Broken Cuboid Bone: Complete Guide to Symptoms, Treatment, and Recovery

Experiencing sudden, sharp pain along the outer side of your foot after a misstep, fall, or intense workout can be both alarming and debilitating. When the lateral midfoot collapses under unexpected force, the cuboid bone often bears the brunt of the trauma. A broken cuboid bone is a complex midfoot injury that disrupts your biomechanical alignment, compromises your ability to bear weight, and requires precise clinical management to restore function. Unlike simple toe or ankle injuries, fractures in this region involve intricate ligamentous attachments and articular surfaces that directly influence your gait, stability, and long-term mobility. Understanding the anatomy, recognizing the early warning signs, and following evidence-based treatment protocols are essential steps toward a full recovery. This comprehensive guide provides actionable insights, clinically verified rehabilitation strategies, and preventive measures to help you navigate your healing journey safely and effectively. Whether you are an athlete recovering from a sports collision or an individual managing a workplace slip-and-fall, knowing what to expect and how to optimize your recovery timeline can make a significant difference in your outcome.
Understanding the Cuboid Bone and Its Role in Foot Biomechanics
Anatomy and Function of the Midfoot Lateral Column
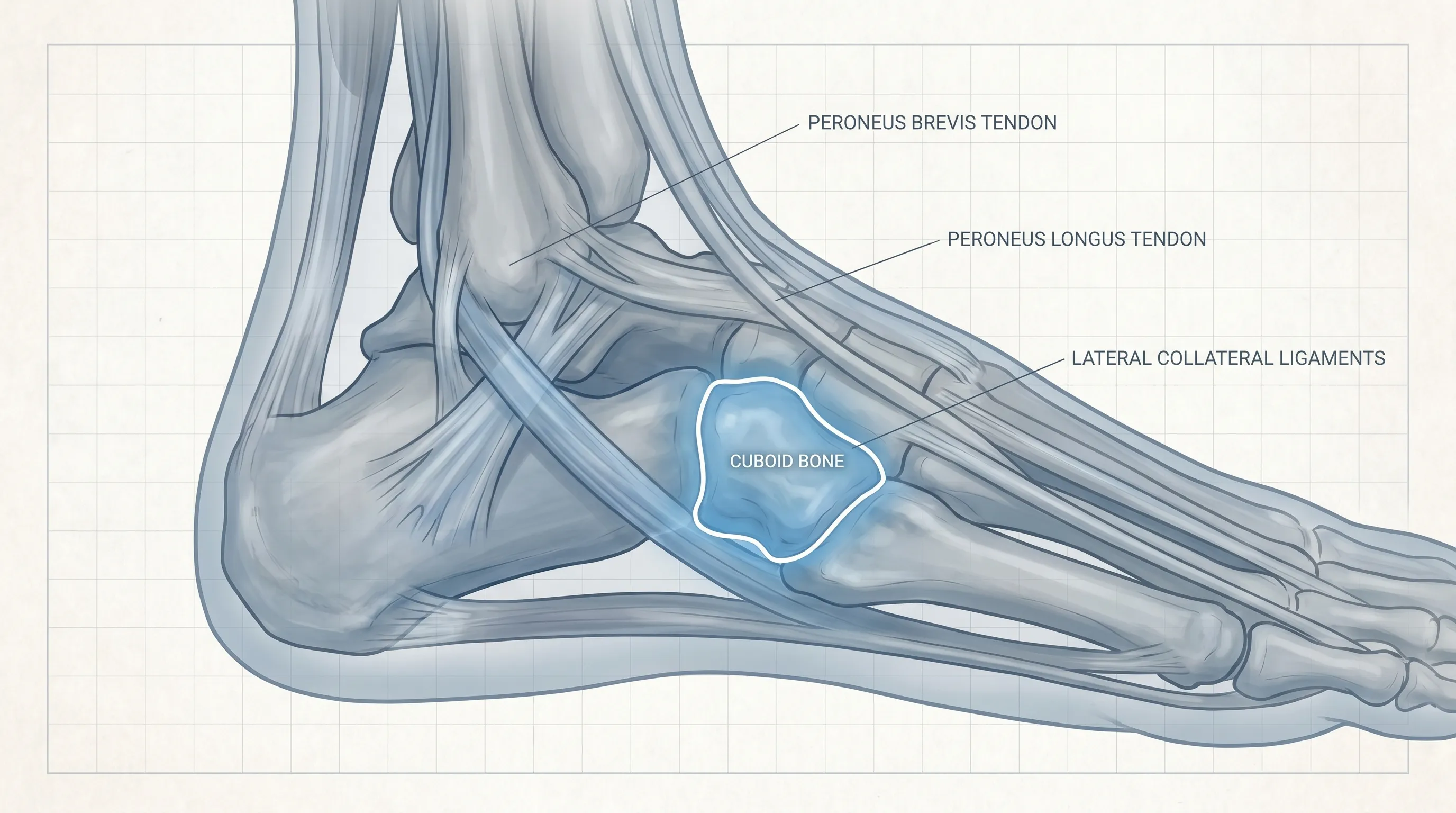
The human foot contains 26 bones, and the cuboid bone serves as a critical keystone within the lateral column of the midfoot. Positioned anterior to the calcaneus (heel bone) and articulating medially with the third and fourth cuneiforms, this cube-shaped bone plays a fundamental role in force distribution during locomotion. When you take a step, the cuboid helps transfer kinetic energy from the heel to the forefoot, acting as a rigid lever during the push-off phase of your gait cycle. It also stabilizes the lateral longitudinal arch and works in concert with the peroneal tendons that glide beneath it. Because it is tightly bound by strong plantar and dorsal ligaments, including the long plantar ligament and the calcaneocuboid joint capsule, the bone normally resists excessive motion. However, when subjected to abnormal torque or direct compression, these stabilizing structures can fail, resulting in a broken cuboid bone that disrupts the entire midfoot architecture. Clinical studies published by the American Academy of Orthopaedic Surgeons emphasize that even minor misalignments in this region can lead to chronic midfoot pain, altered gait patterns, and accelerated joint degeneration if not properly addressed. Maintaining structural integrity through proper alignment and protected rehabilitation remains the cornerstone of successful recovery.
Why the Lateral Column is Prone to Injury
The lateral aspect of the foot absorbs a disproportionate amount of shear and compressive forces during dynamic movement, especially on uneven surfaces or during rapid directional changes. Unlike the medial column, which is reinforced by thicker bone density and a more rigid arch structure, the lateral column prioritizes flexibility and shock absorption. This anatomical trade-off makes the cuboid bone highly vulnerable to both acute trauma and cumulative microtrauma. Athletes participating in sports such as basketball, soccer, dance, and trail running frequently experience high-impact lateral loading that can compromise the bone's structural threshold. Additionally, individuals with underlying biomechanical variations, such as pes cavus (high arches) or hindfoot varus, naturally concentrate more weight along the outer edge of the foot, increasing susceptibility to injury. Recognizing these biomechanical risk factors allows patients and clinicians to implement targeted interventions early. Practical Tip: If you regularly participate in high-impact sports or work on uneven terrain, incorporating lateral foot stabilization exercises and wearing shoes with reinforced midsoles can significantly reduce stress on the cuboid region and prevent a broken cuboid bone from occurring.
Common Causes and Mechanisms of Injury
Direct Trauma and High-Impact Events
Direct compression is the most straightforward mechanism for fracturing the cuboid. When a heavy object falls onto the lateral foot or when the outer foot strikes a rigid surface during a motor vehicle collision, the bone experiences sudden, concentrated force that exceeds its tensile strength. These high-energy injuries often result in comminuted fractures, where the bone shatters into multiple fragments, and frequently involve soft tissue damage, including bruising, tendon lacerations, or ligament avulsions. Emergency protocols prioritize rapid immobilization, vascular assessment, and advanced imaging to evaluate fragment displacement. In cases where the skin integrity is compromised, surgical debridement and stabilization become urgent priorities to prevent infection and non-union. Action Step: Immediately after a direct impact injury, avoid attempting to "walk it off." Apply controlled cryotherapy for 15 to 20 minutes, elevate the limb above heart level, and seek urgent orthopedic evaluation to prevent secondary complications.
Indirect Forces and Overuse Stress Fractures
Not all injuries stem from sudden trauma. A significant portion of cuboid fractures occur through indirect mechanisms, particularly rotational forces and repetitive microtrauma. When the foot is planted firmly and the body twists violently, torsional stress travels through the midfoot, compressing the cuboid between the calcaneus and the metatarsal bases. This mechanism is commonly observed in pivoting sports, dance routines, and occupational settings requiring frequent direction changes. Additionally, stress fractures develop gradually when repetitive loading outpaces the bone's remodeling capacity. Military personnel, long-distance runners, and individuals who rapidly increase their training volume are at elevated risk. Stress-related injuries often present with insidious, progressive discomfort that worsens with activity and eases with rest. According to research from the National Center for Biotechnology Information, early intervention during the stress reaction phase can prevent progression to a complete broken cuboid bone. Practical Advice: Monitor training logs closely and adhere to the 10 percent rule when increasing mileage or intensity. If lateral foot pain persists beyond three days, reduce impact activities and consult a sports medicine specialist.
Occupational and Lifestyle Risk Factors
Beyond athletic pursuits, everyday lifestyle choices and workplace environments contribute significantly to injury risk. Improper footwear with inadequate lateral support, thin midsoles, or excessive heel elevation alters weight distribution and places undue strain on the cuboid. Workers in construction, landscaping, and hospitality often navigate uneven ground, slippery surfaces, and prolonged standing, creating a perfect storm for lateral foot injuries. Additionally, individuals with osteoporosis or vitamin D deficiency exhibit reduced bone mineral density, making the cuboid more susceptible to low-energy fractures. Environmental factors such as wet floors, poorly maintained stairs, and cluttered pathways further increase slip-and-fall probabilities. Action Step: Evaluate your daily footwear and replace worn-out athletic or work shoes every 300 to 500 miles. Incorporate calcium-rich foods and safe sun exposure to support bone density, and install anti-slip mats in high-traffic areas to mitigate environmental hazards.
Signs, Symptoms, and When to Seek Medical Evaluation
Early Warning Signals of a Cuboid Fracture
Identifying a broken cuboid bone early requires recognizing specific clinical patterns that distinguish it from generic foot discomfort. Patients typically report sharp, localized pain along the lateral midfoot that intensifies during weight-bearing, push-off movements, or when the outer foot is compressed. Swelling develops rapidly, often accompanied by ecchymosis (bruising) that tracks along the sole or dorsal surface within 24 to 48 hours. Tenderness upon direct palpation of the cuboid region is a hallmark sign, and many individuals experience difficulty wearing standard shoes due to lateral pressure. Some report a grinding or crepitus sensation when attempting to flex or extend the toes, indicating articular involvement or fragment movement. Importantly, pain that persists despite rest, ice, and over-the-counter anti-inflammatory medications warrants professional assessment. Practical Tip: Perform the "squeeze test" gently by compressing the forefoot and midfoot together. Reproduction of sharp lateral pain strongly suggests a cuboid injury and should prompt immediate clinical evaluation.
Distinguishing a Broken Cuboid Bone from Other Foot Conditions
Accurate differential diagnosis is essential because several foot pathologies mimic cuboid fracture symptoms. Lateral ankle sprains primarily involve the anterior talofibular and calcaneofibular ligaments, producing swelling around the lateral malleolus and pain during inversion. Peroneal tendonitis or subluxation generates discomfort behind the lateral ankle bone, often accompanied by snapping sensations during ankle rotation. Lisfranc injuries affect the tarsometatarsal joints, causing midfoot swelling, dorsal bruising, and pain that worsens with toe extension rather than lateral compression. Stress fractures of the fifth metatarsal base present similarly but localize more distally along the lateral foot edge. Clinical evaluation, combined with diagnostic imaging, remains the gold standard for confirmation. Action Step: If you experience lateral foot pain alongside numbness, tingling, cold toes, or inability to move the digits, seek emergency care immediately, as these symptoms may indicate neurovascular compromise or compartment syndrome.
Diagnostic Procedures and Medical Imaging
Clinical Examination and Palpation Techniques
A thorough physical assessment begins with a detailed patient history, focusing on the mechanism of injury, symptom onset, and previous foot trauma. Orthopedic specialists employ targeted palpation to identify precise areas of maximal tenderness over the cuboid. They evaluate range of motion at the ankle, subtalar, and midtarsal joints while observing for mechanical blocks or crepitus. Gait analysis, even with partial weight-bearing, reveals compensatory patterns such as excessive supination, shortened stride length, or toe-off avoidance. Special tests, including the midfoot compression test and plantar flexion stress examination, help isolate cuboid instability. Clinicians also assess skin integrity, capillary refill, and peripheral pulses to rule out vascular compromise. According to guidelines from the Cleveland Clinic, early identification of joint incongruity or ligamentous laxity directly influences treatment selection and prevents chronic midfoot instability.
Radiographic Imaging and Advanced Scans
Standard weight-bearing and non-weight-bearing radiographs serve as the initial diagnostic tool. Three orthogonal views—dorsoplantar, oblique, and lateral—allow visualization of the cuboid's articular surfaces, alignment with adjacent bones, and fracture lines. However, radiographic interpretation can be challenging due to overlapping bone shadows and complex midfoot anatomy. When standard X-rays appear inconclusive but clinical suspicion remains high, advanced imaging becomes necessary. Computed tomography (CT) scans provide high-resolution cross-sectional images that accurately map fracture displacement, intra-articular involvement, and comminution. Magnetic resonance imaging (MRI) excels at detecting bone marrow edema, stress reactions, ligament tears, and soft tissue injuries before complete fractures occur. Action Step: Always request weight-bearing radiographs when medically safe, as they reveal functional alignment issues and joint space narrowing that non-weight-bearing images may miss.
Comprehensive Treatment Pathways
Conservative Management and Immobilization Protocols
The majority of stable, non-displaced fractures heal successfully through conservative treatment. The foundational approach follows the RICE protocol—Rest, Ice, Compression, and Elevation—during the first 72 hours to control inflammation. Patients are placed in a controlled ankle motion (CAM) walker or a short-leg cast to restrict motion and offload the midfoot. Strict non-weight-bearing is typically enforced for 2 to 4 weeks, followed by a gradual transition to partial weight-bearing using crutches or a knee scooter. Compression sleeves and intermittent cryotherapy reduce post-immobilization stiffness and swelling. Pharmacological support includes scheduled NSAIDs for pain control, with careful consideration of gastrointestinal and renal risk factors. According to evidence from the Mayo Clinic, early protected motion after the initial immobilization phase prevents joint adhesions and promotes synovial fluid circulation. Practical Tip: Keep a recovery journal tracking pain levels, swelling measurements, and weight-bearing tolerance. This data provides valuable insights for your clinician to adjust your rehabilitation timeline safely.
Surgical Interventions for Displaced Fractures
When a broken cuboid bone presents with significant displacement, intra-articular step-offs greater than 2 millimeters, or associated tarsometatarsal instability, surgical management becomes necessary. Open reduction and internal fixation (ORIF) allows surgeons to anatomically realign bone fragments and secure them with lag screws, plates, or tension band constructs. In cases involving severe comminution or bone loss, structural bone grafts harvested from the iliac crest or allograft sources fill defects and promote osseous integration. Postoperative protocols emphasize strict elevation, wound monitoring, and delayed weight-bearing until radiographic evidence confirms early callus formation. Surgical candidates typically undergo intensive physical therapy once hardware stability is verified. Action Step: If surgery is recommended, inquire about your surgeon's fellowship training in foot and ankle orthopedics, discuss hardware removal timelines, and request a detailed postoperative care plan to optimize your recovery trajectory.
Pain Management and Adjunct Therapies
Effective pain control extends beyond oral medications. Intermittent cryotherapy applied for 15 to 20 minutes every two hours reduces inflammatory mediators and numbs superficial nerve endings. Transcutaneous electrical nerve stimulation (TENS) units provide non-pharmacological relief by interrupting pain signal transmission through the gate control mechanism. Gradual compression therapy using graduated medical socks prevents dependent edema and improves venous return. Mindfulness-based stress reduction, diaphragmatic breathing, and guided meditation lower cortisol levels, which can negatively impact bone healing if chronically elevated. Nutritional supplementation with vitamin C, magnesium, and omega-3 fatty acids supports tissue repair and reduces systemic inflammation. Practical Advice: Avoid combining multiple NSAIDs or exceeding recommended dosages without medical supervision. Consult a pain specialist if neuropathic symptoms or complex regional pain syndrome develop.
Recovery Timeline and Rehabilitation Strategies
Phased Return to Activity and Weight-Bearing Progression
Recovery from a broken cuboid bone follows a structured, phase-based approach tailored to radiographic healing and clinical milestones. Phase one focuses on inflammation control and complete offloading. Phase two introduces gentle ankle alphabets, towel scrunches, and isometric contractions to maintain neuromuscular activation. Phase three begins when imaging shows early callus formation, typically around week 4 to 6, initiating progressive weight-bearing in a supportive boot while monitoring pain responses. Phase four transitions to normal footwear with custom orthotics, incorporating balance training and proprioceptive drills. Returning to high-impact activities requires clearance from an orthopedic specialist and objective strength testing. Action Step: Use a standardized pain scale during rehabilitation. If pain exceeds a 3 out of 10 during or after exercises, reduce load, apply ice, and rest before progressing further.
Targeted Physical Therapy Exercises and Mobility Drills
Physical therapy plays a pivotal role in restoring function, preventing stiffness, and rebuilding dynamic stability. Clinicians prescribe toe yoga exercises to enhance intrinsic foot muscle activation, which stabilizes the transverse arch. Calf raises progress from bilateral to unilateral, eventually advancing to eccentric lowering to strengthen the Achilles and peroneal complexes. Resistance band inversions and eversions restore lateral ligament resilience, while wobble board and foam pad training recalibrate proprioception. Manual therapy techniques, including soft tissue mobilization and joint glides, address adhesions and restore midfoot flexibility. According to peer-reviewed studies indexed by NCBI, early controlled motion within pain-free ranges accelerates collagen alignment and reduces scar tissue formation. Practical Tip: Perform rehabilitation exercises in front of a mirror to ensure proper biomechanical alignment, and record sessions periodically to track range of motion improvements with your therapist.
Nutritional Support and Bone Healing Optimization
Bone regeneration demands substantial metabolic resources. Calcium remains the primary mineral for hydroxyapatite crystal formation, but it requires adequate vitamin D3 for intestinal absorption. Protein intake supports collagen matrix synthesis, with optimal recommendations ranging from 1.2 to 1.6 grams per kilogram of body weight daily. Vitamin K2 directs calcium deposition to bone tissue rather than vascular structures, while zinc and copper act as cofactors for enzymatic bone remodeling. Hydration maintains extracellular matrix viscosity and nutrient transport. Conversely, excessive alcohol consumption impairs osteoblast function, delays fracture union, and increases fall risk. Smoking introduces vasoconstrictive compounds that reduce peripheral blood flow and oxygen delivery to healing tissues. Action Step: Schedule a basic metabolic panel and vitamin D level test with your primary care provider to personalize your supplementation strategy safely and effectively.
Prevention Strategies and Long-Term Foot Care
Footwear Selection and Custom Orthotics
Preventing a broken cuboid bone begins with intelligent footwear choices. Shoes should feature a firm heel counter, adequate midfoot torsional rigidity, and cushioned midsoles that disperse impact forces evenly. Avoid minimalist footwear during transitional training phases, as sudden reductions in arch support increase midfoot stress. Custom orthotic devices correct biomechanical inefficiencies, redistribute pressure away from the lateral column, and enhance stability during dynamic movements. Over-the-counter insoles with metatarsal pads and medial arch supports serve as cost-effective alternatives for mild misalignments. Regular footwear inspection for sole compression, uneven wear patterns, or collapsed midsoles ensures continued protective functionality. Practical Tip: Have your feet measured professionally at the end of the day when swelling is maximal, ensuring optimal fit during your recovery and future athletic endeavors.
Biomechanical Adjustments and Strengthening Protocols
Addressing underlying biomechanical deficits reduces long-term injury susceptibility. Gait analysis using motion capture or treadmill video identifies excessive pronation, delayed toe-off, or asymmetrical loading patterns. Targeted strengthening of the gluteus medius, hip external rotators, and core stabilizers improves lower limb alignment, reducing compensatory midfoot stress. Dynamic stretching protocols enhance ankle dorsiflexion and foot intrinsic flexibility, preventing rigid lever arms that concentrate force. Proprioceptive training using single-leg balances and perturbation exercises recalibrate neuromuscular control, enabling rapid adjustments during unexpected surface changes. Consistency remains the most critical factor in biomechanical adaptation. Action Step: Incorporate two to three weekly sessions of hip and core strengthening into your routine, focusing on quality of movement rather than load progression.
| Treatment Approach | Indication | Immobilization Duration | Weight-Bearing Protocol | Typical Recovery Timeline | Key Considerations |
|---|---|---|---|---|---|
| Conservative Management | Non-displaced, stable fractures | 4-6 weeks in CAM boot or cast | Gradual progression from non-weight-bearing to full weight-bearing over 2 weeks | 6-10 weeks for clinical healing | Requires strict compliance; monitor for joint stiffness and muscle atrophy |
| Surgical Fixation (ORIF) | Displaced fragments, intra-articular involvement, multi-ligament injury | 4-8 weeks post-op in protective boot | Strict non-weight-bearing for 4-6 weeks, followed by phased loading | 3-6 months for full functional return | Hardware removal may be necessary; higher infection risk requires wound care |
| Stress Fracture Management | Early microtrauma, insidious onset, repetitive loading | 2-4 weeks in stiff-soled shoes or boot | Activity modification with protected weight-bearing immediately | 4-8 weeks with proper load management | Requires biomechanical correction to prevent recurrence |


Frequently Asked Questions
How long does it take for a broken cuboid bone to heal completely?
Healing typically requires 6 to 8 weeks for uncomplicated fractures, while complex or surgically treated injuries may take 3 to 6 months. Full remodeling of the bone structure can continue for up to 12 months, depending on patient compliance, nutritional status, and adherence to weight-bearing restrictions.
Can you walk with a broken cuboid bone?
Weight-bearing should generally be avoided in the acute phase to prevent displacement. Most clinicians prescribe a non-weight-bearing period followed by gradual loading in a controlled walking boot. Attempting to walk prematurely can delay healing, cause chronic instability, or require surgical intervention.
Is a broken cuboid bone considered a medical emergency?
While not always life-threatening, a broken cuboid bone requires prompt orthopedic evaluation. Open fractures, severe deformity, compromised circulation, or neurological symptoms demand immediate emergency care to prevent permanent damage or infection.
What is the difference between a cuboid fracture and a severe ankle sprain?
A cuboid fracture typically presents with localized midfoot pain on the outer foot, direct bone tenderness, and pain with lateral weight-bearing. Ankle sprains primarily affect lateral ligaments above the foot, causing joint swelling and pain that worsens with inversion. Imaging is required to definitively distinguish the two conditions.
Do all broken cuboid bones require surgery?
No. The majority of isolated cuboid fractures are stable and heal successfully with conservative management, including immobilization and protected weight-bearing. Surgery is reserved for displaced fragments, intra-articular involvement, multiple bone fractures, or failed conservative treatment after several weeks.
Conclusion
Navigating the recovery process for a broken cuboid bone demands patience, clinical guidance, and disciplined rehabilitation. The midfoot's complex architecture requires careful management to restore biomechanical harmony, prevent chronic instability, and ensure a safe return to daily activities and athletic pursuits. By recognizing early warning signs, adhering to evidence-based treatment protocols, optimizing nutrition, and committing to structured physical therapy, patients significantly improve their healing outcomes. Long-term prevention hinges on intelligent footwear choices, biomechanical corrections, and progressive strength training that fortify the foot against future trauma. Always consult a qualified orthopedic specialist or foot and ankle surgeon for personalized evaluations, and never underestimate the value of early intervention in midfoot injuries. With proper care and informed decision-making, full functional recovery remains highly achievable.
For additional clinical insights and evidence-based foot injury management, visit authoritative resources such as AAOS OrthoInfo, Mayo Clinic Foot & Ankle Health, and peer-reviewed research available through the National Center for Biotechnology Information. Prioritizing proactive foot care today ensures resilient mobility for tomorrow.

About the author
Samuel Jones, MD, is a board-certified orthopedic surgeon specializing in joint replacement and orthopedic trauma. He is a team physician for a professional sports team and practices at a renowned orthopedic institute in Georgia.