Why Your Knee is Locking Up: A Comprehensive Guide to Causes and Treatment

Key points
- Inability to bear any weight on the affected leg: This suggests significant structural damage, such as a fracture, severe ligament rupture, or acute meniscal extrusion.
- Severe or escalating pain and swelling: Rapidly progressive swelling within the first 6 hours of injury often indicates hemarthrosis, which requires professional drainage and evaluation.
- The knee remains locked and cannot be unlocked with gentle motion: Prolonged mechanical locking can lead to secondary joint capsule contractures and cartilage degeneration if the obstruction is not surgically addressed.
- You heard a loud "pop" at the moment of injury: Audible pops are classic signs of ligamentous rupture (especially ACL), meniscal tears, or patellar dislocation.
- Signs of infection, such as fever, chills, profound redness, or localized warmth around the knee: Septic arthritis is a medical emergency that can rapidly destroy joint cartilage within days if untreated with intravenous antibiotics and joint lavage.
- Numbness, tingling, or coldness in the lower leg or foot: These neurovascular symptoms may indicate compromised blood flow or nerve impingement, requiring immediate emergency intervention.
That sudden, jarring sensation when your knee gets stuck, refusing to bend or straighten, is more than just an inconvenience—it can be painful and deeply unsettling. This experience, known as a "locked knee," is a common complaint that can stem from a variety of causes, ranging from a minor muscle spasm to a significant joint injury. According to epidemiological studies, knee joint complaints account for nearly 30% of all orthopedic visits, with mechanical symptoms like locking, catching, and giving way representing a substantial subset of these presentations. Whether you are an athlete pushing through a demanding training regimen or an older adult managing age-related wear and tear, understanding the mechanics behind this symptom is essential for preserving mobility and quality of life.
Understanding why your knee is locking is the first step toward finding relief and preventing it from happening again. The knee is a complex hinge joint that bears up to four times your body weight during routine activities like walking or climbing stairs. When any component within or surrounding this intricate system becomes compromised, the joint's smooth gliding mechanics can quickly break down. This comprehensive guide will walk you through the different types of knee locking, their common causes, and the full spectrum of treatment options, from at-home care to advanced medical procedures.
Understanding Knee Locking: Is It a True Block or a Pain Response?
The first crucial step in diagnosing a locked knee is to determine whether you are experiencing a true mechanical lock or a "pseudo-lock." While they feel similar to the untrained patient, their underlying causes, pathophysiology, and treatments are very different. Misidentifying the type of lock can lead to inappropriate self-treatment or delayed medical intervention, potentially worsening the underlying condition.
What is True Mechanical Knee Locking?
True knee locking occurs when a physical object inside the knee joint mechanically blocks its movement, much like a pebble jamming a door hinge. The knee becomes physically stuck in one position, typically at a partially flexed angle between 20 and 40 degrees, and no amount of conscious muscular effort can move it past that point. This blockage is often caused by a displaced piece of tissue or bone. In true mechanical locking, the joint's articular surfaces cannot glide past one another because an interposed structure creates a physical barrier. Patients often describe this sensation with very specific mechanical terms: "something caught," "a doorstop in the joint," or "a physical blockage." Unlocking a true mechanical lock sometimes requires specific maneuvers, such as rotating the tibia or gently shaking the leg, which physically dislodges the offending tissue back into its resting position.
What is Pseudo Knee Locking?
Pseudo-locking is the sensation of the knee being locked, but without a physical obstruction. The immobility is actually a protective neurological and musculoskeletal response from your body. Severe pain from an injury or inflammation can trigger intense muscle spasms around the knee, causing it to seize up to prevent further damage. This phenomenon, often termed "arthrogenic muscle inhibition" or "reflex muscle guarding," occurs when nociceptors (pain receptors) in the joint capsule, ligaments, or synovium send rapid distress signals to the central nervous system. The nervous system responds by involuntarily contracting the surrounding musculature, particularly the quadriceps and hamstrings, to splint the joint. The knee isn't truly blocked, but the pain, swelling, and profound stiffness make it feel functionally immobilized. Unlike true mechanical locking, pseudo-locking tends to improve gradually as inflammation subsides, pain medications take effect, or the patient consciously relaxes the guarding muscles.
| Feature | True Mechanical Locking | Pseudo Locking |
|---|---|---|
| Primary Cause | Physical obstruction (e.g., torn cartilage, loose bone fragment) | Severe pain and protective muscle spasms |
| Sensation | Feeling of something physically catching or blocking the joint | A general inability to move due to intense pain or stiffness |
| Movement | The knee is stuck at a specific angle and cannot be moved further | Range of motion may be restored if pain and spasms ease |
| Onset | Often sudden, may occur with a "pop" or "click" | Can develop gradually with increasing pain and inflammation |
Clinical differentiation between these two presentations heavily relies on the patient's history and a skilled physical examination. Imaging studies like MRI are then utilized to confirm the suspected diagnosis. Understanding which category your symptoms fall into will dictate whether conservative rehabilitation is appropriate or if surgical consultation is warranted.
Common Causes of a Locked Knee
The cause of your locked knee is directly related to whether it is a true mechanical block or a pseudo-lock. Anatomically, the knee consists of three bones (femur, tibia, patella), two primary menisci, four major ligaments, multiple bursae, and an intricate network of tendons and synovial tissue. Pathology in any of these structures can precipitate locking symptoms.
Causes of True Mechanical Locking
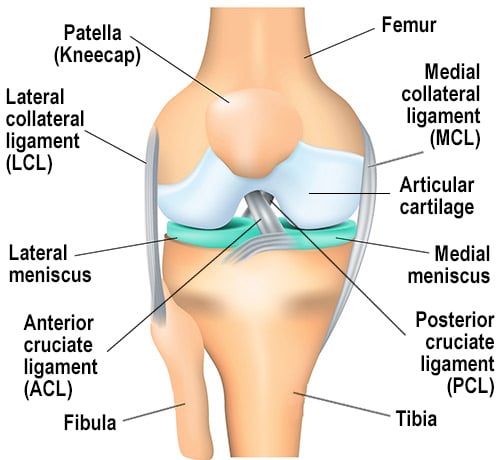 Anatomy of the knee joint. The menisci (highlighted) are crucial for cushioning and stability. Source: HSS.edu
Anatomy of the knee joint. The menisci (highlighted) are crucial for cushioning and stability. Source: HSS.edu
Meniscus Tears
This is the most common cause of true knee locking. The meniscus is a C-shaped piece of tough, fibrocartilaginous tissue that acts as a shock absorber, stabilizer, and load distributor between your shinbone and thighbone. A specific type of injury called a "bucket-handle tear" can cause a large, flap-like piece of the meniscus to detach and flip into the intercondylar notch of the knee, physically blocking movement. This type of tear often results from forceful twisting or pivoting motions common in sports like basketball, soccer, and football. However, degenerative meniscus tears in older adults can also cause locking if fragmented cartilage catches between joint surfaces during flexion and extension. The meniscus has a limited blood supply, concentrated primarily in its outer third (the "red-red" zone). Tears occurring in this vascular region have a higher potential for healing, whereas inner zone ("white-white") tears rely on synovial fluid for nutrition and rarely heal without surgical intervention.
Loose Bodies
Fragments of bone or cartilage can break off due to a traumatic injury, degenerative conditions like osteoarthritis, or a condition known as osteochondritis dissecans (OCD). OCD occurs when a small segment of bone at a joint separates from the surrounding area due to insufficient blood supply. These "loose bodies," sometimes colloquially called "joint mice," can float freely within the joint fluid and synovial cavity. When the knee moves through its full range of motion, these fragments can become temporarily lodged between the articular cartilage of the femur and tibia, causing the joint to lock up suddenly. As the knee changes position, the loose body may dislodge itself, explaining why locking can be intermittent and unpredictable. Over time, untreated loose bodies can cause secondary damage to the articular cartilage, accelerating the development of post-traumatic osteoarthritis.
Ligament Injuries
While less common, a severe injury like a complete tear of the Anterior Cruciate Ligament (ACL) can sometimes cause locking. The torn stump of the ligament can get caught in the joint, creating a mechanical block. Additionally, acute ligamentous injuries are frequently accompanied by hemarthrosis (bleeding into the joint space). The accumulation of blood increases intra-articular pressure, which can severely restrict extension and create a pseudo-locking effect. Chronic ACL deficiency can also lead to altered knee kinematics, where the tibia translates abnormally forward during weight-bearing, causing the posterior horn of the medial meniscus to become impinged and mechanically caught.
Causes of Pseudo Locking
Arthritis
Osteoarthritis, the "wear-and-tear" form of arthritis, is a primary cause of pseudo-locking, especially in older adults. As articular cartilage progressively breaks down, the resulting pain, synovial inflammation, and joint stiffness can trigger prolonged muscle spasms that immobilize the joint. In advanced stages, the formation of osteophytes (bone spurs) and narrowing of the joint space can create a mechanical limitation to extension, which patients often interpret as locking. Additionally, the chronic low-grade inflammation associated with arthritis leads to thickening of the joint capsule (arthrofibrosis), further restricting mobility. Rheumatoid arthritis and other inflammatory arthropathies can similarly cause severe effusions and synovitis that result in pseudo-locking symptoms.
Plica Syndrome
The synovial plica is an embryological remnant of tissue that lines the knee joint. While most plicae remain thin and asymptomatic, certain folds—particularly the medial plica—can become thickened, fibrotic, and highly vascularized due to repetitive trauma, overuse, or direct impact. If this irritated tissue becomes inflamed, it loses its elasticity and can snap over the medial femoral condyle during knee flexion. This snapping creates a painful catching sensation and localized inflammation that often progresses to the feeling of a locked knee. Plica syndrome is frequently misdiagnosed as meniscus pathology, making careful clinical examination crucial.
Patellar Maltracking
This condition occurs when the kneecap (patella) shifts out of its normal anatomical groove (trochlea) as you bend or straighten your leg. The abnormal lateral tracking places excessive compressive forces on the lateral facet of the patella and the lateral femoral trochlea, causing chondromalacia (cartilage softening). The resulting friction, pain, and reactive swelling in the retropatellar space can cause significant pain and a sensation of the knee catching, grinding (crepitus), or getting stuck. Factors contributing to maltracking include quadriceps weakness, tight lateral retinaculum, femoral anteversion, and flat-footed biomechanics (excessive pronation).
Severe Pain and Swelling
Any acute knee injury that causes significant pain and rapid swelling (effusion) can lead to pseudo-locking. The joint capsule has a finite volume capacity. When it fills with synovial fluid or blood, the increased intra-articular pressure stimulates mechanoreceptors that inhibit the quadriceps muscle group, preventing full extension. It is the body's natural defense mechanism to prevent movement and protect the injured joint from further harm. In some cases, Hoffa's fat pad (infrapatellar fat pad) impingement can also mimic locking. This fatty tissue sits behind the patellar tendon and can become pinched and inflamed, causing severe anterior knee pain and extension block during active movement.
When to See a Doctor: Red Flags You Shouldn't Ignore
While some minor instances of knee locking might resolve with gentle movement or a short period of rest, certain symptoms warrant immediate medical attention. Delaying evaluation for specific red flags can lead to irreversible cartilage damage, chronic instability, or permanent loss of function. Contact a doctor, orthopedic specialist, or visit an urgent care facility if you experience:
- Inability to bear any weight on the affected leg: This suggests significant structural damage, such as a fracture, severe ligament rupture, or acute meniscal extrusion.
- Severe or escalating pain and swelling: Rapidly progressive swelling within the first 6 hours of injury often indicates hemarthrosis, which requires professional drainage and evaluation.
- The knee remains locked and cannot be unlocked with gentle motion: Prolonged mechanical locking can lead to secondary joint capsule contractures and cartilage degeneration if the obstruction is not surgically addressed.
- You heard a loud "pop" at the moment of injury: Audible pops are classic signs of ligamentous rupture (especially ACL), meniscal tears, or patellar dislocation.
- Signs of infection, such as fever, chills, profound redness, or localized warmth around the knee: Septic arthritis is a medical emergency that can rapidly destroy joint cartilage within days if untreated with intravenous antibiotics and joint lavage.
- Numbness, tingling, or coldness in the lower leg or foot: These neurovascular symptoms may indicate compromised blood flow or nerve impingement, requiring immediate emergency intervention.
- Recurrent episodes of locking: Even if the knee spontaneously unlocks, repeated episodes indicate an unstable intra-articular lesion that requires definitive treatment to prevent premature osteoarthritis.
Diagnosis: How a Doctor Determines the Cause
To provide the right treatment, your doctor must first pinpoint the exact cause of the locking. A thorough diagnosis typically involves a systematic, multi-modal approach:
- Medical History: Your doctor will ask detailed questions about your symptoms, including the exact mechanism of injury, the frequency and duration of locking episodes, aggravating and alleviating factors, and any previous knee surgeries or injections. They will also assess your activity level, occupation, and overall health status.
- Physical Examination: The clinician will visually assess your knee for swelling, effusion, bruising, and muscle atrophy (particularly of the quadriceps). They will palpate joint lines for focal tenderness and systematically test your range of motion (flexion, extension, and rotation). They will perform specific orthopedic maneuvers:
- McMurray Test: The doctor rotates the tibia while flexing and extending the knee to elicit a painful click or pop, highly suggestive of a meniscal tear.
- Thessaly Test: Standing on the affected leg and rotating the body at 20 degrees of knee flexion; pain or locking indicates meniscal pathology.
- Lachman and Pivot Shift Tests: Assess ACL integrity and rotational stability.
- Patellar Grind/Appliance Tests: Evaluate retropatellar cartilage health and tracking alignment.
- Imaging Tests:
- X-rays: Weight-bearing anteroposterior, lateral, and sunrise views are used first to identify bone-related issues like fractures, osteophytes, joint space narrowing, loose calcified fragments, or signs of advanced arthritis. They provide an excellent baseline but cannot visualize soft tissues.
- MRI (Magnetic Resonance Imaging): An MRI provides high-resolution, cross-sectional images of the knee's soft tissues, making it the gold standard non-invasive tool for diagnosing meniscus tears, ligament damage, articular cartilage defects, bone bruises, and synovial abnormalities. Advanced sequences can even quantify the volume of joint effusion.
- Diagnostic Arthrocentesis (Joint Aspiration): If infection or inflammatory arthritis is suspected, a needle may be used to extract synovial fluid. The fluid is analyzed for cell count, crystals (gout/pseudogout), bacteria, and protein content.
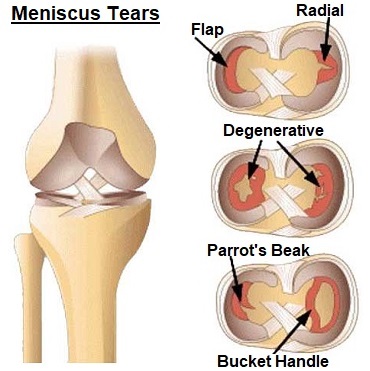 Different types of meniscus tears can cause locking, with the bucket handle tear being a classic example. Source: Knee-Pain-Explained.com
Different types of meniscus tears can cause locking, with the bucket handle tear being a classic example. Source: Knee-Pain-Explained.com
In complex cases, a diagnostic ultrasound may be used dynamically to assess tendon movement, plica snapping, or Baker's cysts in real-time. If imaging remains inconclusive but clinical suspicion for a mechanical block remains high, a diagnostic arthroscopy may be performed to directly visualize the joint interior.
Treatment and Relief for a Locked Knee
Treatment is highly individualized and tailored to the underlying cause, severity, duration of symptoms, patient age, and functional demands. The overarching goal is always to restore pain-free range of motion, stabilize the joint, and prevent long-term degenerative changes.
Immediate At-Home Care: How to Safely Unlock Your Knee
If you experience a locked knee, the most important rule is do not force it. Forcing the joint past a mechanical block or through severe muscle guarding can tear additional cartilage, worsen ligament injuries, or cause micro-fractures. You can try these gentle, evidence-based methods for relief:
- Gentle Movement & Gravity Assistance: Sit down on a stable surface, relax your leg muscles completely, and slowly dangle the leg over the edge. Let gravity gently encourage extension. Slowly and gently try to bend and straighten the knee within a pain-free range. Avoid ballistic or jerking movements. A gentle, sustained hamstring stretch (held for 30 seconds, repeated 3 times) may also help ease posterior tension that restricts full extension.
- Heat and Ice Therapy (Contrast Protocol): Apply a moist heat pack for 15 minutes to increase local blood flow, improve tissue elasticity, and relax the surrounding musculature. If there is acute swelling or recent trauma (within 48 hours), switch to an ice pack or cryotherapy cuff for 15-20 minutes to cause vasoconstriction and reduce inflammatory mediators. Always use a cloth barrier to prevent skin injury.
- The RICE Protocol & Modifications: If the locking is due to an acute injury, follow the modified RICE protocol:
- Rest: Use crutches temporarily to offload weight and avoid activities that provoke pain or instability.
- Ice: Apply cold therapy immediately post-injury and after any rehabilitation exercises.
- Compression: Use a properly fitted elastic bandage or compression sleeve to manage swelling. Ensure it is not so tight that it compromises distal circulation.
- Elevation: Keep the leg raised above the level of the heart to facilitate venous and lymphatic drainage. Prop the heel, not just the knee, to encourage terminal knee extension.
- Over-the-Counter Medication: Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or naproxen can help manage pain and reduce prostaglandin-mediated inflammation. Acetaminophen may be used if NSAIDs are contraindicated. Always consult a pharmacist regarding dosage and interactions.
- Knee Immobilization Bracing: A hinged knee brace or sleeve can provide proprioceptive feedback, limit painful end-range movements, and give the patient a sense of security during the acute phase.
Professional Medical Treatments
If at-home care isn't effective, symptoms persist beyond 1-2 weeks, or true mechanical locking is confirmed, a doctor may recommend one of the following treatments.
Physical Therapy & Rehabilitation
A licensed physical therapist will design a phased rehabilitation program targeting neuromuscular control, joint kinematics, and muscular balance. Initial phases focus on pain modulation, edema control, and restoring passive and active range of motion. As symptoms improve, the program transitions to strengthening the dynamic stabilizers:
- Quadriceps Activation: Straight leg raises, quad sets, and closed-chain exercises like mini-squats and leg presses (avoiding deep flexion initially) to combat arthrogenic muscle inhibition.
- Posterior Chain & Hip Strengthening: Glute bridges, clamshells, and hamstring curls to improve pelvic alignment and reduce valgus stress on the knee.
- Proprioception & Balance: Single-leg stands on unstable surfaces, perturbation training, and gait retraining to restore the nervous system's ability to stabilize the joint dynamically.
- Manual Therapy: Soft tissue mobilization, joint mobilizations (Grades I-III), and patellar mobilizations can break down adhesions, improve synovial fluid circulation, and restore normal tracking.
Medications and Injections
For pseudo-locking driven by synovitis, arthritis, or chronic inflammatory conditions, your doctor may recommend targeted pharmacological interventions. Corticosteroid injections deliver potent anti-inflammatory medication directly into the intra-articular space, often providing rapid relief within 48-72 hours. Hyaluronic acid (viscosupplementation) injections may be used in osteoarthritis to restore synovial fluid viscosity and lubricate joint surfaces. Emerging regenerative medicine therapies, such as Platelet-Rich Plasma (PRP) or bone marrow aspirate concentrate, are increasingly utilized for early-stage degenerative changes and tendinopathy, though clinical guidelines continue to evolve regarding their definitive efficacy for locking symptoms.
Surgical Options
Surgery is typically reserved for cases of true mechanical locking that fail to resolve with 4-6 weeks of conservative treatment, or when structural integrity is severely compromised.
- Arthroscopy: This minimally invasive, outpatient procedure is the gold standard for addressing intra-articular pathology. The surgeon makes 2-3 small portals (incisions) to insert a fiber-optic arthroscope and specialized micro-instruments. They can perform partial meniscectomy (trimming unstable flaps), meniscal repair (suturing tears in vascular zones), loose body extraction, plica resection, or chondroplasty (smoothing frayed cartilage). Recovery typically involves immediate weight-bearing with crutch assistance, with return to daily activities within 2-4 weeks.
- Ligament Reconstruction: For locking secondary to complete ACL tears with instability, arthroscopic reconstruction using autografts (patellar tendon, hamstring, or quadriceps tendon) or allografts is indicated. This is a more extensive surgery requiring 9-12 months of structured rehabilitation before return to pivoting sports.
- Osteotomy: In younger patients with isolated compartment arthritis and malalignment (bow-legged or knock-kneed), a realignment osteotomy shifts weight-bearing forces away from the damaged joint area, delaying the need for replacement.
- Partial or Total Knee Replacement (Arthroplasty): In cases of severe, end-stage osteoarthritis or rheumatoid arthritis where the joint space is obliterated and locking is constant, arthroplasty replaces the damaged articulating surfaces with medical-grade metal and polyethylene components. Modern techniques, including robotic-assisted surgery, have dramatically improved precision, implant longevity (often 15-20+ years), and post-operative recovery times.
Long-Term Management and Preventing Recurrence
Once the immediate issue is resolved, whether through rehabilitation or surgery, the focus shifts to preventing future episodes and optimizing lifelong joint health. A proactive, multi-disciplinary approach yields the best outcomes.
- Consistent Strength & Conditioning: A lifelong commitment to strengthening your quadriceps, hamstrings, glutes, and core is the most effective way to stabilize the knee joint and prevent re-injury. Strong muscles act as dynamic shock absorbers, offloading compressive forces from the articular cartilage. Incorporate low-impact cross-training such as cycling, elliptical training, swimming, and water aerobics to maintain cardiovascular fitness without excessive joint wear.
- Biomechanics & Proper Footwear: Wear supportive, well-cushioned shoes appropriate for your foot type and activity. Consider custom orthotics or over-the-counter arch supports if you have flat feet or excessive pronation, as faulty foot mechanics directly alter tibial rotation and knee tracking.
- Activity Pacing & Ergonomics: Learn to listen to your body's warning signs. Gradually increase training volume and intensity, adhering to the 10% rule per week. Avoid prolonged squatting, kneeling on hard surfaces, and sudden, forceful twisting movements on planted feet. Use proper lifting techniques and consider ergonomic modifications at work or home.
- Weight Management & Nutrition: Every extra pound of body weight adds approximately four pounds of compressive force on your knees during walking, and up to eight times during running or stair climbing. Maintaining a healthy BMI significantly reduces mechanical stress. Adopt an anti-inflammatory diet rich in omega-3 fatty acids (salmon, flaxseeds, walnuts), colorful antioxidants (berries, leafy greens), vitamin D, and adequate lean protein to support tissue repair and cartilage matrix synthesis.
- Chronic Condition Optimization: If arthritis is the underlying driver of pseudo-locking, collaborate with a rheumatologist or primary care physician on a comprehensive management plan. This may include disease-modifying agents for inflammatory arthritis, consistent low-impact exercise, weight optimization, and periodic joint monitoring. Sleep hygiene and stress management are also critical, as poor sleep lowers pain tolerance and chronic stress exacerbates systemic inflammation.
- Regular Follow-Up: Schedule periodic check-ups, especially if you have a history of significant trauma or surgical intervention. Early intervention for new symptoms prevents minor issues from becoming major mechanical derangements.
By understanding the signals your body is sending, respecting the healing timeline, and seeking appropriate care when warranted, you can effectively manage a locked knee and take proactive, evidence-based steps to keep your joints healthy, stable, and mobile for decades to come.
Frequently Asked Questions
How long does it take to recover from a locked knee?
Recovery time varies dramatically depending on the underlying cause and treatment pathway. Pseudo-locking caused by mild muscle spasms, minor strains, or early-stage inflammation often resolves within 1 to 3 weeks with conservative RICE therapy, NSAIDs, and gentle physical therapy. True mechanical locking caused by a displaced meniscus tear or loose body typically requires surgical intervention (arthroscopy) if it does not resolve within 2-4 weeks. Post-arthroscopic recovery allows for immediate weight-bearing and a return to sedentary work within days, with full return to sports and high-impact activities usually taking 6 to 12 weeks. Severe ligament reconstructions or joint replacements require 3 to 9 months of structured rehabilitation for optimal functional recovery.
Can a locked knee fix itself without surgery?
Yes, in many cases. Pseudo-locking frequently resolves on its own or with conservative treatment as inflammation decreases and muscle guarding subsides. Even some meniscus tears can heal spontaneously if they are located in the outer, well-vascularized "red zone," or if the displaced fragment naturally shifts back into place and scars over. However, true mechanical locking caused by a large bucket-handle tear, unstable loose bodies, or significant ligament disruption rarely resolves permanently without medical intervention. Repeated forced manipulation or ignoring persistent locking can accelerate cartilage wear and lead to chronic instability.
What is the difference between knee locking and knee popping?
Knee locking and popping are distinct mechanical symptoms, though they can coexist. Knee popping (crepitus) refers to an audible or palpable sound/cracking sensation that occurs during movement. It is often harmless, caused by nitrogen gas bubbles releasing from synovial fluid or tendons snapping over bony prominences. However, painful popping with swelling can indicate cartilage damage or patellar maltracking. Knee locking, conversely, refers to a physical restriction of movement where the joint cannot fully extend or flex. It implies a mechanical block (true locking) or severe neurological inhibition due to pain/swelling (pseudo-locking). While popping is often benign, true locking is a clinical red flag requiring professional evaluation.
Are knee braces effective for preventing knee locking?
Braces can be highly effective as an adjunct therapy, but they do not cure the underlying pathology. For pseudo-locking related to patellar maltracking or mild instability, a patellar-tracking brace or hinged sleeve can improve proprioception, guide the kneecap into a healthier trajectory, and provide psychological confidence. For post-injury recovery, unloader braces shift weight away from damaged compartments, reducing mechanical stress. However, braces should not replace targeted physical therapy. Over-reliance on external support can lead to muscular atrophy. The most effective "bracing" is building robust intrinsic musculature through dedicated rehabilitation.
When should I apply heat versus ice for a locked knee?
The choice depends on the injury phase and symptom profile. Apply ice (cryotherapy) during the acute phase (first 48-72 hours post-injury) or immediately after activity if swelling, throbbing, or sharp inflammatory pain is present. Ice causes vasoconstriction, reduces metabolic rate, and numbs pain receptors. Apply heat (thermotherapy) for chronic stiffness, pseudo-locking driven by muscle spasms, or subacute pain without active swelling. Heat promotes vasodilation, increases tissue elasticity, and relaxes hyperactive guarding muscles. A common clinical recommendation is contrast therapy: alternating 3 minutes of heat with 1 minute of cold to create a "pumping" effect that accelerates fluid clearance and nutrient delivery, finishing with ice if inflammation is prominent.
Conclusion
Experiencing a locked knee is a distressing and functionally limiting symptom that should never be dismissed as a minor inconvenience. By distinguishing between true mechanical obstruction and pain-induced pseudo-locking, patients and clinicians can navigate toward the most appropriate diagnostic and therapeutic pathways. While some cases resolve with targeted rest, anti-inflammatory measures, and dedicated physical therapy, persistent mechanical blocks often require timely orthopedic intervention to prevent irreversible cartilage damage and long-term mobility loss.
Empowerment comes from knowledge: recognizing red flags, understanding the anatomy at play, and adhering to evidence-based rehabilitation protocols can dramatically improve outcomes. Whether through conservative management, minimally invasive arthroscopy, or joint preservation strategies, modern orthopedics offers robust solutions for restoring full, pain-free knee function. Prioritize proactive joint health through consistent strengthening, mindful movement patterns, and appropriate medical consultation. With the right approach, a locked knee is not a permanent sentence to limited mobility, but rather a clear signal to realign your movement habits and invest in the long-term resilience of your lower extremities.
References
- Medical News Today. (2019). Locked knee: Causes, symptoms, and treatment. Link
- OrthoNeuro. (n.d.). 7 Main Causes of Locked Knees. Link
- Ronak Mukesh Patel MD. (2024). Knee Popping, Locking, Buckling, and Giving Out. Link
- Hospital for Special Surgery (HSS). (2024). Meniscus Tear: Symptoms & Treatment. Link
- WebMD. (n.d.). Knee Osteoarthritis. Link

About the author
Samuel Jones, MD, is a board-certified orthopedic surgeon specializing in joint replacement and orthopedic trauma. He is a team physician for a professional sports team and practices at a renowned orthopedic institute in Georgia.