Brown Dots on Bottom of Feet: Comprehensive Causes, Diagnosis, and Treatment Guide

Discovering unexpected pigmentation changes on your soles can trigger immediate concern, especially when you notice brown dots on bottom of feet that refuse to fade with routine hygiene. While many skin variations are entirely benign and resolve without intervention, certain underlying conditions require prompt clinical evaluation to prevent complications or rule out serious pathology. Understanding the physiological mechanisms behind these pigmented spots, recognizing the subtle differences between harmless callus hemorrhages and potentially malignant lesions, and implementing targeted foot care strategies are essential steps in maintaining long-term dermatological and vascular health. This comprehensive guide explores the multifaceted causes, diagnostic protocols, and evidence-based treatment pathways for plantar pigmentation, empowering you with actionable insights to manage your foot health proactively. Whether you are an athlete, someone with diabetes, or simply observing natural skin changes, navigating these symptoms with medical accuracy and informed caution will help you make confident decisions about when self-care suffices and when professional intervention becomes necessary.
What Are Brown Dots on the Bottom of the Feet?
Defining the Appearance and Clinical Presentation
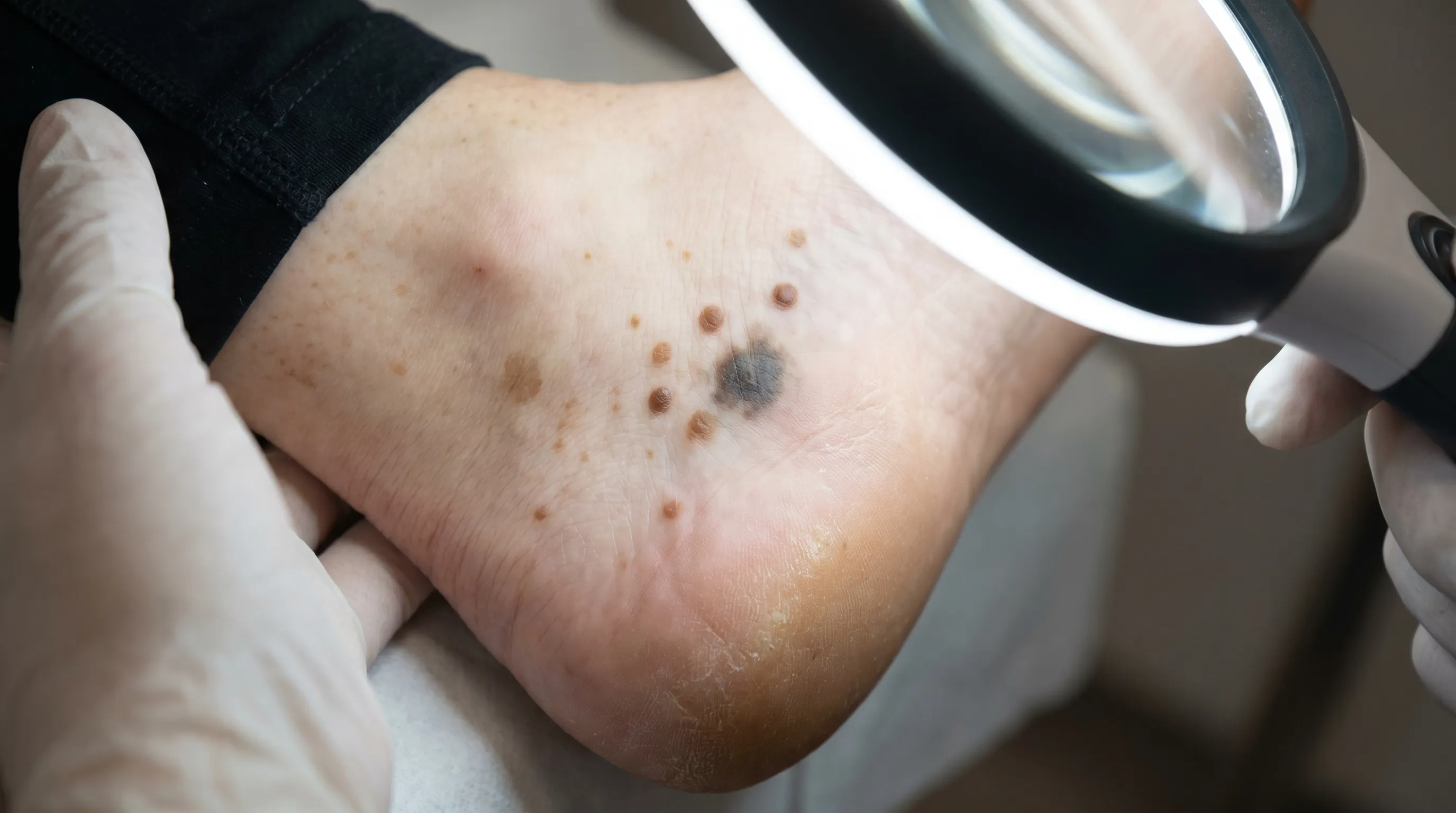
The human plantar surface contains specialized eccrine glands, thick stratum corneum, and dense vascular networks that react uniquely to mechanical stress, environmental exposure, and microbial activity. When you observe brown dots on bottom of feet, they typically present as discrete, hyperpigmented macules or papules ranging from one to five millimeters in diameter. These spots may appear uniformly distributed, clustered around pressure-bearing zones, or localized to the arches and heels. Their coloration stems from varying concentrations of melanin, oxidized hemoglobin, iron deposits from degraded red blood cells, or trapped keratinous debris. Dermatologists classify plantar pigmentation based on symmetry, border regularity, elevation, and response to dermoscopic lighting. Recognizing the precise morphology is crucial because similar-looking lesions can originate from completely distinct pathophysiological pathways, including viral infections, capillary fragility, fungal colonization, and malignant melanocytic proliferation.
How They Differ From Other Foot Lesions
Differentiating hyperpigmented plantar spots from common dermatoses like plantar warts, corns, blisters, or dermatophyte infections requires careful observation of texture and growth patterns. Unlike fungal tinea infections that typically produce scaly, annular borders and intense pruritus, isolated brown spots rarely exhibit significant flaking unless secondary eczema develops. Conversely, plantar warts caused by human papillomavirus often display a disrupted dermatoglyphic pattern with pinpoint black thrombosed capillaries visible after paring. Acral melanoma may mimic benign nevi initially but progressively demonstrates asymmetry, irregular borders, color variegation, diameter expansion, and evolving characteristics over weeks to months. Vascular petechiae, which result from capillary rupture due to pressure or coagulopathy, usually remain flat and non-blanching, whereas hemosiderin staining presents as rust-brown patches that slowly migrate as venous pressure normalizes. Accurate identification relies on tracking temporal changes, evaluating associated symptoms like pain or numbness, and correlating findings with systemic risk factors.
Common Medical Causes of Plantar Pigmentation
The etiology behind pigmented plantar lesions spans dermatological, vascular, infectious, and neoplastic categories. Each pathway follows distinct biological triggers, necessitating targeted diagnostic approaches and therapeutic interventions.
Plantar Warts and HPV-Induced Hyperpigmentation
Human papillomavirus infiltrates the epidermal layers through microscopic fissures in weight-bearing skin, stimulating rapid keratinocyte proliferation. As the viral infection progresses, capillaries grow inward to supply the hypertrophic tissue, eventually thrombosing and forming characteristic dark speckles. Patients frequently mistake these for foreign bodies or calluses, especially when pain emerges during ambulation. The resulting pigmentation typically aligns with disrupted skin lines and exhibits tenderness upon lateral compression rather than direct pressure. Salicylic acid preparations, cryotherapy, and immunomodulatory topicals remain first-line therapies, though viral clearance often requires sustained treatment regimens spanning several weeks to months. Maintaining foot hygiene, avoiding shared shower surfaces, and wearing moisture-wicking socks significantly reduce transmission risks.
Acral Lentiginous Melanoma and Malignant Melanocytic Changes
Representing a rare but clinically significant subtype of cutaneous melanoma, acral lentiginous melanoma arises on glabrous skin surfaces including palms, soles, and subungual regions. Unlike sun-exposed melanomas driven primarily by ultraviolet radiation, this variant occurs independently of cumulative sun damage and affects all Fitzpatrick skin types disproportionately. Early lesions manifest as slowly expanding, irregularly pigmented macules that gradually develop nodularity, ulceration, or satellite pigmentation. The presence of concerning lesions with asymmetrical borders, multiple color variations (tan, black, blue, red), and diameter exceeding six millimeters warrants immediate dermatoscopic evaluation. Genetic predisposition, atypical nevus syndrome, and immunosuppressive states increase susceptibility. Early excision with appropriate surgical margins remains the cornerstone of management, emphasizing why vigilant monitoring of new plantar pigmentation should never be dismissed as harmless dirt or bruising.
Petechiae, Capillaritis, and Microvascular Fragility
Microvascular rupture within the plantar dermis frequently produces pinpoint hemorrhages that oxidize into rust-brown or dark purple spots. This phenomenon, clinically termed pigmented purpuric dermatosis or capillaritis, results from increased hydrostatic pressure, mechanical trauma from prolonged standing, or underlying vasculitic processes. Individuals experiencing chronic venous insufficiency, orthostatic intolerance, or capillary wall inflammation commonly observe these specks following extended weight-bearing activities or ill-fitting footwear. Unlike coagulopathy-related petechiae that appear diffusely across dependent extremities, exercise-induced capillaritis typically localizes to high-friction zones. Management focuses on compression therapy, elevation protocols, and minimizing repetitive plantar impact. When accompanied by lower extremity edema, varicosities, or stasis dermatitis, comprehensive venous duplex ultrasonography helps differentiate benign microvascular leakage from progressive circulatory compromise.
Tinea Nigra and Superficial Fungal Colonization
Hortaea werneckii, a dematiaceous fungus endemic to tropical and subtropical coastal environments, colonizes the stratum corneum of the palms and soles, producing asymptomatic, sharply demarcated brown to black macules. Unlike dermatophyte infections that invade viable tissue and provoke inflammatory cascades, tinea nigra remains strictly superficial, relying on melanin production for photoprotection and environmental survival. The resulting pigmentation frequently raises alarm due to its resemblance to early melanoma, yet it effortlessly wipes away or scrapes off with gentle mechanical debridement. Diagnosis relies on potassium hydroxide preparation revealing septate hyphae and yeast cells, while topical antifungal agents like clotrimazole or terbinafine typically eradicate colonization within two to four weeks. Preventing recurrence involves thorough drying of interdigital spaces, rotating moisture-absorbent insoles, and avoiding barefoot exposure in humid communal environments.
Hemosiderin Staining, Punctate Hemorrhages, and Mechanical Trauma
Repetitive blunt impact from running, jumping, or wearing rigid-soled footwear fractures capillary networks beneath the thick plantar epidermis, releasing hemoglobin that subsequently degrades into hemosiderin. These iron-rich deposits manifest as discrete brown macules that persist long after the initial trauma resolves. Athletes and individuals with occupational standing requirements frequently develop these punctate hemorrhages, particularly beneath metatarsal heads and calcaneal fat pads. While inherently self-limiting, recurrent bleeding indicates inadequate shock absorption or gait abnormalities requiring podiatric assessment. Transitioning to cushioned footwear, incorporating orthotic inserts, and implementing structured rest periods facilitate vascular healing and prevent chronic hemosiderin accumulation.
Key Symptoms and Diagnostic Clues
Correlating visual findings with symptomatic presentation accelerates accurate diagnosis and guides appropriate clinical pathways.
Pain, Itching, and Sensory Changes
Benign mechanical punctate hemorrhages typically remain painless unless secondary inflammation develops, whereas viral plantar warts generate sharp, knife-like discomfort during stance phase gait. Fungal colonization rarely provokes significant symptoms unless complicated by secondary bacterial infection or allergic contact dermatitis from topical treatments. Malignant melanocytic proliferation usually remains asymptomatic until ulceration or nerve invasion occurs, underscoring the danger of relying solely on sensory feedback. Neuropathic patients with diabetic peripheral neuropathy frequently miss early warning signs, making scheduled self-inspections indispensable. Pruritic lesions combined with scaling, erythema, or interdigital maceration strongly suggest dermatophyte or candidal overgrowth, warranting targeted antimicrobial therapy.
When to Seek Professional Evaluation
Medical professionals recommend prompt clinical assessment when brown dots on bottom of feet demonstrate rapid expansion, irregular borders, color heterogeneity, or failure to resolve within three to four weeks of conservative care. Systemic symptoms like unexplained weight loss, lymphadenopathy, or new-onset joint pain may indicate broader immunological or vascular pathology. Individuals with diabetes mellitus, peripheral artery disease, or chronic corticosteroid usage face heightened risks for atypical wound healing and opportunistic infections, necessitating lowered thresholds for professional consultation. Any lesion that bleeds spontaneously, crusts persistently, or disrupts normal dermatoglyphic patterns requires dermoscopic examination and potential tissue sampling.
Clinical Diagnosis Process
Evidence-based dermatological evaluation integrates visual assessment, non-invasive imaging, and histopathological confirmation to differentiate benign pigmentation from malignant transformation.
Dermatoscopic Examination and Pattern Analysis
Reflectance confocal microscopy and polarized light dermoscopy reveal structural characteristics invisible to the naked eye. Parallel ridge patterns suggest melanocytic proliferation within acral skin, while globular or dotted vascular arrangements frequently indicate viral papillomas. Capillaritis presents with coiled capillary loops surrounded by faint brown hemosiderin halos, whereas superficial fungal infections display homogeneous brown pigmentation without structural disruption. Expert dermatoscopists utilize algorithmic frameworks like the three-point checklist, seven-point criteria, and acral melanoma specific scoring systems to standardize diagnostic accuracy and minimize false-negative rates.
Biopsy and Laboratory Testing
Excisional, punch, or shave biopsies provide definitive histopathological diagnosis when dermoscopic findings remain equivocal or malignant features predominate. Tissue specimens undergo hematoxylin and eosin staining, immunohistochemical profiling, and occasionally molecular sequencing to determine tumor thickness, mitotic rate, and genetic mutations like BRAF or KIT. Fungal cultures, direct microscopic examination with potassium hydroxide, and polymerase chain reaction assays rapidly identify dematiaceous organisms and dermatophyte species. Coagulation panels, complete blood counts, and metabolic profiles screen for underlying hematological disorders, nutritional deficiencies, or systemic vasculitis contributing to recurrent microvascular hemorrhage.
Imaging for Deep Tissue Assessment
High-resolution ultrasound evaluates soft tissue infiltration, vascular anomalies, and foreign body localization when clinical examination suggests deeper structural involvement. Magnetic resonance imaging with contrast enhances visualization of tendon sheath extension, bone marrow edema, or atypical soft tissue masses requiring surgical planning. While rarely indicated for simple hyperpigmented macules, advanced imaging becomes essential when brown dots on bottom of feet correlate with palpable nodules, restricted joint mobility, or progressive structural deformity.
Treatment Options and Management Strategies
Therapeutic interventions align with underlying pathophysiology, balancing rapid symptom resolution with long-term tissue preservation and recurrence prevention.
Over-the-Counter Remedies and Conservative Care
Salicylic acid keratolytics, urea-based emollients, and antifungal sprays address superficial viral, hyperkeratotic, and mycotic etiologies respectively. Proper application techniques include soaking the affected area to soften the stratum corneum, gently debriding excess tissue, and maintaining consistent daily treatment schedules. Mechanical cushioning pads, metatarsal sleeves, and custom orthotics redistribute plantar pressure, reducing capillary fragility and accelerating punctate hemorrhage resolution. Patients should avoid aggressive filing or unsterile cutting, which frequently introduces secondary bacterial colonization and delays epithelial regeneration.
Prescription Medications and Targeted Therapies
Cryotherapy with liquid nitrogen, cantharidin application, and intralesional bleomycin injections effectively eradicate recalcitrant plantar warts while minimizing scarring. Topical immunomodulators like imiquimod and diclofenac gel reduce inflammatory cascades and stimulate localized immune clearance. Antifungal prescriptions containing terbinafine or itraconazole penetrate deeply into keratinized layers, addressing resistant superficial infections within structured dosing protocols. Patients requiring long-term corticosteroid or immunosuppressive therapy often benefit from prophylactic antimicrobial regimens and enhanced foot hygiene routines to mitigate opportunistic colonization risks.
Surgical and Procedural Interventions
Wide local excision with appropriate safety margins remains the definitive treatment for confirmed acral lentiginous melanoma, often supplemented by sentinel lymph node mapping to evaluate metastatic potential. Laser ablation techniques using carbon dioxide, pulsed dye, or Nd:YAG wavelengths selectively target hyperpigmented lesions while preserving surrounding healthy tissue. Electrosurgical curettage, Mohs micrographic surgery, and advanced photodynamic therapy address complex dermatological presentations where cosmetic outcomes and functional preservation require specialized expertise. Postoperative care emphasizes strict wound protection, offloading protocols, and regular follow-up examinations to monitor healing trajectories and detect early recurrence.
Prevention and Daily Foot Care Tips
Sustainable plantar health requires proactive hygiene practices, biomechanical optimization, and consistent tissue monitoring.
Hygiene and Footwear Selection
Daily washing with mild, pH-balanced cleansers removes environmental debris, sweat accumulation, and microbial colonies without stripping natural epidermal lipids. Rotating footwear every forty-eight hours allows complete evaporation of trapped moisture, while breathable mesh uppers and antimicrobial linings significantly reduce fungal proliferation risk. Avoiding tight, non-supportive shoes prevents excessive shear forces that fracture capillary networks and stimulate compensatory hyperkeratosis. Selecting socks manufactured from merino wool or moisture-wicking synthetics maintains optimal microclimate conditions and minimizes friction-induced microtrauma.
Moisture Control and Skin Protection
Applying broad-spectrum emollients containing ceramides, glycerin, and hyaluronic acid reinforces the plantar stratum corneum barrier, reducing fissure formation and environmental irritant penetration. Antiperspirant powders and moisture-absorbent insoles manage hyperhidrosis, a primary catalyst for maceration and opportunistic pathogen colonization. When engaging in high-impact activities or occupational standing, silicone gel pads and graduated compression sleeves buffer plantar impact forces, stabilizing microvascular networks and preventing hemosiderin deposition. Consistent exfoliation with alpha-hydroxy acids or gentle foot files removes dead cellular accumulation that obscures early lesion development.
Monitoring Changes Over Time
Establishing a monthly self-inspection routine using high-resolution photography, natural lighting, and measurement reference cards enables precise tracking of pigmentation evolution. Recording lesion dimensions, color variations, border characteristics, and symptomatic shifts creates valuable longitudinal documentation that enhances clinical consultations. Utilizing standardized tracking applications or dedicated health journals reduces recall bias and facilitates rapid identification of concerning morphological changes. Sharing photographic timelines with dermatological or podiatric specialists accelerates diagnostic workflows and ensures evidence-based intervention timing.
| Etiological Category | Primary Mechanism | Typical Presentation | Recommended Initial Management | Prognosis |
|---|---|---|---|---|
| Plantar Warts (HPV) | Viral keratinocyte proliferation with thrombosed capillaries | Painful, disrupted skin lines, pinpoint black specks | Salicylic acid, cryotherapy, immunomodulators | Excellent with consistent treatment |
| Acral Lentiginous Melanoma | Malignant melanocytic mutation on glabrous skin | Asymmetrical, irregular borders, color variegation, evolving | Urgent biopsy, wide excision, sentinel node mapping | Depends on Breslow thickness and stage |
| Pigmented Purpuric Dermatoses | Capillary fragility and hemosiderin deposition | Flat, rust-brown macules, non-blanching, often symmetrical | Compression therapy, leg elevation, trauma avoidance | Generally self-limiting, chronic if untreated |
| Tinea Nigra | Superficial dematiaceous fungal colonization | Sharply demarcated, asymptomatic brown macules | Topical antifungals (clotrimazole, terbinafine) | Excellent, resolves within 2-4 weeks |
| Punctate Hemorrhages | Mechanical trauma and microvascular rupture | Localized brown spots under high-pressure zones | Footwear modification, cushioning, activity modification | Rapid resolution with pressure redistribution |
Frequently Asked Questions
Are brown dots on bottom of feet always cancerous?
No, the vast majority of pigmented plantar spots are benign and result from harmless mechanisms like mechanical trauma, viral warts, superficial fungal colonization, or hemosiderin staining from capillary fragility. While acral lentiginous melanoma can present similarly, it remains relatively rare compared to common dermatological conditions. Professional dermoscopic evaluation distinguishes malignant features from benign presentations, preventing unnecessary anxiety while ensuring early detection when warranted.
How long do punctate hemorrhages take to fade?
Microvascular punctate hemorrhages typically resolve spontaneously within two to six weeks as the body gradually reabsorbs extravasated blood and degrades hemosiderin deposits. The thick plantar epidermis slows visible turnover compared to thinner skin elsewhere on the body, making patience essential. Implementing pressure redistribution strategies, utilizing cushioned footwear, and avoiding repetitive high-impact activities accelerates the natural healing timeline and prevents recurrence.
Can diabetes cause hyperpigmentation on the soles?
Diabetes mellitus indirectly contributes to plantar pigmentation through multiple pathways, including chronic venous insufficiency, peripheral neuropathy, impaired wound healing, and increased susceptibility to fungal and bacterial infections. Autonomic neuropathy frequently alters sweat gland function, creating persistently dry or excessively moist environments that disrupt epidermal barrier integrity. Diabetic patients experiencing new or rapidly changing pigmentation should undergo comprehensive vascular and neurological assessments to identify underlying systemic complications.
Should I pop or file down suspicious plantar spots at home?
Attempting to excise, shave, or aggressively file undiagnosed plantar lesions carries significant risks, including secondary bacterial infection, deeper tissue invasion, accelerated viral spread, and delayed malignant diagnosis. Unsterile instruments and improper wound management frequently convert manageable conditions into complex dermatological emergencies. Consulting a licensed dermatologist or podiatrist ensures accurate identification through safe biopsy techniques and targeted treatment protocols tailored to your specific clinical presentation.
What daily habits prevent recurrence of plantar pigmentation?
Consistent preventive measures encompass daily gentle cleansing with pH-neutral products, thorough drying focusing on interdigital spaces, and regular application of barrier-reinforcing moisturizers. Rotating supportive footwear with adequate arch support and cushioning minimizes mechanical stress, while moisture-wicking socks regulate plantar microclimates and reduce fungal proliferation risk. Monthly self-examinations, prompt treatment of minor abrasions, and professional annual foot evaluations establish sustainable protective frameworks that maintain long-term dermatological health and vascular integrity.
Conclusion
Navigating the appearance of brown dots on bottom of feet requires a balanced approach that combines vigilant self-observation, informed symptom recognition, and timely professional consultation when concerning features emerge. While most plantar pigmentation originates from benign, easily manageable sources like viral infections, mechanical capillary fragility, or superficial fungal activity, the possibility of malignant transformation demands respectful attention and structured diagnostic pathways. Implementing evidence-based foot care routines, optimizing footwear mechanics, maintaining consistent hygiene practices, and avoiding aggressive self-treatment significantly reduce recurrence risks while preserving functional mobility. If you observe brown dots on bottom of feet after starting a new exercise routine, evaluate your footwear cushioning and gait alignment to mitigate excessive shear forces. Treatment success for brown dots on bottom of feet largely depends on accurate etiology identification and adherence to prescribed clinical protocols. Many patients ask whether brown dots on bottom of feet require surgical intervention, which remains true only for confirmed malignant lesions or deeply embedded foreign bodies. By prioritizing early clinical evaluation for evolving lesions, tracking morphological changes systematically, and integrating preventive dermatological habits into daily routines, individuals can confidently manage plantar skin health and maintain optimal lower extremity function throughout their lifespan. Trust your observations, respect clinical guidance, and approach foot care as an essential component of overall wellness rather than an afterthought. Consult authoritative medical resources like the American Academy of Dermatology and the Mayo Clinic Melanoma Guidelines for further evidence-based protocols and clinical updates.

About the author
Elena Vance, MD, is a double board-certified dermatologist and pediatric dermatologist. She is an assistant professor of dermatology at a leading medical university in California and is renowned for her research in autoimmune skin disorders.