What Age Do Boobs Stop Growing? A Complete Medical Guide to Breast Development

Navigating the physical transformations of adolescence can feel overwhelming, especially when questions about bodily changes lack clear, scientifically grounded answers. One of the most common inquiries among young women and their caregivers centers on developmental timelines, specifically what age do boobs stop growing. Understanding this process requires a comprehensive look at human biology, endocrine signaling, genetic programming, and the natural variations that make each developmental journey unique. Breast development is not a uniform event; it is a complex, multi-phase biological process regulated by intricate hormonal networks and influenced by environmental, nutritional, and psychological factors. While societal narratives often push a rigid timeline for physical maturation, clinical research consistently demonstrates that human development operates on a broad, highly individualized spectrum. This evidence-based guide will dissect the physiological mechanisms behind mammary development, clarify realistic developmental windows, debunk pervasive myths, and provide actionable strategies for supporting breast health across the lifespan. Whether you are seeking clarity for personal understanding, parental guidance, or clinical awareness, this resource offers a medically sound, compassionate framework for navigating this fundamental aspect of human growth.
Understanding Breast Development and Puberty
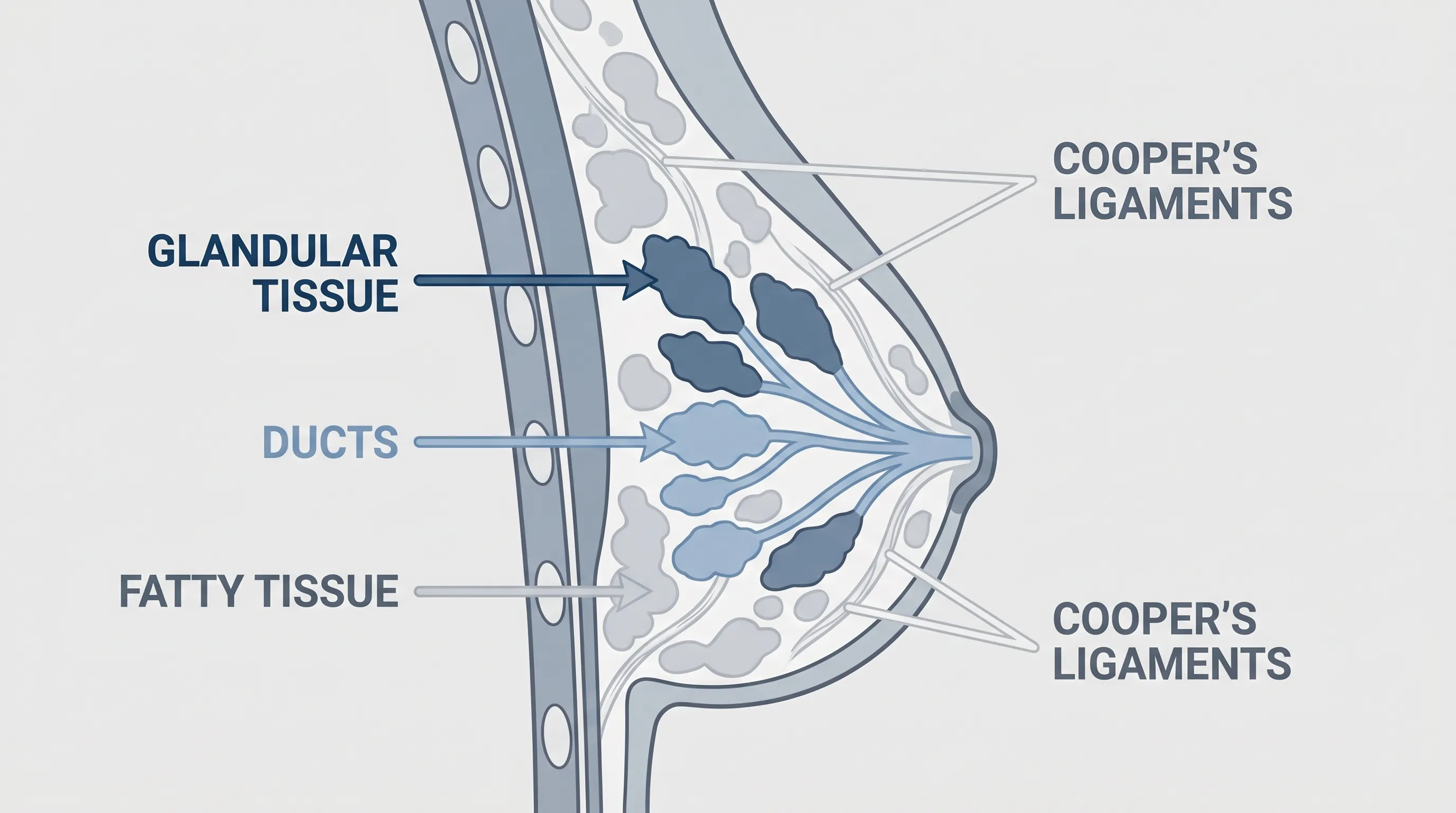
Breast development is one of the earliest and most visible markers of female puberty, signaling the activation of the hypothalamic-pituitary-gonadal axis. Anatomically, the mature breast consists primarily of glandular tissue, adipose tissue, connective tissue, blood vessels, and lymphatic structures. The glandular component includes fifteen to twenty lobes arranged radially, each containing smaller lobules responsible for milk production. These structures are interconnected via a network of lactiferous ducts that converge at the nipple. Adipose tissue determines much of the external volume and contour, while fibrous Cooper ligaments provide structural support and maintain shape against gravitational forces. During childhood, breast tissue remains rudimentary, consisting primarily of undeveloped ductal networks. Puberty triggers a remarkable cellular expansion driven by systemic hormonal shifts, transforming flat, pre-pubescent contours into mature mammary structures.
The Tanner Stages of Breast Growth
Clinicians utilize the Tanner staging system to objectively track pubertal progression. This five-phase framework provides standardized benchmarks for evaluating normal development and identifying potential endocrine irregularities.
Stage 1 represents pre-pubertal anatomy, characterized by a flat chest contour and elevated papillae without underlying glandular expansion.
Stage 2 marks the initial appearance of a palpable breast bud beneath the areola. The areolar diameter begins to increase, and early ductal branching initiates. This typically occurs between ages eight and thirteen.
Stage 3 features continued glandular enlargement and areolar expansion, though the contour remains unified without distinct secondary projection. Breast tissue becomes fuller and more conical.
Stage 4 demonstrates further maturation with the formation of a secondary mound, where the areola and papilla elevate distinctly above the primary breast contour. This phase reflects advanced lobulo-ductal differentiation.
Stage 5 represents full maturity. The areolar mound recedes into the continuous breast contour, leaving only the central nipple projection. Ductal networks achieve complete architectural branching, and adipose distribution stabilizes.
Understanding these clinical stages clarifies why asking what age do boobs stop growing rarely yields a single numerical answer. Each stage unfolds over months or years, and transition speeds vary dramatically based on genetic programming and metabolic health.
Hormonal Drivers of Breast Tissue Expansion
The endocrine orchestra behind mammary development is led primarily by estrogen and progesterone, supported by growth hormone, insulin-like growth factor one (IGF-1), and prolactin. Estrogen stimulates ductal elongation and branching, promoting the proliferation of epithelial cells within the mammary framework. Progesterone drives lobular development, preparing the tissue for potential future lactation. Growth hormone and IGF-1 act synergistically to enhance cellular division and stromal tissue formation. Leptin, secreted by adipose tissue, serves as a critical metabolic signal that informs the hypothalamus of adequate energy reserves for pubertal progression. When body fat percentage remains insufficient, leptin levels drop, often delaying hormonal cascades and subsequent breast development. This neuroendocrine feedback loop explains why nutritional status profoundly impacts pubertal timing and mammary maturation.
What Age Do Boobs Stop Growing: The Typical Timeline
When examining population-based longitudinal studies, researchers observe that breast development typically initiates between ages eight and thirteen, with a median onset around ten to eleven years. Following initial budding, the progressive expansion generally spans two to five years. Consequently, the question of what age do boobs stop growing most frequently resolves between ages seventeen and nineteen. For many adolescents, breast size stabilizes within eighteen to twenty-four months after the onset of menarche. This post-menarchal period represents a window of final glandular maturation and adipose redistribution. However, clinicians emphasize that stabilization does not equate to permanent fixation. Breast tissue remains biologically dynamic, responding continuously to metabolic and reproductive cycles.
Average Age Ranges and Developmental Milestones
Epidemiological data from the National Institutes of Health and the American Academy of Pediatrics indicate that approximately ninety percent of females reach Tanner stage four by age seventeen. Stage five, denoting full architectural maturity, typically manifests between ages seventeen and twenty. These ranges reflect aggregate trends and do not account for individual outliers. Early maturing adolescents, defined as those exhibiting breast buds before age eight, often experience accelerated timelines, frequently reaching completion by ages fifteen to sixteen. Conversely, constitutional delay of puberty shifts the entire developmental window later, with full maturation occasionally extending into the early twenties. Both trajectories remain within the spectrum of normal human variation when unsupported by pathological endocrine markers.
Why Some Women Stop Developing Earlier or Later
Several physiological and environmental variables dictate developmental pacing. Genetic ancestry influences pubertal onset, with population studies consistently showing earlier average breast development among certain demographic groups compared to others. Baseline metabolic rate, thyroid function, and childhood body composition create additional layers of variation. Adolescents with higher adiposity often experience earlier pubertal triggering due to elevated leptin signaling, though this can sometimes complicate glandular maturation if insulin resistance develops. Conversely, athletes engaged in intensive endurance training frequently exhibit delayed progression due to suppressed gonadotropin-releasing hormone pulsatility and altered estrogen metabolism. Environmental endocrine disruptors, including certain plastics, pesticides, and cosmetic chemicals, have also been investigated for their potential to accelerate or delay pubertal timing, though clinical consensus regarding direct causation remains under active research.
Genetic and Environmental Factors Influencing Growth
The blueprint for mammary development is heavily encoded within genomic architecture. Heritability studies suggest that genetic factors account for approximately sixty to eighty percent of the variance in adult breast size. Specific gene polymorphisms related to estrogen receptor sensitivity, adipocyte differentiation, and connective tissue elasticity play decisive roles in shaping developmental outcomes. When evaluating what age do boobs stop growing, clinicians first assess familial patterns. Daughters frequently follow maternal or maternal-grandmaternal developmental timelines, demonstrating the profound influence of inherited endocrine programming. However, genetics does not operate in isolation. Epigenetic mechanisms allow environmental exposures to modulate gene expression, creating complex interactions between inherited potential and lived experience.
The Role of Family History and Body Composition
Family history provides the strongest predictive indicator for breast volume, developmental pacing, and final contour. Individuals with close relatives who experienced early menarche and rapid breast expansion typically share similar trajectories. Body composition further interacts with genetic predispositions. Adipose tissue serves as both a hormonal reservoir and a structural component of the breast. Consequently, weight fluctuations directly impact apparent size, even after glandular maturation concludes. Adolescents maintaining consistent, healthy body mass indexes tend to experience smoother developmental transitions, whereas extreme caloric deficits or excesses can trigger hormonal dysregulation that alters tissue distribution. Maintaining metabolic equilibrium during puberty remains one of the most actionable strategies for supporting optimal development.
Nutrition, Exercise, and Lifestyle Impacts
Micronutrient availability profoundly influences cellular proliferation during developmental windows. Adequate protein intake provides essential amino acids for tissue synthesis. Essential fatty acids, particularly omega-three and omega-six variants, support cell membrane integrity and prostaglandin synthesis required for balanced inflammatory responses. Zinc, iodine, vitamin D, and B-complex vitamins serve as cofactors in steroidogenesis and hormonal conversion pathways. Chronic nutritional deficiencies can impair estrogen synthesis or reduce receptor responsiveness, potentially stalling glandular expansion. Regular moderate exercise enhances circulation, optimizes lymphatic drainage, and supports healthy metabolic function. However, excessive high-intensity training without adequate caloric compensation can suppress ovarian estrogen production, delaying maturation. Prioritizing balanced nutrition, restorative sleep cycles, and stress management creates an internal environment conducive to natural developmental progression.
| Developmental Phase | Typical Age Range | Primary Hormonal Activity | Key Physical Markers |
|---|---|---|---|
| Pre-Pubertal | Birth to 7-8 | Minimal gonadal activity | Flat contour, undeveloped ducts |
| Initial Budding | 8-11 | Rising estrogen, leptin threshold met | Palpable mound under areola, slight diameter increase |
| Progressive Expansion | 11-14 | Peak estrogen, progesterone initiation | Full breast enlargement, areolar expansion |
| Secondary Mound Formation | 14-16 | Stabilizing estrogen, rising progesterone | Areola projects above breast tissue |
| Adult Maturation | 17-21 | Balanced estrogen-progesterone ratio | Unified contour, complete lobular architecture |
Medical Conditions That Alter Breast Development
While natural variation accounts for most developmental differences, certain clinical conditions can disrupt typical timelines and architectural formation. Endocrine disorders represent the most common underlying causes of atypical progression. Hypothyroidism and hyperthyroidism alter basal metabolic rates and disrupt hypothalamic signaling, frequently manifesting as delayed or accelerated breast development. Polycystic ovary syndrome elevates circulating androgens while disrupting regular estrogen-progesterone cycling, often resulting in reduced glandular density, irregular tissue expansion, and significant asymmetry. Congenital adrenal hyperplasia and Turner syndrome present additional structural and hormonal deviations that require specialized endocrine management.
Hormonal Imbalances and PCOS
Polycystic ovary syndrome affects approximately one in ten reproductive-age females, fundamentally altering the hormonal milieu necessary for coordinated mammary development. Elevated luteinizing hormone pulses stimulate ovarian androgen overproduction, which competitively binds to tissue receptors and can inhibit estrogen-driven ductal expansion. Consequently, individuals with untreated PCOS may experience prolonged developmental windows, incomplete lobular formation, and pronounced tissue asymmetry. Insulin resistance frequently accompanies this condition, further complicating metabolic signaling and adipose distribution patterns. Addressing underlying insulin dysregulation through targeted dietary modifications, metformin therapy, or lifestyle interventions often restores hormonal equilibrium and allows developmental processes to resume more naturally.
When to Consult a Healthcare Provider
Clinical evaluation becomes essential when developmental patterns fall significantly outside expected parameters. Medical guidance is warranted if no breast tissue develops by age thirteen, or if progression halts completely for more than twenty-four months after initial budding. Rapid, unilateral enlargement accompanied by erythema, warmth, or discharge requires prompt evaluation to exclude inflammatory or neoplastic processes. Severe asymmetry causing mechanical discomfort, postural strain, or psychological distress also merits professional assessment. Pediatric endocrinologists and adolescent gynecologists utilize bone age radiography, hormone panels, and pelvic ultrasonography to differentiate constitutional delays from pathological endocrine dysfunction. Early intervention ensures accurate diagnosis, prevents unnecessary psychological distress, and establishes appropriate therapeutic pathways when medically indicated.
Debunking Common Myths About Breast Growth
The commercial wellness industry frequently exploits developmental uncertainty, promoting unverified products and pseudoscientific methodologies that promise accelerated growth or permanent volume enhancement. Understanding what age do boobs stop growing scientifically empowers individuals to recognize marketing claims that contradict established medical physiology. Breast tissue does not respond to topical applications, mechanical massage, or isolated dietary supplements in the manner advertised by commercial vendors. Clinical trials consistently demonstrate that non-prescription interventions fail to stimulate true glandular proliferation or alter genetically programmed architectural boundaries.
Do Supplements Actually Work?
Herbal formulations containing fenugreek, saw palmetto, pueraria mirifica, wild yam, and dong quai are heavily marketed as natural breast enhancers. While some botanicals contain phytoestrogens capable of weakly binding to estrogen receptors, systematic reviews reveal inconsistent, transient effects at best. More concerning, unregulated phytoestrogen concentrations can disrupt endogenous hormone synthesis, potentially triggering menstrual irregularities, mood fluctuations, or hepatic strain. The National Institutes of Health notes that the regulatory framework does not require pre-market efficacy testing for dietary supplements, leaving consumers vulnerable to contaminated or mislabeled products. Medical professionals strongly advise against self-prescribing hormonal modulators without comprehensive endocrine evaluation and clinical supervision.
The Truth About Exercise and Breast Size
Fitness culture frequently misrepresents anatomical realities by claiming that specific chest exercises directly increase breast volume. Exercise cannot generate glandular or adipose tissue within the mammary structures. However, strengthening the underlying pectoralis major and minor muscles creates a supportive foundation that lifts breast tissue, improves projection, and enhances overall chest aesthetics. Postural correction exercises targeting the rhomboids, trapezius, and deep cervical flexors further optimize thoracic alignment, reducing the appearance of sagging and minimizing strain on Cooper ligaments. Integrating balanced strength training, cardiovascular conditioning, and mobility work supports systemic health without promising unrealistic anatomical alterations.
Managing Expectations and Embracing Body Positivity
The psychological dimensions of breast development frequently receive inadequate attention despite their profound impact on self-esteem, social confidence, and emotional wellbeing. Media saturation, digital comparison culture, and historical beauty standards create unrealistic expectations that diverge significantly from biological reality. When individuals ask what age do boobs stop growing, they often seek reassurance that their current appearance will remain stable and socially acceptable. Healthcare providers emphasize that breast morphology exists across an exceptionally broad, naturally occurring spectrum. Symmetry, volume, contour, and pigmentation vary extensively among healthy individuals, with no single configuration representing a clinical or aesthetic ideal.
Psychological Impacts of Developmental Variations
Adolescents experiencing asynchronous development frequently report heightened anxiety, social withdrawal, and negative body image assessments. Severe asymmetry or perceived inadequate volume can trigger depressive symptoms, disordered eating patterns, and avoidance behaviors. Cognitive-behavioral interventions, peer support networks, and psychoeducational resources demonstrate high efficacy in restructuring maladaptive thought patterns. Professional counseling helps individuals differentiate between culturally constructed beauty metrics and authentic biological diversity. Parents and educators play crucial roles by modeling body neutrality, avoiding weight-focused commentary, and validating emotional experiences without reinforcing appearance-based worth.
Practical Tips for Comfort and Confidence
Implementing evidence-based comfort strategies significantly improves daily functioning and psychological resilience. Accurate bra fitting remains foundational. Approximately eighty percent of individuals wear incorrectly sized undergarments, leading to shoulder grooving, rib cage restriction, inadequate tissue support, and accelerated connective tissue strain. Professional fitting services measure both band circumference and cup volume while accounting for root width, projection, and tissue density. Selecting breathable fabrics with appropriate stretch recovery minimizes skin irritation and supports lymphatic circulation. For adolescents experiencing rapid growth phases, adjustable closures and modular cup designs accommodate weekly volume fluctuations without compromising support. Consistent skin hydration using fragrance-free, hypoallergenic formulations maintains epidermal elasticity, particularly when stretch marks develop during rapid tissue expansion. Integrating gentle thoracic mobility routines, posture awareness exercises, and sleep optimization creates a holistic framework for lifelong breast comfort and confidence.

Frequently Asked Questions
What is the average age for breast growth to stop?
Clinical research indicates that breast development typically concludes between ages seventeen and nineteen for the majority of individuals. Final maturation usually occurs within two to four years following the onset of the first menstrual period, though constitutional variation can extend this window into the early twenties.
Does breast size continue changing after puberty ends?
Yes. While glandular architecture stabilizes after developmental completion, adipose tissue remains metabolically active throughout adulthood. Weight fluctuations, menstrual cycle variations, pregnancy, lactation, and menopausal transitions continuously influence volume, density, and contour.
Can specific exercises increase breast size?
Targeted strength training cannot stimulate glandular proliferation or adipose accumulation within breast tissue. However, developing the pectoral musculature improves structural support, enhances projection, and optimizes posture, creating a lifted, more defined appearance without altering actual volume.
Are breast development supplements safe and effective?
Current medical evidence does not support the efficacy of over-the-counter breast enhancement supplements or topical formulations. Many contain unregulated phytoestrogens that may disrupt natural endocrine function. Healthcare providers recommend consulting an endocrinologist or gynecologist before using hormonal modulators.
When should I consult a doctor about delayed or asymmetrical breast growth?
Medical evaluation is recommended if no breast tissue develops by age thirteen, progression halts for over twenty-four months, menstruation does not begin by age fifteen, or severe asymmetry causes mechanical discomfort or significant psychological distress. Early specialist consultation ensures accurate assessment and appropriate intervention pathways.
Key Takeaways
Understanding what age do boobs stop growing requires moving beyond simplistic timelines and embracing the biological complexity of human development. Breast maturation follows a highly individualized trajectory governed by genetic programming, endocrine regulation, metabolic health, and environmental influences. While the majority of individuals reach full glandular maturity between ages seventeen and nineteen, natural variation remains both normal and expected. Rather than pursuing unverified enhancement methods or comparing personal development to manufactured ideals, prioritizing metabolic equilibrium, professional bra fitting, strength training, and psychological resilience yields lasting benefits. When developmental concerns arise, consulting qualified healthcare providers ensures accurate assessment, appropriate intervention, and evidence-based guidance. Ultimately, honoring the diverse, dynamic nature of human physiology fosters sustainable wellbeing and authentic body confidence across every life stage.

About the author
Sofia Rossi, MD, is a board-certified obstetrician-gynecologist with over 15 years of experience in high-risk pregnancies and reproductive health. She is a clinical professor at a top New York medical school and an attending physician at a university hospital.