseases/loose-tooth
- Medical News Today. (2018). Loose tooth: Treatments, causes, and prevention. https://www.medicalnewstoday.com/articles/322028
- Colgate. Pulling A Tooth At Home: When It's OK And When It's Not. https://www.colgate.com/en-us/oral-health/tooth-removal/pulling-a-tooth-at-home-when-its-ok-and-when-its-not
- Healthline. (2025). ‘Ozempic Teeth’: GLP-1 Drugs May Cause Tooth Decay, Experts Say. https://www.healthline.com/health-news/ozempic-teeth-may-impact-dental-health
- New York Post. (2025). A loose tooth can be sign of mouth cancer — 4 others revealed. https://nypost.com/2025/02/12/health/a-loose-tooth-can-be-sign-of-mouth-cancer-4-others-revealed/

About the author
Benjamin Carter, MD, is a board-certified otolaryngologist specializing in head and neck surgery, with an expertise in treating throat cancer. He is an associate professor and the residency program director at a medical school in North Carolina.