A Comprehensive Guide to Understanding Your Headache Map

Key points
- Location: Bilateral (both sides), often felt across the forehead, on the temples, or at the back of the head and neck.
- Symptoms: A mild-to-moderate, non-throbbing pain. It's often described as a "hatband" sensation.
- Common Causes: Stress, muscle tension in the neck and shoulders, poor posture, and fatigue are primary triggers.
A throbbing pain behind your eye, a dull ache that wraps around your head like a tight band, or a sharp pressure in your sinuses—headaches are a near-universal experience, but their variety can be baffling. One of the most intuitive tools for making sense of this pain is the "headache map," a concept that links the location of your discomfort to its potential cause. Globally, headache disorders rank among the most common neurological conditions, affecting billions of individuals across all demographics and significantly impacting daily productivity, mental health, and overall quality of life. Despite their prevalence, many people struggle to differentiate between benign, self-limiting headaches and those requiring clinical intervention. The headache map serves as a foundational educational framework, helping patients and clinicians alike visualize how pain referral patterns correlate with underlying neurological, vascular, and musculoskeletal mechanisms.
The economic and psychosocial burden of headache disorders cannot be overstated. Migraine alone is consistently ranked among the top ten leading causes of years lived with disability worldwide, according to comprehensive global burden of disease studies. Chronic daily headaches contribute to substantial workplace absenteeism, presenteeism (reduced productivity while at work), and frequent emergency department visits, often resulting in millions of healthcare dollars spent annually. Beyond the financial impact, the psychological toll includes increased rates of anxiety, depression, sleep disturbances, and social isolation. Patients frequently report feeling dismissed or misunderstood, which is why structured educational tools like headache maps are increasingly integrated into primary care and neurology clinics. These visual frameworks not only validate patient experiences but also accelerate the clinical workflow by providing a shared language for symptom description. By demystifying headache anatomy and pathophysiology, healthcare providers can foster stronger therapeutic alliances and guide patients toward targeted, evidence-based interventions earlier in the disease course.
While a headache map can be an invaluable starting point for understanding your body's signals, it's essential to remember that location is just one piece of a complex puzzle. Headache pathophysiology involves intricate interactions between cranial blood vessels, peripheral nerves, central nervous system processing, and systemic physiological triggers. This comprehensive guide will help you navigate your own headache map, understand what other symptoms to watch for, explore evidence-based management strategies, and know exactly when it's time to seek professional medical advice. Understanding the multidimensional nature of head pain requires looking beyond simple geography. Factors such as circadian rhythm disruption, hormonal fluctuations, genetic predisposition, medication history, and even gut-brain axis modulation play critical roles in headache genesis and chronification. A truly effective approach to headache management combines anatomical awareness with lifestyle optimization, targeted pharmacotherapy, and, when necessary, advanced neurological interventions.
What is a Headache Map?
A headache map is a diagnostic tool, often presented as an infographic, that illustrates the common locations of pain for different types of headaches. By identifying where your head hurts, you can narrow down the potential type of headache you're experiencing, which is the first step toward finding effective relief. These maps are grounded in the International Classification of Headache Disorders (ICHD-3), the globally recognized diagnostic standard developed by the International Headache Society. The ICHD-3 categorizes headaches into primary disorders (where the headache itself is the disease, like migraines or tension-type headaches) and secondary disorders (where the headache is a symptom of another underlying condition, such as infection, trauma, or vascular abnormalities).
The clinical utility of headache mapping extends far beyond patient education. In neurology practice, pain referral patterns are deeply tied to the neuroanatomical architecture of the trigeminocervical complex. The trigeminal nerve, responsible for sensation in the face and anterior scalp, converges with upper cervical nerve roots (C1–C3) at the brainstem. This anatomical convergence means that irritation in the cervical spine can be perceived as frontal, temporal, or retro-orbital pain—a phenomenon known as referred pain. Headache maps visualize these referral pathways, helping clinicians distinguish between true primary headache phenotypes and secondary pain generators. For example, occipital neuralgia or cervicogenic dysfunction frequently masquerades as migraine due to shared neural circuitry, but careful mapping of radiation patterns, palpation of trigger points, and response to cervical movement can clarify the diagnosis. Furthermore, digital health platforms have revolutionized headache mapping by enabling real-time symptom logging, geolocation-based weather tracking, and AI-assisted pattern recognition, allowing for highly personalized treatment algorithms.
For example, pain localized to the sinus areas might suggest a sinus headache, while one-sided, throbbing pain is a classic sign of a migraine. This visual approach helps both patients and doctors begin a more targeted conversation about symptoms. In clinical practice, headache maps are frequently integrated into digital pain-tracking applications, patient education pamphlets, and neurological intake forms. They empower individuals to communicate more effectively during medical appointments by providing precise anatomical descriptors rather than vague statements like "my head hurts." Understanding the neuroanatomical basis of referred pain—such as how trigeminal nerve branches innervate different facial and cranial regions—further clarifies why certain headaches manifest in predictable patterns. Additionally, mapping headache distribution over time can reveal evolution from episodic to chronic states, prompt early intervention, and help avoid inappropriate imaging or unnecessary surgical consultations. When combined with a thorough clinical history, headache maps significantly improve diagnostic accuracy and streamline the pathway to effective therapy.
Decoding Your Headache: A Location-Based Guide
Let's explore the different regions on the headache map and what they might signify.
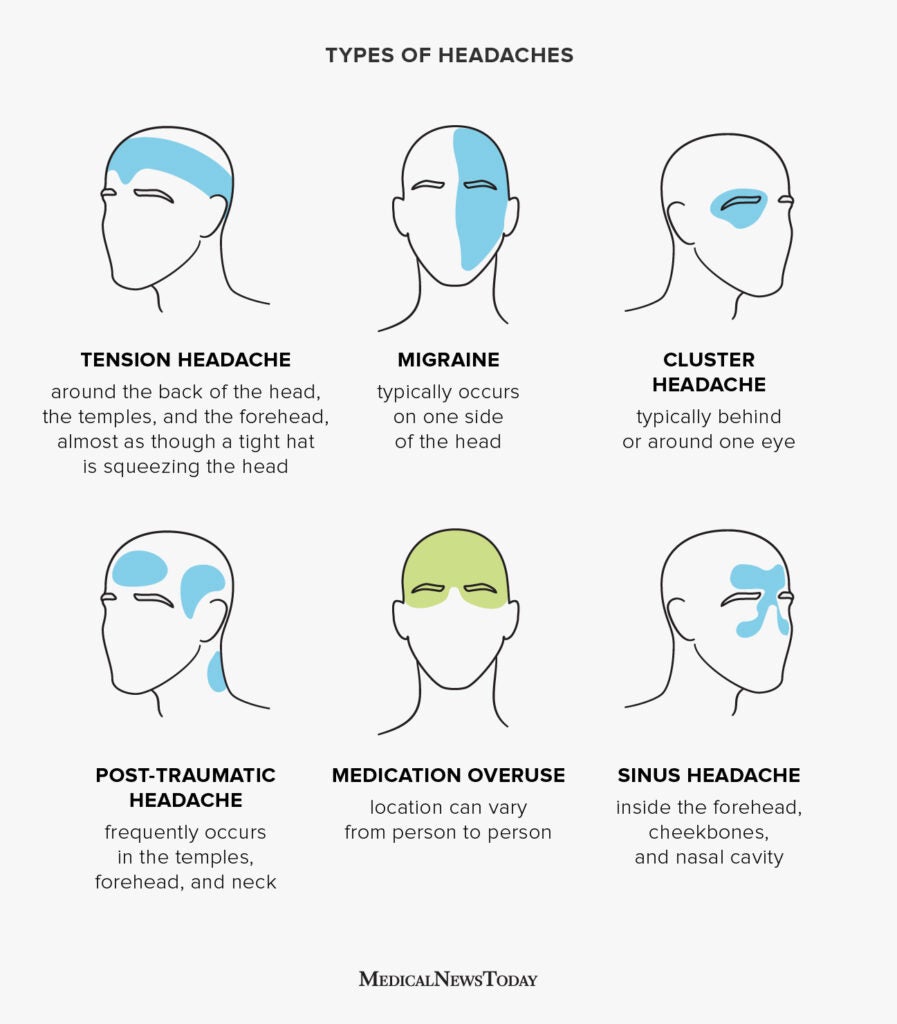 Image Source: MedicalNewsToday
Image Source: MedicalNewsToday
Pain All Over or Like a Tight Band
If your headache feels like a constant, dull ache or a pressure band squeezing your entire head, you are likely experiencing a Tension-Type Headache.
- Location: Bilateral (both sides), often felt across the forehead, on the temples, or at the back of the head and neck.
- Symptoms: A mild-to-moderate, non-throbbing pain. It's often described as a "hatband" sensation.
- Common Causes: Stress, muscle tension in the neck and shoulders, poor posture, and fatigue are primary triggers.
Tension-type headaches (TTH) are the most prevalent headache disorder worldwide, affecting an estimated 70% of the general population at some point in their lives. Unlike migraines, TTH does not typically involve significant nausea, vomiting, or photophobia, though mild light or sound sensitivity may occur. The exact mechanism remains debated, but current research points toward peripheral myofascial sensitization and altered central pain processing. Chronic pericranial muscle tenderness, often resulting from sustained contraction due to psychological stress or ergonomic strain, plays a substantial role in episodic cases. Over time, repeated episodes can lead to central sensitization, where the nervous system becomes hyperreactive, transitioning episodic TTH into chronic TTH (defined as occurring on 15 or more days per month). Emerging neuroimaging studies have also identified subtle gray matter changes in pain-modulating regions of the brainstem and thalamus in patients with chronic TTH, suggesting that long-standing peripheral irritation can induce neuroplastic alterations that perpetuate pain cycles independently of the original trigger.
Management typically begins with conservative, non-pharmacological interventions. Regular aerobic exercise, progressive muscle relaxation techniques, cognitive behavioral therapy (CBT), and targeted physical therapy for cervical and pericranial muscle dysfunction have demonstrated strong efficacy. Ergonomic assessments are crucial for individuals with desk-based occupations; adjusting chair lumbar support, elevating computer monitors to eye level, and implementing structured microbreaks (following the 20-20-20 rule: every 20 minutes, look 20 feet away for 20 seconds, and stretch) can dramatically reduce muscular strain. For acute relief, over-the-counter analgesics such as acetaminophen, ibuprofen, or naproxen are generally effective when used judiciously. However, patients must be cautious about medication-overuse headache (MOH), a rebound condition caused by taking acute headache medications more than 15 days per month for over three months. Preventive pharmacotherapy, including low-dose amitriptyline, may be considered for individuals experiencing frequent or disabling episodes. Additionally, emerging modalities like dry needling, trigger point injections with local anesthetics, and transcutaneous electrical nerve stimulation (TENS) are gaining traction for refractory cases, offering non-systemic alternatives that directly address myofascial trigger zones.
Throbbing Pain on One Side of the Head
Unilateral, pulsating pain is the most defining characteristic of a Migraine.
- Location: Typically on one side of the head, but it can affect both.
- Symptoms: Moderate-to-severe throbbing pain that can last for hours or even days. It's often accompanied by nausea, vomiting, and extreme sensitivity to light and sound. Some people also experience an "aura"—visual disturbances like flashing lights or blind spots—before the headache begins.
- Common Causes: Migraines have a strong genetic component and can be triggered by hormonal changes, stress, certain foods, and changes in sleep patterns.
Migraine is not merely a severe headache; it is a complex neurovascular disorder characterized by episodes of recurrent, often disabling pain. The underlying pathophysiology involves abnormal brain activity affecting nerve signals, chemicals, and blood vessels. Cortical spreading depression—a wave of neuronal depolarization followed by suppressed brain activity—is believed to initiate migraine aura and activate the trigeminovascular system, leading to the release of calcitonin gene-related peptide (CGRP) and subsequent inflammation of meningeal blood vessels. This cascade explains the throbbing quality, autonomic symptoms, and profound sensitivity experienced during attacks. Genetic studies have identified over 40 susceptibility loci associated with migraine, highlighting the strong hereditary component and the involvement of ion channels, vascular regulation pathways, and glutamate signaling. Functional MRI research during migraine attacks reveals altered connectivity in the default mode network and brainstem nuclei, underscoring that migraine is fundamentally a disorder of sensory processing and central nervous system hypersensitivity.
Migraines affect roughly 12% of the global population, with women being three times more likely to experience them than men, largely due to estrogen fluctuations. Triggers are highly individualized and can include barometric pressure changes, missed meals, alcohol, bright lights, and intense physical exertion. The prodrome phase, occurring hours or days before pain onset, may feature mood changes, food cravings, neck stiffness, or frequent yawning. The postdrome phase, often called a "migraine hangover," can leave individuals feeling fatigued, cognitively foggy, or unusually refreshed for up to 48 hours after pain subsides. Understanding these temporal phases allows patients to implement early-stage interventions, such as hydration, magnesium supplementation, or taking acute medications during the prodrome before central sensitization fully develops. Menstrual migraines, specifically tied to the rapid drop in estrogen preceding menstruation, often respond well to targeted short-term prophylaxis like frovatriptan or NSAID regimens initiated two days prior to expected onset.
Acute migraine treatment has evolved significantly beyond traditional analgesics. Triptans, which act as serotonin (5-HT1B/1D) agonists to constrict blood vessels and inhibit pain pathways, remain first-line for moderate-to-severe attacks. Newer therapeutics, including gepants (CGRP receptor antagonists) and ditans (5-HT1F receptor agonists), offer alternatives for patients who cannot tolerate triptans due to cardiovascular contraindications. For individuals with four or more migraine days per month, preventive treatments such as beta-blockers, anticonvulsants, antidepressants, CGRP monoclonal antibodies, and onabotulinumtoxinA injections for chronic migraine are available. Lifestyle consistency—maintaining regular sleep schedules, hydration, and stress management—remains the cornerstone of migraine prevention. Additionally, neuromodulation devices like external trigeminal nerve stimulation (eTNS) and single-pulse transcranial magnetic stimulation (sTMS) provide FDA-cleared, non-invasive options that modulate cortical excitability without systemic drug exposure, making them ideal for patients seeking drug-free management or those with polypharmacy concerns.
Piercing Pain Around or Behind One Eye
Excruciating, sharp pain localized to one eye is the hallmark of a Cluster Headache.
- Location: Centered around or behind one eye, but the pain can radiate to the forehead, temple, and cheek on the same side.
- Symptoms: The pain is severe, often described as a burning or piercing sensation. Attacks occur in "clusters," meaning they can happen daily for weeks or months. Accompanying symptoms on the affected side include a red or watery eye, a drooping eyelid, and a runny or stuffy nostril.
- Common Causes: The exact cause is unknown, but it's linked to the hypothalamus in the brain. Alcohol can trigger an attack during a cluster period.
Cluster headache is widely recognized as one of the most painful conditions known to medicine, earning the nickname "suicide headache" in historical medical literature. It belongs to the trigeminal autonomic cephalalgias (TACs), a group of primary headache disorders characterized by unilateral head pain with ipsilateral cranial autonomic symptoms. The condition shows a striking male predominance (roughly 3:1 to 4:1) and typically onsets between ages 20 and 40. The pain peaks rapidly, usually within 5 to 10 minutes, and lasts 15 to 180 minutes if untreated. Attacks often occur at highly predictable times, frequently waking patients from REM sleep, which reinforces the strong association with hypothalamic circadian rhythm dysregulation. Positron emission tomography (PET) scans during active cluster periods consistently show heightened metabolic activity in the posterior hypothalamus, suggesting a pacemaker-like dysfunction that synchronizes with the autonomic nervous system to generate cyclical pain episodes.
Cluster periods typically last 6 to 12 weeks, followed by remission periods that can span months or even years. During an active cluster cycle, absolute abstinence from alcohol is mandatory, as even minimal consumption reliably triggers attacks. Smoking is also highly prevalent among cluster headache sufferers, though cessation does not always terminate the cycle. Behavioral modifications are critical during active periods; maintaining strict sleep regularity, avoiding high-altitude travel, and steering clear of strong olfactory triggers like solvents or perfumes can help minimize attack frequency. Patients often experience profound anticipatory anxiety as their predictable attack time approaches, which can exacerbate pain perception and prolong recovery. Psychological support, including counseling or participation in specialized headache support networks, plays a vital role in mitigating the severe emotional toll these cycles exact.
Acute treatment requires rapid-acting interventions. High-flow oxygen therapy (12–15 liters per minute via non-rebreather mask) administered for 15 minutes is highly effective for approximately 70% of patients and carries no systemic side effects. Subcutaneous sumatriptan or intranasal triptans provide fast relief when oxygen is unavailable or impractical. Preventive therapy must be initiated immediately upon cycle onset. Verapamil is the first-line prophylactic medication, though it requires ECG monitoring due to potential cardiac conduction effects. Other options include lithium, corticosteroids for bridge therapy, and neuromodulation devices. Because of the severity and suicide risk associated with untreated cluster cycles, prompt neurological evaluation is essential. Emerging treatments like galcanezumab (a CGRP monoclonal antibody) have received regulatory approval specifically for episodic cluster headache prevention, marking a significant advancement in targeted immunotherapy for this historically difficult-to-treat condition. In highly refractory cases, surgical interventions such as occipital nerve stimulation or sphenopalatine ganglion stimulation may be considered by specialized headache centers.
Pressure in the Face, Forehead, or Cheeks
If your headache is accompanied by pressure and tenderness in your face, it may be a Sinus Headache.
- Location: Pain is focused over the sinus cavities—in the forehead, around the eyes, and over the cheeks.
- Symptoms: A deep, constant ache that worsens with sudden head movement or bending forward. It's almost always accompanied by other sinus symptoms, such as nasal congestion, thick nasal discharge, and sometimes a fever. Many migraines are misdiagnosed as sinus headaches.
True sinus headaches, clinically termed rhinosinusitis-related headaches, occur secondary to inflammation or infection of the paranasal sinuses. The maxillary, frontal, ethmoid, and sphenoid sinuses are lined with mucous membranes that become swollen and congested during upper respiratory infections, allergic rhinitis, or nasal polyps. When sinus ostia become obstructed, trapped secretions increase intrasinus pressure, stimulating pain-sensitive nerve endings. The pain is characteristically positional, intensifying when leaning forward due to increased hydrostatic pressure in the inflamed cavities. Unlike migraines, true rhinosinusitis headaches are accompanied by objective clinical signs of mucosal disease, including purulent nasal discharge, hyposmia, and endoscopic evidence of middle meatus inflammation or polypoid edema.
Diagnosis requires clinical evidence of acute or chronic rhinosinusitis: purulent nasal discharge, nasal obstruction, facial pain/pressure/fullness, and reduced sense of smell, often corroborated by endoscopic examination or CT imaging showing mucosal thickening or air-fluid levels. It is crucial to differentiate true sinus headaches from migraines, which frequently present with periorbital pain, autonomic tearing, nasal congestion, and positional worsening. Studies indicate that up to 90% of patients self-diagnosing with "sinus headaches" actually meet ICHD-3 criteria for migraine. This widespread misclassification often leads to inappropriate antibiotic prescribing and delayed initiation of effective migraine therapies. Clinicians should maintain a high index of suspicion for migraine in patients presenting with recurrent "sinus" symptoms that fail to respond to standard decongestants or antibiotics, especially when accompanied by photophobia, phonophobia, or a family history of migraine.
Management depends on etiology. Viral rhinosinusitis is self-limiting and managed with saline irrigation, intranasal corticosteroids, hydration, and decongestants for short-term relief. Bacterial sinus infections, characterized by symptoms lasting >10 days without improvement, severe onset with high fever (>102°F/39°C) and purulent discharge, or "double-worsening" after initial improvement, may require targeted antibiotic therapy (e.g., amoxicillin-clavulanate). Chronic sinusitis with or without nasal polyps often necessitates long-term topical steroids, allergy management, or endoscopic sinus surgery. Treating underlying migraine or allergic triggers frequently resolves perceived sinus headaches entirely. For recurrent allergic contributors, immunotherapy (subcutaneous or sublingual allergen desensitization) offers long-term disease modification by reprogramming immune responses, potentially eliminating chronic mucosal inflammation and associated craniofacial discomfort.
Pain at the Back of the Head or Neck
Pain that starts in the neck and radiates to the back of the head often points to a Cervicogenic Headache.
- Location: Typically starts at the base of the skull and spreads upwards.
- Symptoms: A non-throbbing ache often accompanied by a stiff neck or reduced range of motion. The pain can be triggered by certain neck movements.
- Common Causes: This is a secondary headache caused by an underlying issue in the cervical spine (neck), such as arthritis or an injury.
Cervicogenic headache arises from musculoskeletal or degenerative disorders in the cervical spine, particularly the upper cervical segments (C1–C3). The trigeminocervical nucleus, located in the upper spinal cord and brainstem, receives sensory input from both the trigeminal nerve and the upper cervical nerves. Dysfunction or irritation in the cervical facet joints, intervertebral discs, ligaments, or muscles can refer pain to the occipital, frontal, or temporal regions due to this neural convergence. It is frequently misdiagnosed as tension-type headache or migraine. Postural abnormalities such as forward head posture, commonly seen in individuals who spend prolonged hours on smartphones or computers, increase the mechanical load on the suboccipital muscles by up to 10 pounds for every inch the head translates anteriorly. This sustained biomechanical stress leads to ischemia, metabolic waste accumulation, and trigger point formation in the upper trapezius, levator scapulae, and suboccipital muscle groups.
Key diagnostic features include unilateral headache without side shift, precipitation by specific neck movements or sustained awkward postures, reduced cervical range of motion, and ipsilateral neck, shoulder, or arm pain. Imaging such as X-rays, MRI, or CT scans may reveal osteoarthritis, disc herniation, facet joint degeneration, or post-traumatic changes, though clinical examination and diagnostic nerve blocks remain the gold standard for confirmation. A positive response to a fluoroscopically guided medial branch block or third occipital nerve block strongly confirms the cervical spine as the primary pain generator. Differential diagnosis must carefully exclude vertebrobasilar insufficiency, cervical radiculopathy, and spinal cord pathology, which can present with overlapping neck and occipital pain but require entirely different management pathways.
Treatment is fundamentally rehabilitative. Physical therapy focusing on cervical stabilization, posture correction, scapulothoracic strengthening, and myofascial release techniques yields significant long-term improvement. Ergonomic modifications at workstations—adjusting monitor height, using supportive chairs, and taking frequent microbreaks—are essential for sustained relief. Pharmacological options include NSAIDs, muscle relaxants, or neuropathic pain agents if nerve compression is present. Interventional procedures such as medial branch blocks, facet joint injections, or radiofrequency ablation of the third occipital nerve can provide durable relief for refractory cases. Additionally, targeted exercises like chin tucks, deep cervical flexor training, and thoracic extension mobilizations have demonstrated robust evidence in restoring normal cervicothoracic biomechanics and reducing headache frequency. Patients are encouraged to avoid prolonged static positions, use ergonomic pillows designed to maintain neutral cervical alignment during sleep, and incorporate yoga or Pilates to enhance core and postural muscle endurance.
Beyond Location: Other Crucial Clues
While the headache map is a useful guide, a full picture requires looking at other characteristics of your pain. To truly understand your headache, consider these factors:
The Character of the Pain
How does the pain feel? Describing its quality can provide vital clues.
- Dull and Pressing: Suggests a tension headache.
- Throbbing and Pulsating: A classic sign of a migraine.
- Sharp and Piercing: Characteristic of a cluster headache.
Pain character reflects underlying physiological mechanisms. Dull, pressing pain typically correlates with sustained muscle contraction or mild vascular changes without significant inflammatory mediator release. Throbbing quality mirrors cardiac pulsations and indicates active vasodilation with inflammatory neuropeptide involvement. Sharp, stabbing, or electric-like sensations often suggest neural irritation, neuropathic involvement, or severe focal inflammation. Keeping track of pain descriptors over multiple episodes helps clinicians distinguish primary headache disorders from secondary pathologies and guides therapeutic selection. Beyond these classic descriptors, patients may report burning, aching, squeezing, or pressure-like qualities, each mapping to distinct pathophysiological pathways. For instance, a heavy, pressure-like sensation worsening with Valsalva maneuvers may indicate intracranial hypertension, while a sudden, lightning-like jolt radiating from the neck to the scalp suggests occipital neuralgia. Quantitative sensory testing in specialized headache clinics can objectively measure pain thresholds and help tailor neuromodulatory or pharmacological treatments based on individual pain processing phenotypes.
Identifying Your Triggers
Keeping a headache diary can help you pinpoint what sets off your pain. Common triggers include stress, lack of sleep, and dehydration. For migraines specifically, certain dietary factors, sometimes called the "5 C's," are known triggers for some people:
- Cheese (aged varieties like blue cheese or parmesan)
- Chocolate
- Coffee (or caffeine withdrawal)
- Cola beverages
- Citrus fruits
Trigger identification requires systematic documentation. Effective headache diaries record sleep duration and quality, meal timing and composition, hydration status, weather changes, menstrual cycle phase, stress levels, medication intake, and headache onset/duration/severity. Over 4 to 12 weeks, patterns typically emerge. Beyond the 5 C's, common dietary triggers include monosodium glutamate (MSG), nitrates/nitrites in processed meats, artificial sweeteners (particularly aspartame), sulfites in wine/dried fruits, and tyramine-rich foods. Fasting or skipping meals rapidly drops blood glucose, which can lower the threshold for cortical spreading depression in susceptible individuals. Caffeine demonstrates a complex biphasic effect: low-to-moderate doses can enhance analgesic efficacy and provide acute relief, while daily consumption >300 mg or abrupt cessation frequently precipitates withdrawal headaches. Gradual reduction and strategic, limited use are recommended. Environmental triggers are equally impactful; fluorescent lighting, strong perfumes, high-altitude travel, and rapid barometric pressure drops during storm fronts are frequently reported. Modern smartphone applications leverage machine learning algorithms to cross-reference diary entries with local weather APIs, sleep tracking data, and menstrual cycle logs, providing highly personalized predictive alerts and preventive recommendations.
Accompanying Symptoms
What else are you experiencing?
- Nausea and light sensitivity strongly point toward a migraine.
- A stuffy nose and fever suggest a sinus infection.
- A watery eye and drooping eyelid on one side are telltale signs of a cluster headache.
Autonomic and systemic symptoms are critical diagnostic discriminators. Gastrointestinal stasis is a well-documented feature of migraine, delaying gastric emptying and reducing oral medication absorption—this is why rapidly dissolving, nasal, or injectable formulations are often preferred. Phonophobia, osmophobia (sensitivity to smells), and cutaneous allodynia (pain from normally non-painful stimuli like brushing hair) frequently accompany moderate-to-severe migraines and indicate central sensitization. Allodynia is particularly prognostic; patients who develop widespread cutaneous sensitivity during attacks have higher rates of headache chronification and often require earlier initiation of preventive therapies.
Autonomic symptoms such as lacrimation, conjunctival injection, nasal congestion, rhinorrhea, forehead/facial sweating, or miosis/ptosis localize to trigeminal autonomic reflex pathways. Bilateral autonomic symptoms with fever, malaise, and thick nasal discharge point toward infectious or inflammatory etiologies. Neurological symptoms like hemiparesis, dysphasia, vertigo, or transient cortical blindness warrant immediate evaluation to rule out stroke, transient ischemic attack, or complex migraine variants. Brainstem aura symptoms, including diplopia, dysarthria, tinnitus, or ataxia, characterize basilar-type migraine (now termed migraine with brainstem aura) and require careful differentiation from posterior circulation ischemia. Vestibular migraine, presenting with spontaneous vertigo, motion sensitivity, and balance disturbances alongside headache, often responds to prophylactic vestibular rehabilitation and dietary sodium restriction, highlighting the multidimensional sensory involvement in certain migraine phenotypes.
 Image Source: Healthline
Image Source: Healthline
The Limitations of a Headache Map: A Word of Caution
Headache maps are powerful for starting a conversation, but they are not a substitute for a professional diagnosis. Here's why you should use them with caution:
- Symptom Overlap: Pain location can be misleading. For example, a study from the National Headache Foundation notes that most self-diagnosed sinus headaches are actually migraines.
- Focus on Migraine: Many diagnostic tools are designed primarily to screen for migraines, which means they may not accurately capture the nuances of other headache types like tension-type or cervicogenic headaches.
- Diagnosis is Complex: A doctor's diagnosis relies on a detailed patient history, physical examination, and understanding of the individual's overall health—factors a simple map cannot convey.
Headache diagnosis remains fundamentally clinical. The ICHD-3 criteria require specific combinations of pain characteristics, duration, frequency, associated symptoms, and exclusion of secondary causes. Pain location alone has low specificity because multiple headache types can refer to overlapping anatomical regions. For instance, both migraines and cervicogenic headaches frequently present with unilateral temporal or retro-orbital pain. Furthermore, headache patterns evolve over time; episodic conditions may transform into chronic forms, and multiple primary headache disorders frequently coexist in the same patient (comorbidity). This phenotypic plasticity means that a static map cannot capture the dynamic nature of headache disorders, which are influenced by hormonal shifts, medication changes, stress trajectories, and neuroplastic adaptations.
Secondary headaches caused by intracranial hypertension, space-occupying lesions, giant cell arteritis, carotid dissection, or medication toxicity may initially mimic benign patterns. A headache map cannot assess pupillary reflexes, temporal artery tenderness, papilledema, or focal neurological deficits—findings that fundamentally alter clinical pathways. Relying solely on anatomical location may delay appropriate imaging (MRI/MRV/CT), laboratory testing, or specialist referral. Always integrate location data with comprehensive symptom tracking and professional medical evaluation. Primary care physicians and neurologists utilize a layered diagnostic approach: initial clinical screening, targeted physical and neurological examinations, selective laboratory investigations (e.g., inflammatory markers for suspected arteritis, thyroid function, metabolic panels), and imaging when red flags or atypical features are present. This multidimensional strategy ensures that dangerous secondary pathologies are excluded while optimizing the management of common primary headache disorders.
When to See a Doctor: Recognizing the "Red Flags"
Most headaches are benign, but some can be a sign of a serious underlying condition. You should seek immediate medical attention if your headache is accompanied by any of the following red flags, sometimes remembered by the mnemonic SNNOOP10:
- Systemic Symptoms (fever, stiff neck, rash).
- Neoplasm History (a new headache in someone with a history of cancer).
- Neurological Deficit (weakness, vision loss, confusion, seizures, difficulty speaking).
- Onset is sudden or abrupt (a "thunderclap" headache that peaks within a minute).
- Older Age (new onset of a headache over age 50).
- Pattern Change (a change in frequency, severity, or characteristics of your usual headaches).
- Positional (headache worsens when standing up).
- Precipitated by exertion (triggered by coughing, sneezing, or exercise).
- Papilledema (swelling of the optic nerve, detected during an eye exam).
- Progressive (a headache that steadily worsens over time).
These red flags serve as clinical warning signs that warrant urgent diagnostic workup. Thunderclap headaches may indicate subarachnoid hemorrhage, reversible cerebral vasoconstriction syndrome, or pituitary apoplexy. Positional headaches that worsen upright suggest spontaneous intracranial hypotension (often from CSF leak), while those worsening supine may indicate elevated intracranial pressure. New-onset headaches in patients over 50 raise suspicion for giant cell arteritis, which requires immediate high-dose corticosteroids to prevent irreversible vision loss. Exertional or Valsalva-induced headaches may point to structural abnormalities like Chiari malformation or posterior fossa lesions. Additionally, headaches accompanied by unexplained weight loss, night sweats, or jaw claudication necessitate prompt evaluation for systemic inflammatory or neoplastic processes. Delaying assessment in the presence of these indicators can result in permanent neurological injury, making timely triage essential.
Diagnostic evaluation typically includes neuroimaging (MRI preferred for soft tissue and vascular resolution, CT for acute hemorrhage), blood work (ESR, CRP for arteritis), and sometimes lumbar puncture to assess opening pressure or rule out infection/meningitis. Never dismiss abrupt, severe, or atypical head pain as "just stress" without ruling out life-threatening etiologies. Emergency departments utilize standardized headache pathways to rapidly stratify risk, ensuring that patients with high suspicion for secondary headaches receive expedited imaging and specialist consultation, while those with reassuring primary headache features are safely discharged with clear follow-up instructions. This risk-stratified approach maximizes resource utilization and patient safety.
Special Consideration: Headaches in Pregnancy
Headaches are common during pregnancy due to hormonal shifts, dehydration, and the physical strain of carrying extra weight. While most are tension headaches, it's crucial to discuss any new or severe headaches with your doctor, as they can sometimes be a sign of conditions like preeclampsia. First-trimester headaches often correlate with surging progesterone and estrogen levels, while third-trimester headaches may relate to hemodynamic changes or sleep disruption. Many standard acute and preventive medications are contraindicated or require dose adjustment during gestation and lactation. Acetaminophen remains the preferred first-line acute treatment, while certain antihistamines, magnesium supplementation, and physical therapy are considered safe. New-onset headaches after 20 weeks gestation, particularly when accompanied by hypertension, proteinuria, visual disturbances, right upper quadrant pain, or sudden edema, require immediate evaluation for preeclampsia/eclampsia. Preeclamptic headaches often present as persistent, refractory frontal or occipital pain unresponsive to standard analgesics and may precede seizures (eclampsia), necessitating urgent magnesium sulfate administration and obstetric intervention.
Postpartum headaches may also signal complications like post-dural puncture headache (from epidural anesthesia), cerebral venous thrombosis, or reversible cerebral vasoconstriction syndrome. Always coordinate headache management with your obstetrician and neurologist. Medication safety during breastfeeding follows similar principles; most migraine-specific triptans and NSAIDs demonstrate minimal infant transfer and are compatible with lactation, while ergotamines and certain antiepileptics require careful consideration. Non-pharmacological strategies such as paced breathing, warm compresses, hydration optimization, and sleep hygiene take on heightened importance during the perinatal period, providing safe, effective symptom control without fetal or neonatal exposure risks.
Your Path to Relief
Understanding your headache map is the first step toward managing your pain. Use it as a guide to track your symptoms, identify triggers, and have a more productive conversation with your doctor. By combining this knowledge with professional medical advice, you can find the most effective pathway to relief and get back to living your life without pain.
Effective headache management operates on three complementary pillars: acute intervention, preventive therapy, and lifestyle optimization. Acute treatments aim to abort attacks quickly while minimizing side effects and preventing progression to intractable pain. The key principle is early administration—taking medication at the first sign of headache, rather than waiting for peak severity, significantly improves efficacy and reduces total medication required. Delayed treatment allows peripheral and central sensitization to escalate, rendering medications less effective and increasing the risk of rebound headaches. Preventive strategies are indicated when headaches occur ≥4 days monthly, cause significant functional impairment, or when acute medications are contraindicated or overused. These therapies require patience, as optimal results often take 6 to 8 weeks to manifest, and they work by raising the neurological threshold for attack initiation. Regular follow-up visits every 4 to 8 weeks during preventive titration allow clinicians to assess tolerability, adjust dosages, and monitor for adverse effects before committing to long-term regimens.
Non-pharmacological interventions demonstrate robust evidence across multiple headache disorders. Cognitive behavioral therapy and biofeedback teach patients to modulate physiological stress responses, reduce muscle tension, and interrupt pain-anxiety cycles. Acupuncture and cervical physical therapy address myofascial dysfunction and improve neuromuscular control. Neuromodulation devices, including transcranial magnetic stimulation (TMS), vagus nerve stimulators, and supraorbital nerve stimulators, offer drug-free options for acute and preventive management. Lifestyle foundations cannot be overstated: maintaining consistent sleep-wake cycles (even on weekends), achieving adequate hydration (roughly 2-3 liters daily, adjusted for body weight and activity), incorporating regular moderate aerobic exercise (which releases endogenous opioids and CGRP-modulating compounds), and practicing structured stress-reduction techniques all substantially reduce headache burden. Mindfulness-based stress reduction (MBSR) and acceptance and commitment therapy (ACT) have shown particular efficacy in chronic headache populations, improving pain coping mechanisms, reducing catastrophizing, and enhancing overall quality of life despite persistent symptoms.
Crucially, patients must remain vigilant about medication-overuse headache (MOH), a paradoxical condition where frequent use of acute analgesics (≥10-15 days/month) transforms episodic headaches into chronic daily pain. Breaking the MOH cycle requires structured withdrawal under medical supervision, often accompanied by transitional therapy, patient education, and initiation of preventive medications. Detoxification protocols typically span 2 to 4 weeks, with gradual tapering or abrupt discontinuation depending on the medication class, combined with supportive care, hydration, and antiemetics if needed. Patient education regarding realistic expectations, potential withdrawal symptoms, and long-term medication limits is paramount to prevent relapse. With a multidisciplinary approach combining accurate anatomical mapping, trigger management, targeted therapeutics, and professional guidance, most individuals achieve significant reduction in headache frequency, severity, and disability. Building a collaborative care team—including a primary care physician, neurologist or headache specialist, physical therapist, psychologist, and registered dietitian—creates a comprehensive support network tailored to the complex, multifactorial nature of chronic headache disorders.
Frequently Asked Questions
Can a headache map accurately diagnose my specific headache type?
A headache map is an excellent educational and communication tool, but it cannot provide a definitive medical diagnosis. Headache pain location frequently overlaps across different conditions, and primary headache disorders are diagnosed using comprehensive clinical criteria that include pain quality, duration, frequency, associated symptoms, and exclusion of secondary causes. While a map helps you articulate where you feel pain and generate informed discussions with your healthcare provider, a formal diagnosis requires a thorough neurological examination, detailed medical history, and occasionally diagnostic imaging or laboratory testing by a qualified physician.
How long should I keep a headache diary before seeing a specialist?
Most headache specialists and neurologists recommend maintaining a detailed headache diary for at least 4 to 12 weeks prior to your initial consultation. This timeframe captures sufficient data to identify cyclical patterns, track trigger correlations, evaluate medication usage frequency, and document baseline headache burden. A well-documented diary accelerates the diagnostic process, helps differentiate primary from secondary headaches, and enables your provider to select the most appropriate acute and preventive treatment strategies from your first visit. Include attack timing, duration, severity (0-10 scale), specific symptoms, all medications taken with dosages/times, potential triggers, sleep quality, and menstrual cycle days if applicable.
Are imaging tests like MRI or CT scans necessary for every headache?
Routine neuroimaging is not required for most patients presenting with a normal neurological examination and a classic history of primary headache disorders such as tension-type headache, migraine, or stable chronic headaches without recent changes. However, imaging becomes necessary when red flags are present: new onset after age 50, sudden thunderclap onset, progressive worsening, focal neurological deficits, history of malignancy or immunosuppression, headaches triggered by exertion or positional changes, or significant deviation from your established headache pattern. Your physician will determine the appropriate modality—CT for acute trauma or suspected hemorrhage, MRI/MRV for detailed soft tissue, vascular, or posterior fossa evaluation—based on your specific clinical presentation.
Is it possible to have more than one type of headache at the same time?
Yes, headache comorbidity is highly common. Many individuals meet diagnostic criteria for multiple primary headache disorders simultaneously. For example, patients with migraine frequently also experience episodic tension-type headaches, and medication-overuse headache can develop on a background of any preexisting primary headache condition. Additionally, secondary headaches (such as those from cervical spine dysfunction or chronic sinus disease) can coexist with and exacerbate primary headache disorders. This overlapping presentation is precisely why comprehensive symptom tracking and professional evaluation are essential; treating only one component while ignoring another often leads to incomplete relief. A tailored, multifaceted management plan addresses all active headache phenotypes concurrently.
Can dietary changes and supplements actually prevent headaches?
Dietary modifications and evidence-based nutritional supplements can play a significant supportive role in headache prevention, particularly for migraine and tension-type disorders. Consistent meal timing prevents hypoglycemia-induced cortical excitability, while identifying and limiting individual food triggers reduces attack frequency. Certain supplements have demonstrated clinical efficacy in randomized controlled trials: magnesium glycinate or citrate (400–500 mg daily) helps regulate neuronal excitability and neurotransmitter release; riboflavin (vitamin B2 at 400 mg daily) supports mitochondrial energy production; coenzyme Q10 (100–300 mg daily) acts as an antioxidant and anti-inflammatory agent; and omega-3 fatty acids may reduce neuroinflammatory pathways. However, supplements should be viewed as adjuncts to, not replacements for, comprehensive medical management, and patients should consult their physician before initiating high-dose supplementation, especially during pregnancy, nursing, or while taking prescription medications.
Conclusion
Navigating the complex landscape of headache disorders begins with understanding the signals your body is sending, and the headache map provides a valuable framework for interpreting those messages. By correlating pain location with characteristic symptoms, common triggers, and underlying physiological mechanisms, you gain a clearer picture of whether you're dealing with tension-type headaches, migraines, cluster episodes, sinus-related discomfort, or cervicogenic pain. However, anatomical mapping is merely the foundation of effective headache management. True diagnostic accuracy requires integrating location data with pain quality, duration, frequency, accompanying neurological or autonomic signs, and comprehensive lifestyle tracking. Modern headache medicine emphasizes a biopsychosocial model that recognizes the interplay between genetic susceptibility, environmental exposures, psychological stressors, and physiological vulnerabilities in shaping individual headache phenotypes.
Recognizing the limitations of self-assessment is equally important. Headache presentation is highly individualized, symptom overlap is common, and serious secondary conditions can initially mimic benign patterns. Knowing when to seek professional care—particularly when red flags like thunderclap onset, neurological deficits, progressive worsening, or new headaches after age 50 appear—can be life-saving. Modern headache medicine offers a robust arsenal of evidence-based treatments, from targeted acute therapies and preventive medications to neuromodulation devices, cognitive behavioral strategies, and structured lifestyle interventions. With accurate tracking, professional guidance, and a multidisciplinary approach, most individuals can significantly reduce their headache burden, prevent medication overuse, and reclaim their daily functioning. Use this guide as your starting point, document your patterns diligently, and partner with your healthcare provider to develop a personalized, sustainable management plan tailored to your unique physiology and lifestyle needs. Headache management is not a one-size-fits-all endeavor; it is an evolving journey that requires patience, education, and proactive collaboration. By leveraging anatomical awareness alongside cutting-edge therapeutics and holistic wellness practices, patients can transition from passive suffering to empowered, long-term symptom control and improved quality of life.
References
- National Headache Foundation. (n.d.). The Complete Headache Chart. headaches.org
- Santhakumar, S. (2021). Headache chart: Types by symptoms, location, and causes. MedicalNewsToday. medicalnewstoday.com
- Cleveland Clinic. (2023). Heads Up: What Your Headache Location Means. health.clevelandclinic.org
- Wei, Y., et al. (2023). Secondary headaches - red and green flags and their significance. ScienceDirect. sciencedirect.com
About the author
David Chen, DO, is a board-certified neurologist specializing in neuro-oncology and stroke recovery. He is the director of the Comprehensive Stroke Center at a New Jersey medical center and has published numerous articles on brain tumor treatment.