Why Your Knee Keeps Popping: Causes, Treatments, and When to Worry

You might be climbing stairs, walking through the grocery store, or simply shifting positions on the couch when it happens again: a distinct click, crack, or pop resonates from your knee joint. For many adults, this phenomenon is an everyday occurrence that raises more questions than answers. While the sensation can be momentarily startling or mildly frustrating, understanding the underlying mechanics is essential for separating harmless joint noise from potential warning signs. The human knee is a complex biomechanical hinge that bears up to six times your body weight during basic movements, making it highly susceptible to wear, alignment shifts, and soft tissue changes, as noted by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS). When a knee keeps popping repeatedly, it often reflects a disruption in the smooth gliding mechanics that normally keep your lower extremity functioning painlessly. Whether you are an athlete, a busy professional, or someone navigating age-related joint changes, learning why this occurs and how to address it proactively can make the difference between chronic discomfort and lifelong mobility. This comprehensive guide explores the science behind joint sounds, identifies the most common triggers, outlines evidence-based treatment pathways, and provides actionable self-care strategies to help you restore confidence in every step. By integrating clinical insights with practical daily adjustments, you can take control of your knee health and minimize unnecessary worry or restrictive lifestyle changes.
Understanding Knee Crepitus: What Does It Actually Mean?
The medical term for joint popping, cracking, or grinding is crepitus. It is a broad descriptor used by clinicians to classify audible or tactile sensations occurring within joints during movement (Cleveland Clinic). While many associate crepitus exclusively with aging or injury, research demonstrates that it is a normal physiological occurrence across all age groups. Synovial joints like the knee contain lubricating fluid that nourishes cartilage and reduces friction. Over time, changes in tissue composition, muscle tension, and joint alignment can amplify these natural sounds, making them more noticeable. When patients report that their knee keeps popping, they are typically describing either harmless physiological noise or early indicators of mechanical dysfunction. Distinguishing between the two requires a foundational understanding of joint anatomy, fluid dynamics, and soft tissue behavior under varying loads.
The Anatomy Behind the Sound
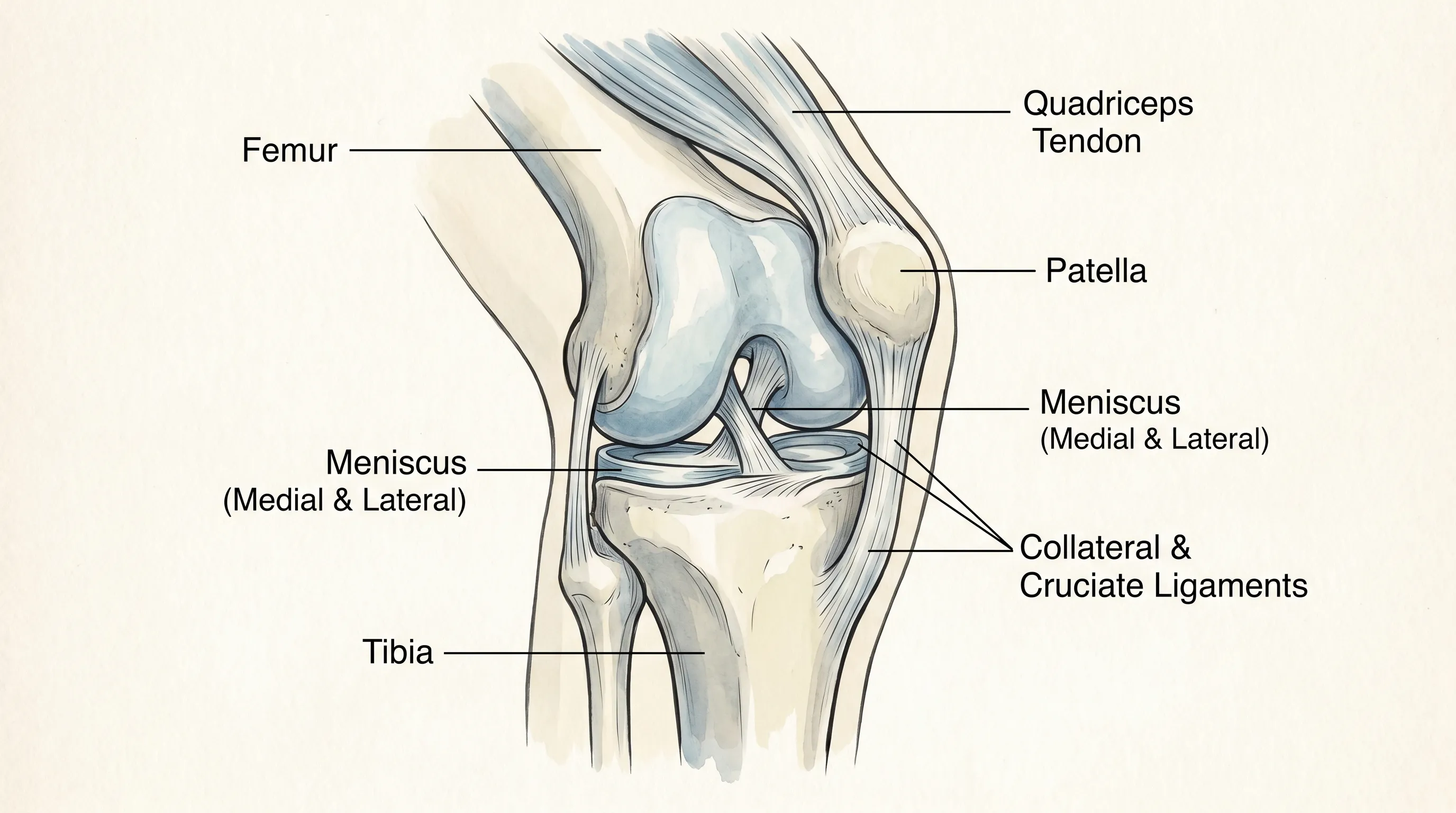
The knee joint is formed by the articulation of the distal femur, proximal tibia, and patella. These bones are cushioned by two C-shaped menisci that distribute weight, absorb shock, and stabilize the joint capsule. Surrounding ligaments—including the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), and lateral collateral ligament (LCL)—maintain structural integrity, while tendons connect powerful thigh and calf muscles to bone. The joint is enclosed in a synovial membrane that secretes hyaluronic acid-rich fluid, creating a low-friction environment. When movement occurs, tendons glide over bony landmarks, cartilage surfaces compress and decompress, and dissolved gases within the synovial fluid undergo pressure changes. Each of these processes can generate sound. The frequency, volume, and sensation of popping depend on individual biomechanics, muscle balance, hydration levels, and cumulative joint stress. Understanding this intricate network clarifies why isolated popping rarely signifies catastrophic damage unless accompanied by functional impairment.
Crepitus vs. Pathological Popping
Not all knee noises are created equal. Physiological crepitus is typically painless, intermittent, and reproducible without joint instability. It often feels like a gentle bubble popping or a soft snap that resolves immediately. Pathological popping, on the other hand, correlates with tissue irritation, structural compromise, or inflammatory processes. Patients experiencing pathological sounds frequently describe grinding, catching, or grinding sensations paired with stiffness, swelling, or giving way. The distinction lies in symptom complexity and functional impact. Evidence from orthopedic literature indicates that asymptomatic crepitus does not accelerate joint degeneration or predict future arthritis (Mayo Clinic). However, when abnormal tracking, meniscal tears, or progressive cartilage loss occur, the acoustic profile changes dramatically. Recognizing this difference prevents unnecessary anxiety while ensuring timely intervention when true mechanical failure develops. If your knee keeps popping during routine activities but never interferes with walking, squatting, or climbing, it is likely a benign adaptation to normal wear and tissue remodeling.
Why Your Knee Keeps Popping: Common Causes Explained
Multiple physiological and structural factors can trigger repetitive knee noises. Identifying the primary driver helps guide appropriate management strategies. While some causes require professional evaluation, others respond well to targeted self-care and movement modification. Below are the most clinically documented mechanisms responsible for persistent knee popping.
Gas Cavitation (The Harmless Pop)
Gas cavitation accounts for the majority of painless joint sounds. Synovial fluid contains dissolved nitrogen, oxygen, and carbon dioxide. When the joint capsule stretches rapidly during flexion or extension, intra-articular pressure drops suddenly, causing gas molecules to coalesce into microscopic bubbles. These bubbles collapse or pop instantaneously, producing a sharp cracking noise. This phenomenon, known as tribonucleation, follows a refractory period; you cannot reproduce the same sound immediately because the gases require time to redissolve. Studies using high-speed ultrasound and MRI confirm that cavitation does not damage cartilage or inflame tissues (Mayo Clinic). It is a natural byproduct of joint lubrication and mobility. People who notice their knee keeps popping after prolonged sitting, sudden standing, or light stretching are typically experiencing harmless cavitation. Regular movement prevents fluid stagnation and maintains optimal joint hydration, reducing the frequency of dramatic gas releases.
Tendon or Ligament Snapping
Soft tissues surrounding the knee do not always glide silently over bony prominences. The iliotibial band, patellar tendon, hamstring tendons, and medial hamstring tendons can catch or snap as they move across the lateral femoral condyle or medial tibial plateau. This snapping is more prevalent when muscles are tight, fatigued, or imbalanced. Repetitive flexion-extension cycles without adequate warm-up increase friction between tendons and underlying bone. Athletes, runners, and individuals who transition rapidly from sedentary to active lifestyles often report this sensation. Unlike gas cavitation, tendon snapping may feel more tactile and sometimes produces mild irritation at the contact point. Strengthening hip abductors, improving quadriceps flexibility, and implementing gradual loading protocols significantly reduce tendon tracking abnormalities. If your knee keeps popping primarily during deep knee bends or prolonged walking, soft tissue friction is a highly probable contributor.
Patellofemoral Tracking Issues
The patella must glide smoothly within the trochlear groove of the femur to maintain efficient force transmission during leg extension. When muscular imbalances, foot pronation, or structural variations disrupt this alignment, the kneecap tilts, shifts, or tracks laterally. Maltracking causes uneven cartilage pressure, tendon strain, and audible grinding or popping during stair negotiation, squatting, or rising from chairs. Vastus medialis obliquus (VMO) weakness relative to lateral quadriceps dominance is a common culprit, particularly in women due to wider pelvic anatomy (Cleveland Clinic). Over time, improper tracking accelerates cartilage wear and increases inflammation within the suprapatellar pouch. Physical therapy focusing on hip external rotation strengthening, neuromuscular control drills, and patellar taping techniques frequently restores smooth tracking. Addressing kinetic chain deficits upstream from the knee often resolves recurrent popping without invasive intervention.
Meniscus Tears and Joint Surface Damage
The meniscus acts as a shock absorber and stabilizer between the femur and tibia. Degenerative tears from chronic wear or acute tears from twisting injuries can displace fragment tissue into the joint space. When movement forces these displaced pieces between articulating surfaces, patients experience sudden popping, catching, or locking. Unlike harmless cavitation, meniscal sounds are often accompanied by joint line tenderness, intermittent swelling, and mechanical symptoms that limit full range of motion. Large displaced fragments or root tears may require arthroscopic evaluation, while smaller degenerative tears frequently respond to conservative rehabilitation. Magnetic resonance imaging remains the gold standard for visualizing meniscal integrity and cartilage thickness. If your knee keeps popping after a specific injury or feels unstable during pivoting movements, professional assessment is warranted to rule out structural compromise that could progress without targeted management (Cleveland Clinic).
Arthritis and Degenerative Changes
Osteoarthritis progressively thins articular cartilage, exposing underlying bone and altering joint congruency. As cartilage loses its smooth, glass-like surface, bones glide over irregularities that generate grinding, cracking, or persistent popping. Synovial fluid viscosity decreases, inflammation increases, and osteophyte formation alters normal biomechanics. While arthritis does not always produce noticeable sounds, degenerative changes frequently amplify joint noise, particularly during weight-bearing activities or temperature fluctuations (CDC). Rheumatoid arthritis and other inflammatory conditions add synovial proliferation and pannus formation to the equation, further disrupting smooth articulation. Managing inflammatory load, maintaining muscle mass, and utilizing joint-friendly movement patterns slow degenerative progression. Anti-inflammatory nutrition, low-impact conditioning, and medical supervision optimize function even when structural changes are present. Understanding that arthritis-related popping reflects adaptation rather than imminent failure helps patients maintain active lifestyles while receiving appropriate symptom management.
When Should You Be Concerned? Red Flags to Watch For
Painless popping rarely warrants alarm, but certain symptom patterns signal underlying pathology requiring professional evaluation. Recognizing these red flags prevents delayed treatment and reduces the risk of secondary complications. Joint health monitoring should prioritize functional capacity over isolated acoustic events.
Pain Accompanying the Sound
The presence of pain fundamentally alters the clinical significance of joint noise. Sharp, shooting, or deep aching discomfort that coincides with popping suggests tissue irritation, inflammation, or structural compromise. Pain that worsens with specific movements, persists at rest, or disrupts sleep indicates active pathology rather than benign crepitus. Inflammatory conditions like synovitis, bursitis, or early osteoarthritis generate chemical mediators that sensitize nerve endings, making normally silent movements painful. Tracking pain location, intensity, duration, and movement correlation helps clinicians isolate affected structures. Persistent pain should never be dismissed as normal aging, especially if it limits daily activities or alters gait patterns (Mayo Clinic).
Swelling, Stiffness, or Locking
Post-activity swelling lasting more than 48 hours suggests intra-articular effusion, typically triggered by meniscal tears, ligament sprains, or synovial irritation. Stiffness that persists beyond morning hours or develops after brief inactivity points toward inflammatory arthritis or cartilage degradation. Mechanical locking—where the knee temporarily refuses to straighten or bend—often indicates displaced tissue fragments blocking joint articulation. These symptoms demand clinical evaluation to prevent further joint damage and restore normal kinematics. Early intervention through imaging, aspiration, or targeted rehabilitation yields significantly better long-term outcomes than delayed management.
Recent Trauma or Injury History
Acute trauma alters joint biomechanics instantly. Falls, sports collisions, sudden direction changes, or heavy lifting incidents can stretch, partially tear, or fully rupture stabilizing tissues. Even seemingly minor impacts may initiate microtrauma that accumulates into symptomatic dysfunction. If your knee keeps popping following an injury, professional assessment rules out occult fractures, ligament laxity, or meniscal displacement. Ignoring post-traumatic noises increases reinjury risk and accelerates compensatory movement patterns that strain adjacent joints. Prompt rehabilitation restores proprioception, strengthens supporting musculature, and establishes safe return-to-activity protocols tailored to individual recovery trajectories.

Diagnostic Approaches: How Professionals Evaluate the Issue
Accurate diagnosis requires systematic assessment that integrates patient history, physical examination findings, and diagnostic imaging. Clinicians use standardized protocols to differentiate benign crepitus from structural pathology, ensuring treatment aligns with actual tissue status.
Physical Examination and Movement Assessment
Orthopedic and sports medicine professionals begin with comprehensive palpation, range-of-motion testing, and functional movement screens. They assess patellar mobility, joint line tenderness, ligamentous stability, and muscle strength ratios. Special tests like the McMurray maneuver, Lachman test, and patellar grind assessment help isolate specific structures. Observing gait mechanics, squat depth, and single-leg balance reveals kinetic chain deficiencies that contribute to abnormal joint loading. Dynamic palpation during active movement identifies reproducible popping triggers. Clinicians document pain provocation, swelling presence, and functional limitations to establish baseline metrics for monitoring progress.
Imaging Studies (X-Rays, MRI, Ultrasound)
Radiographic evaluation provides structural clarity when clinical suspicion indicates tissue damage. Weight-bearing X-rays reveal joint space narrowing, osteophyte formation, alignment deviations, and bone quality. Magnetic resonance imaging offers unparalleled soft tissue visualization, detecting meniscal tears, ligament integrity, cartilage defects, and synovial abnormalities. Diagnostic ultrasound dynamically assesses tendon movement, bursa inflammation, and joint effusion in real-time. Clinicians order imaging selectively to avoid unnecessary exposure and healthcare costs. Results directly inform treatment pathways, distinguishing conservative rehabilitation candidates from those requiring procedural or surgical intervention.
Gait Analysis and Biomechanical Testing
Advanced clinics utilize motion capture technology, force plates, and pressure-mapping insoles to quantify lower extremity loading patterns. Gait analysis identifies pronation, supination, limb length discrepancies, and compensatory strategies that increase knee stress. Biomechanical testing reveals muscle activation timing deficits, joint stiffness ratios, and kinetic energy transfer inefficiencies. Data guides individualized exercise prescriptions, orthotic recommendations, and activity modification strategies. Integrating movement science with clinical examination ensures comprehensive management that addresses root causes rather than isolated symptoms. When your knee keeps popping due to movement inefficiency, targeted biomechanical correction frequently eliminates the problem without pharmacological or invasive measures.
Treatment and Management Strategies
Effective management depends entirely on symptom complexity, structural integrity, and individual functional goals. Treatment progresses from conservative self-care to targeted rehabilitation, with procedural options reserved for refractory cases or significant mechanical disruption.
Conservative Care and Lifestyle Modifications
First-line management emphasizes activity modification, load management, and ergonomic optimization. Patients learn to avoid movements that consistently trigger painful popping while maintaining joint mobility through controlled ranges. Weight reduction decreases compressive forces on articular surfaces, dramatically reducing grinding and inflammation. Proper warm-up routines increase synovial fluid viscosity, improving joint lubrication before intense activity. Incorporating micro-breaks during prolonged sitting or standing prevents tissue stiffening and promotes circulation. Environmental adjustments like cushioned flooring, supportive seating, and temperature regulation minimize external joint stress. These foundational changes create a favorable healing environment while preventing symptom exacerbation.
Physical Therapy and Targeted Exercises
Evidence-based rehabilitation remains the cornerstone of knee management programs. Therapists design progressive loading protocols that strengthen quadriceps, hamstrings, gluteals, and core stabilizers without aggravating tissues. Closed-chain exercises like mini-squats, step-ups, and leg presses build functional strength while maintaining joint congruency. Open-chain movements like straight leg raises and terminal knee extensions target specific muscle groups with controlled resistance. Neuromuscular retraining improves proprioception, reducing abnormal tracking patterns. Flexibility protocols address tight IT bands, calves, hip flexors, and hamstrings that pull joints out of alignment. Blood flow restriction training and aquatic therapy provide low-impact strengthening alternatives for highly symptomatic individuals. Consistency over intensity drives long-term structural adaptation and symptom reduction (CDC).
Medical Interventions and Injections
When conservative measures yield insufficient relief, clinicians consider targeted pharmaceutical or procedural options. Nonsteroidal anti-inflammatory drugs reduce acute inflammation and pain, facilitating participation in rehabilitation programs. Hyaluronic acid viscosupplementation injections temporarily improve joint lubrication, particularly in early osteoarthritis. Corticosteroid injections provide short-term inflammation suppression for acute flare-ups but require careful dosing to avoid cartilage compromise. Platelet-rich plasma therapy and stem cell injections show promising regenerative potential, though long-term efficacy data remains under investigation. Orthobiologics aim to modulate inflammatory cascades and support tissue healing in selected patients. Medical professionals weigh risks, benefits, and individual response patterns before recommending procedural intervention.
Surgical Options for Severe Cases
Surgical intervention addresses structural failures that resist conservative management. Arthroscopic debridement removes loose fragments, smooths irregular cartilage, and repairs manageable meniscal tears. Meniscectomy or meniscal repair preserves long-term joint health by restoring shock absorption capacity. Cartilage restoration techniques like microfracture, autologous chondrocyte implantation, or osteochondral grafting address focal defects in younger patients. Osteotomy realigns malpositioned joints to shift load away from damaged compartments, delaying degenerative progression. Total joint arthroplasty remains reserved for end-stage arthritis with severe pain and functional disability. Surgical decisions involve multidisciplinary consultation, risk-benefit analysis, and realistic expectation setting. Postoperative rehabilitation requires strict adherence to phased protocols to optimize tissue healing and restore functional independence.
Home Care and Self-Management Tips
Sustainable knee health depends on daily habits that support joint integrity, reduce inflammatory load, and promote muscular balance. Integrating these evidence-based practices into your routine creates lasting improvements without relying solely on clinical interventions.
Daily Mobility Routines
Establishing consistent mobility practices prevents tissue adhesions and maintains optimal joint lubrication. Begin each morning with gentle ankle pumps, knee extensions, and hip circles to stimulate synovial fluid circulation. Perform controlled patellar mobilizations by gently shifting the kneecap side-to-side while the leg is straight and relaxed, improving tracking mechanics. Incorporate dynamic warm-ups before activity, focusing on glute activation, hamstring lengthening, and calf mobility. End each day with light stretching, focusing on the quadriceps, IT band, and hip flexors to reduce cumulative tension. Use foam rollers sparingly on thick muscle bellies, avoiding direct pressure over bones or inflamed tendons. Regular mobility practice maintains joint health and reduces the likelihood of stiffness-related popping.
Footwear and Support Considerations
Proper footwear dramatically influences lower extremity alignment and joint loading patterns. Replace athletic shoes every 300–500 miles when midsole cushioning compresses and shock absorption declines. Select shoes with appropriate arch support matching your foot type to prevent excessive pronation or supination. Consider over-the-counter or custom orthotics if structural deviations cause persistent discomfort. Avoid worn-out heels, flat unsupportive sandals, or shoes that force the foot into unnatural angles during daily wear. Use knee sleeves or patellar straps during high-demand activities to enhance proprioceptive feedback and reduce tissue strain. Proper support systems create stable foundations that minimize compensatory knee stress and abnormal tracking.
Nutrition for Joint Health
Dietary choices directly influence inflammation levels, cartilage integrity, and tissue repair capacity. Prioritize omega-3 fatty acids from fatty fish, flaxseeds, and walnuts to modulate inflammatory pathways. Increase colorful vegetable and fruit intake for antioxidant protection against cellular degradation. Maintain adequate protein consumption to support muscle maintenance and connective tissue remodeling. Stay consistently hydrated to preserve synovial fluid viscosity and cartilage hydration. Consider evidence-based supplements like collagen peptides, glucosamine-chondroitin blends, or curcumin extracts after consulting healthcare providers, as individual responses vary (Cleveland Clinic). Reducing processed sugars, refined carbohydrates, and excessive alcohol lowers systemic inflammation that exacerbates joint symptoms. Nutritional optimization supports structural resilience and enhances rehabilitation outcomes.
| Symptom Profile | Likely Mechanism | Recommended First Step | When to Seek Medical Care |
|---|---|---|---|
| Painless popping during extension | Gas cavitation, tendon gliding | Maintain mobility routine, warm up properly | Never, unless function changes |
| Grinding with mild stiffness after activity | Early cartilage wear, tracking shift | Begin quad/hip strengthening, optimize footwear | If stiffness persists >2 weeks or swelling occurs |
| Sharp pop followed by immediate swelling | Ligament strain, meniscal tear, acute injury | Rest, ice, compression, elevation (RICE protocol) | Immediately for instability or inability to bear weight |
| Catching/locking with intermittent pain | Displaced tissue fragment, mechanical block | Modify activities, avoid deep flexion | Prompt evaluation to prevent secondary damage |
| Persistent crunching with morning stiffness | Degenerative changes, inflammatory process | Anti-inflammatory nutrition, gentle daily movement | If functional limitation worsens or pain disrupts sleep |
Frequently Asked Questions
Is it normal for my knee to pop without pain?
Yes, painless knee popping is extremely common and typically harmless. It often results from nitrogen gas bubbles releasing in the synovial fluid or tendons gliding over bony prominences. If there is no swelling, instability, or functional limitation, it rarely indicates structural damage. Research consistently shows that asymptomatic crepitus does not accelerate joint degeneration or predict future arthritis onset.
Can weak muscles cause my knee to pop more frequently?
Absolutely. Weakness in the quadriceps, hamstrings, or hip stabilizers can alter patellar tracking and joint biomechanics. When the kneecap does not glide smoothly through its femoral groove, tendons snap, and cartilage surfaces experience uneven pressure, leading to increased crepitus and popping sensations. Targeted strengthening restores alignment and significantly reduces abnormal joint sounds.
Does arthritis always cause knee popping?
While osteoarthritis frequently produces grinding or cracking sounds due to cartilage deterioration, not everyone with arthritis experiences noticeable popping. Conversely, many people with arthritis have quiet joints. The presence or absence of noise does not directly correlate with disease severity. Symptom management focuses on function, pain control, and maintaining mobility rather than eliminating acoustic changes.
When should I see a doctor for knee popping?
Seek medical evaluation if the popping is accompanied by persistent pain, sudden swelling, joint locking or giving way, visible deformity, or a history of acute trauma (Mayo Clinic). These symptoms suggest structural injury or inflammation that requires professional assessment and targeted intervention. Early diagnosis prevents secondary complications and guides appropriate treatment pathways.
What exercises help reduce knee popping safely?
Low-impact strengthening exercises such as straight leg raises, clamshells, wall sits, and controlled step-ups improve joint stability and muscle balance. Stretching tight IT bands, hamstrings, and calves also promotes smoother tracking. Always progress gradually and avoid high-impact or deep flexion movements during acute flare-ups. Consistency and proper form drive lasting biomechanical improvements.
Can footwear choices impact knee popping?
Yes. Shoes with poor arch support, worn-out cushioning, or incorrect heel height alter lower extremity alignment, increasing torsional stress on the knee joint. Proper footwear with adequate shock absorption and biomechanical alignment significantly reduces abnormal joint forces that contribute to crepitus and discomfort. Regular shoe replacement and activity-specific selection protect joint integrity long-term.
Conclusion
Noticing that your knee keeps popping can trigger uncertainty, but understanding the underlying mechanisms transforms anxiety into informed action. Most joint sounds stem from harmless physiological processes like gas cavitation or tendon gliding that require minimal intervention beyond consistent mobility and strength maintenance. When popping coincides with pain, swelling, instability, or mechanical blockage, it signals the need for professional evaluation and targeted rehabilitation. By prioritizing muscle balance, optimizing footwear, managing inflammatory load, and implementing evidence-based movement protocols, you can significantly improve joint function and reduce disruptive symptoms. Knee health thrives on consistency, proper load management, and proactive self-care rather than reactive crisis management. Integrating daily mobility routines, targeted strengthening, and smart lifestyle modifications creates a resilient foundation that supports lifelong activity. Whether your sounds are entirely benign or early indicators of mechanical shift, taking deliberate, informed steps ensures your knees continue carrying you forward with confidence and comfort for years to come.

About the author
Samuel Jones, MD, is a board-certified orthopedic surgeon specializing in joint replacement and orthopedic trauma. He is a team physician for a professional sports team and practices at a renowned orthopedic institute in Georgia.