Understanding Discharge After Ovulation: What Changes Mean for Your Health

Noticing changes in your vaginal discharge can feel confusing, but understanding the physiological rhythm of your menstrual cycle reveals a highly predictable, hormone-driven process. Discharge after ovulation undergoes a distinct transformation that serves both reproductive and protective functions. Rather than viewing these shifts as arbitrary, recognizing them provides valuable insight into your hormonal health, fertility window, and overall vaginal wellness. Throughout the menstrual cycle, cervical mucus acts as a dynamic biological barometer, responding to fluctuating estrogen and progesterone levels with remarkable precision. For individuals tracking their fertility, managing reproductive goals, or simply seeking greater bodily awareness, observing these changes offers a non-invasive, clinically validated window into what your endocrine system is doing behind the scenes. For comprehensive clinical guidance on menstrual physiology and cervical mucus tracking, refer to resources from the Mayo Clinic and the National Institutes of Health (NIH). This comprehensive guide explores the science, tracking methods, clinical distinctions, and lifestyle factors that shape cervical mucus during the post-ovulatory phase, empowering you with evidence-based knowledge to navigate your cycle confidently.
The Endocrinology Behind Cervical Mucus Dynamics
Cervical mucus is not a static fluid but a highly responsive biological secretion produced by crypts within the cervix. Its primary function is to create a selective environment that either facilitates or restricts sperm passage, depending on where you are in your menstrual cycle. The transformation you observe in discharge after ovulation is fundamentally governed by two primary hormones: estrogen and progesterone. Understanding how these chemical messengers interact with cervical tissue is essential for interpreting cycle changes accurately and distinguishing normal physiology from potential imbalances. Detailed endocrine pathways and reproductive hormone functions are thoroughly documented by the NIH.
The Follicular Phase and Estrogen Dominance
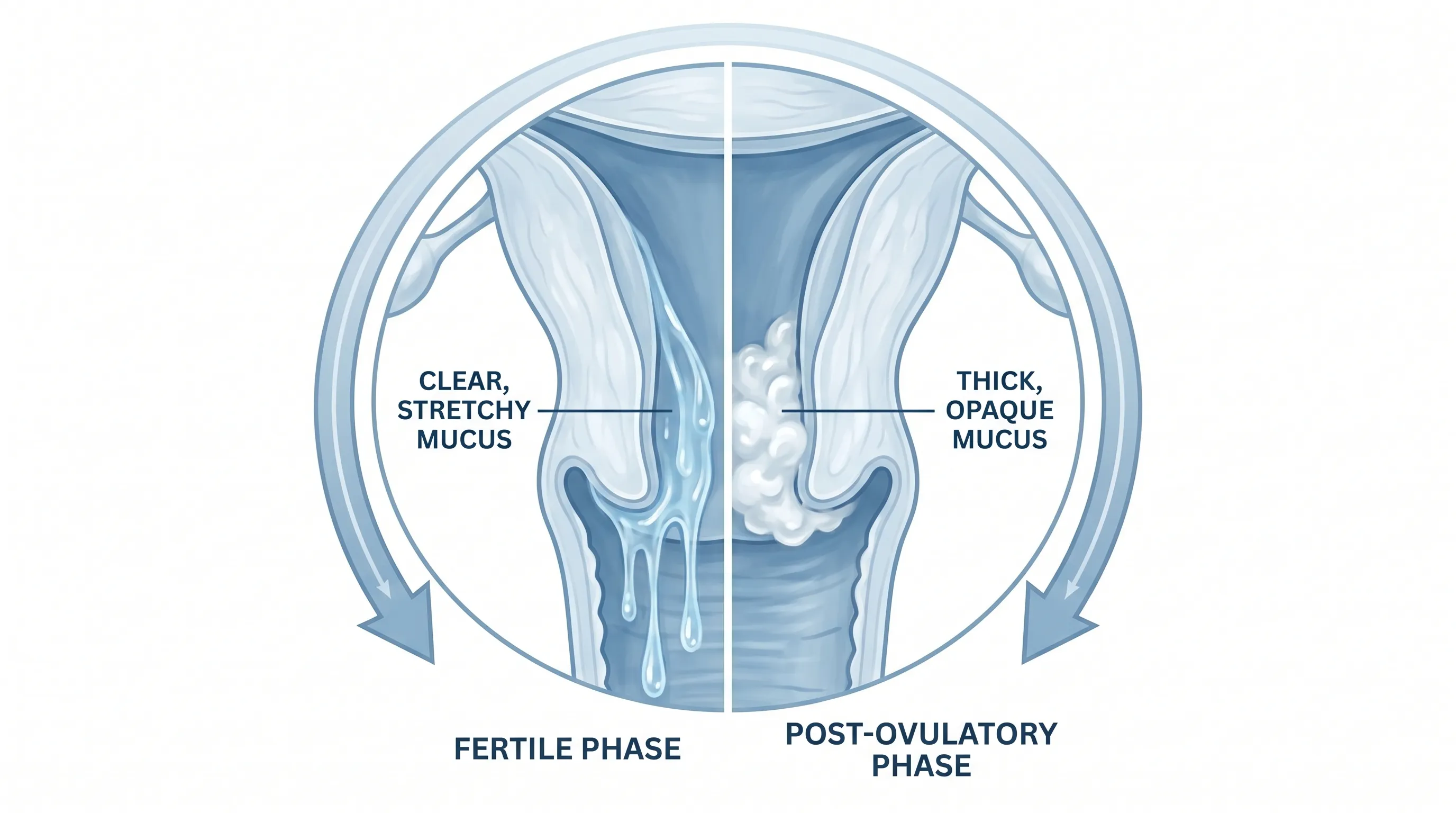
During the follicular phase, which begins on the first day of menstruation and extends through ovulation, estrogen levels gradually rise as ovarian follicles mature. Estrogen stimulates the cervical crypts to increase production of a thin, watery secretion rich in glycoproteins. As estrogen peaks just before ovulation, the mucus becomes highly hydrated, clear, and exceptionally elastic—a quality clinicians refer to as spinnbarkeit. At this stage, cervical mucus can stretch over an inch between two fingers and exhibits a microscopic ferning pattern when dried. This highly fertile state lowers vaginal pH slightly and creates microchannels that protect sperm from the naturally acidic vaginal environment, allowing them to survive for up to five days as they journey toward the fallopian tubes. This process aligns with established reproductive biology outlined by the Cleveland Clinic.
The luteinizing hormone (LH) surge that triggers ovulation coincides with the peak of this estrogen-dominant mucus phase. Many individuals using natural tracking methods rely on this clear, slippery discharge as a primary indicator that ovulation is imminent. However, once the mature follicle releases its egg, the endocrine environment shifts dramatically, initiating the next phase of cervical mucus transformation.
The Luteal Phase and Progesterone Surge
Immediately following egg release, the ruptured follicle transforms into the corpus luteum, a temporary endocrine structure that begins secreting progesterone. Progesterone is fundamentally antagonistic to the fertile mucus-producing effects of estrogen. Within hours of ovulation, rising progesterone signals the cervical crypts to reduce fluid secretion and increase the density of glycoprotein cross-linking. This biochemical shift rapidly alters the physical properties of cervical fluid. The result is discharge after ovulation that transitions from stretchy and transparent to thick, opaque, and noticeably less abundant.
This luteal phase typically spans 12 to 16 days, a remarkably consistent duration across most individuals regardless of overall cycle length. During this window, progesterone maintains elevated levels to support potential endometrial implantation. If pregnancy does not occur, the corpus luteum degenerates, progesterone levels fall, and the endometrial lining sheds as menstruation begins. The predictable nature of this hormonal cascade makes post-ovulatory cervical mucus a reliable biomarker for cycle tracking and reproductive health assessment. Clinical breakdowns of luteal phase dynamics are widely available through WHO reproductive health resources.
Physical Characteristics of Discharge After Ovulation
Recognizing the tactile and visual properties of cervical mucus during the luteal phase is crucial for accurate self-monitoring. Discharge after ovulation undergoes several distinct changes that differentiate it clearly from the fertile-window mucus observed just days prior. These physical shifts are not random but are tightly regulated physiological responses designed to alter the vaginal and cervical environment.
Consistency, Color, and Volume Shifts
The most noticeable change involves consistency. Post-ovulatory mucus loses its watery, lubricating quality and becomes noticeably thicker. Many individuals describe it as creamy, lotion-like, sticky, or pasty. The volume also decreases significantly. While the fertile window often produces enough fluid to leave a distinct wet sensation or visible marks on underwear, the luteal phase typically brings a drier, more contained discharge that may only be noticeable during routine wiping. Color transitions from transparent or clear to cloudy white, pale yellow, or slightly off-white. This opacity occurs because the thicker mucus scatters light differently and contains fewer water channels. Importantly, normal discharge after ovulation should never be foul-smelling, green, gray, or accompanied by significant irritation.
Loss of Spinnbarkeit and Elasticity
The hallmark of pre-ovulatory mucus is its remarkable stretchiness. In contrast, post-ovulatory discharge completely loses this elastic property. When rubbed between the fingers, it will typically crumble, smear, or break immediately rather than forming a continuous thread. This loss of spinnbarkeit is a direct clinical marker that ovulation has already occurred. In fertility awareness education, the disappearance of stretchy mucus, followed by three consecutive days of thicker or drier observations, confirms the opening of the post-ovulatory infertile phase. Understanding this tactile shift removes guesswork and provides a clear, objective sign that the fertile window has closed for the current cycle.
| Characteristic | Pre-Ovulation (Follicular/Periovulatory) | Post-Ovulation (Luteal Phase) |
|---|---|---|
| Consistency | Thin, watery, slippery, stretchy | Thick, creamy, sticky, pasty |
| Color | Clear or transparent | White, cloudy, pale yellow |
| Volume | High, often noticeable wetness | Low to moderate, often dry feeling |
| Elasticity | Stretches >1 inch between fingers | Breaks immediately, no stretch |
| Primary Hormone | Rising and peaking estrogen | Dominant progesterone |
| Biological Function | Facilitates sperm transport | Creates protective cervical barrier |
This comparative framework aligns with clinical observations documented by reproductive endocrinologists and serves as the foundation for symptothermal tracking protocols used worldwide.
The Biological Purpose and Protective Mechanisms
While many focus on cervical mucus primarily for fertility timing, discharge after ovulation serves equally vital defensive roles within the female reproductive system. The physiological shift is not merely a byproduct of hormonal fluctuation; it is a highly evolved mechanism designed to protect the uterus and maintain internal homeostasis during the critical window when the body prepares for potential pregnancy.
Formation of the Cervical Mucus Plug
Progesterone-induced thickening of cervical mucus contributes to the formation of a functional cervical plug. This viscous barrier physically obstructs the cervical os, preventing pathogens, debris, and non-viable cells from ascending into the uterine cavity. During the luteal phase, the endometrium thickens in anticipation of embryo implantation. If bacteria or environmental contaminants were to reach the uterus during this vulnerable period, they could trigger inflammation, disrupt implantation, or lead to pelvic infections. The post-ovulatory mucus plug acts as a selective filter, maintaining a sterile or near-sterile environment for the developing endometrial lining. Even if conception does not occur, this protective barrier remains essential for overall pelvic health and cycle regularity.
Microbiome Support and Ascending Infection Prevention
The vaginal microbiome relies heavily on Lactobacillus species to maintain an acidic pH between 3.8 and 4.5. Cervical mucus interacts dynamically with this microbial ecosystem. The thicker consistency of discharge after ovulation reduces the rapid washout of beneficial bacteria, helping stabilize vaginal flora during the luteal phase. Additionally, progesterone promotes glycogen deposition in vaginal epithelial cells, which Lactobacilli metabolize into lactic acid. This acidification further deters pathogenic overgrowth. Understanding this symbiotic relationship highlights why interventions like douching or harsh scented washes are counterproductive. Disrupting the natural mucus barrier and pH balance can inadvertently increase susceptibility to bacterial vaginosis or yeast overgrowth, particularly during hormonal transition windows. For evidence-based prevention and treatment guidelines, consult the CDC and NIH.
Clinical Tracking and Fertility Awareness Methods
Tracking cervical mucus changes has evolved from anecdotal observation into a clinically recognized practice supported by decades of research in reproductive medicine. Symptothermal fertility awareness-based methods (FABMs) integrate temperature tracking with daily mucus observation to identify fertile windows, confirm ovulation, and monitor cycle health. Understanding how to accurately observe and record discharge after ovulation is essential for anyone utilizing these evidence-based approaches.
Symptothermal Rules and the Three-Day Standard
Clinical protocols for fertility awareness establish clear, standardized rules for interpreting cervical mucus shifts. The most widely validated guideline states that the post-ovulatory phase begins after the peak fertile day and requires three consecutive days of dry, sticky, or thick mucus to confirm ovulation has passed. This three-day rule accounts for the slight delay between the actual release of the egg and the full progesterone-mediated thickening of cervical fluid. Once confirmed, individuals are generally in a sustained infertile phase until the next menstruation begins. Organizations like the American College of Obstetricians and Gynecologists and research institutes behind methods such as the Creighton Model and Marquette Method have published peer-reviewed data validating these observation standards when practiced correctly. Comprehensive fertility awareness guidelines are also maintained by the CDC. Consistency in daily tracking, rather than sporadic observation, is what yields reliable clinical insights.
Practical Daily Observation Techniques
Accurate tracking requires a systematic approach. Begin by checking your discharge at the same time each day, preferably before using the toilet in the morning. Gently wipe the vaginal opening from front to back with clean toilet paper or use a washed finger to collect a small sample. Avoid using lubricants, vaginal washes, or spermicides prior to observation, as these artificially alter consistency and color. Assess three primary parameters: consistency (does it feel dry, sticky, creamy, or wet?), color (clear, white, yellow, or other?), and stretch (does it break immediately or stretch between fingers?). Record your findings in a dedicated journal or reputable tracking application. Over several cycles, you will establish a personal baseline that makes deviations easier to recognize. This disciplined practice not only supports family planning but also provides early warning signs for hormonal shifts, stress impacts, or nutritional deficiencies.
Distinguishing Normal Physiology from Pathological Changes
While discharge after ovulation follows a predictable physiological pattern, not all changes during the luteal phase are benign. Recognizing the boundary between normal hormonal responses and signs of infection or endocrine disruption is crucial for timely clinical intervention. Vaginal health relies on maintaining a delicate equilibrium, and deviations in mucus characteristics often serve as the first noticeable indicator of underlying imbalances.
Infections, Imbalances, and When to Seek Care
Bacterial vaginosis (BV), vulvovaginal candidiasis (yeast infection), and sexually transmitted infections can alter cervical mucus characteristics at any point in the cycle. BV often presents with thin, grayish-white discharge accompanied by a distinct fishy odor, particularly after intercourse or during menstruation. Yeast infections typically produce thick, white, cottage cheese-like discharge with intense vulvar itching and erythema. Trichomoniasis and other STIs may cause frothy, yellow-green discharge alongside dysuria or pelvic discomfort. Importantly, these infections are not caused by normal luteal phase changes but by microbial overgrowth or pathogenic exposure. If your usual post-ovulatory mucus suddenly becomes excessively watery, unusually odorous, or accompanied by irritation, professional evaluation is necessary. Swabs, pH testing, and microscopic examination allow clinicians to differentiate between normal progesterone-driven thickening and active infections requiring targeted treatment. Clinical symptom checkers and diagnostic pathways are available through Mayo Clinic and CDC STI resources.
Red Flags: Odor, Irritation, and Abnormal Bleeding
Certain symptoms warrant immediate medical attention regardless of where you are in your cycle. Foul or metallic odors that persist beyond mild cycle-related changes, persistent itching or burning that interferes with daily activities, pelvic pain unrelated to typical menstrual cramping, or unexpected spotting during the luteal phase are clinical red flags. Abnormal bleeding between ovulation and your next period may indicate hormonal imbalances, polyps, fibroids, or early pregnancy complications. Tracking your discharge after ovulation helps you establish a personal normal, making it easier to recognize when something falls outside your typical pattern. Proactive communication with a gynecologist ensures accurate diagnosis and prevents minor disruptions from progressing into chronic reproductive health concerns.
Lifestyle, Hygiene, and Vaginal Health Optimization
While hormones drive cervical mucus production, external lifestyle factors significantly influence vaginal microbiome stability, hydration levels, and overall cycle regularity. Adopting evidence-based hygiene practices and supporting your endocrine system through daily habits can enhance the predictability of your discharge after ovulation and promote long-term reproductive wellness.
Microbiome-Friendly Habits and Daily Care
Vaginal health is deeply connected to microbiome preservation. The simplest and most effective practice is to wear breathable cotton underwear that minimizes moisture buildup and heat retention. Avoid synthetic fabrics that trap humidity and create environments conducive to pathogenic growth. Never douche or use internal cleansing products. The vagina is self-cleaning, and introducing harsh chemicals or altering pH levels strips away protective lactobacilli, often triggering rebound infections. External washing should involve only warm water or mild, unscented soap applied to the vulva. During your cycle, change menstrual products regularly, and consider menstrual cups or period underwear made from medical-grade, breathable materials. If you experience persistent dryness or irritation during the luteal phase, consult a provider about pH-balanced external moisturizers rather than attempting internal treatments that could disrupt natural mucus function. Global hygiene recommendations are further supported by WHO guidelines.
Nutrition, Hydration, and Stress Modulation
Systemic hydration directly impacts the water content of cervical secretions. Chronic mild dehydration can make post-ovulatory discharge feel excessively dry or pasty, even within normal hormonal parameters. Aim for consistent daily water intake and incorporate foods rich in omega-3 fatty acids, antioxidants, and B vitamins, which support hormone metabolism and mucosal membrane health. Chronic stress elevates cortisol, which can interfere with the hypothalamic-pituitary-ovarian axis, potentially delaying ovulation or altering progesterone production. This disruption manifests as irregular mucus patterns, including delayed or inconsistent discharge after ovulation. Prioritizing sleep hygiene, engaging in regular moderate exercise, and practicing mindfulness-based stress reduction techniques support endocrine balance. The physiological impact of stress on reproductive hormones is extensively reviewed in NIH research. When lifestyle foundations are solid, cervical mucus patterns become more predictable, and cycle-related fluctuations align closer to clinical norms.

Pregnancy Implications and Early Conception Signs
For individuals trying to conceive or those concerned about unexpected pregnancy, interpreting cervical mucus during the two-week wait between ovulation and expected menstruation generates significant attention. Understanding how discharge after ovulation differs from early pregnancy signs reduces unnecessary anxiety and promotes informed decision-making.
Differentiating Luteal Phase Discharge from Early Pregnancy
Both the normal luteal phase and early pregnancy are dominated by progesterone, which is why discharge characteristics often overlap significantly. Thick, creamy, white discharge is entirely normal after ovulation and does not indicate conception on its own. If fertilization and implantation occur, sustained progesterone combined with rising estrogen and human chorionic gonadotropin (hCG) may increase vaginal secretions slightly, leading to a more noticeable creamy or milky consistency. However, this increase is typically gradual and subtle. Relying on mucus changes alone to diagnose pregnancy is clinically unreliable. The most accurate approach combines symptom observation with properly timed home pregnancy tests, ideally taken on or after the first day of a missed period, alongside confirmation from a healthcare provider if needed. Early pregnancy indicators and clinical testing guidelines are thoroughly documented by Mayo Clinic.
Hormonal Overlap and Implantation Windows
Implantation typically occurs six to ten days after ovulation. During this narrow window, some individuals notice light spotting or a brief change in discharge color due to endometrial remodeling. These signs are mild, short-lived, and not experienced universally. The continued presence of thick, odorless, non-irritating discharge after ovulation remains a normal physiological state regardless of pregnancy status. Tracking your patterns over multiple cycles helps you recognize your personal baseline, making it easier to distinguish routine luteal phase changes from notable deviations. If you experience prolonged heavy discharge, severe cramping, or unusual bleeding during the implantation window, medical consultation ensures appropriate evaluation and rules out ectopic pregnancy or hormonal insufficiency.
Frequently Asked Questions
How soon does discharge change after ovulation?
Cervical mucus typically begins thickening within 24 to 48 hours after ovulation. This shift is driven by the rapid rise in progesterone secreted by the corpus luteum, which transforms the once clear, stretchy fertile fluid into a thicker, creamier, or drier consistency that persists until menstruation begins.
Can thick white discharge after ovulation indicate pregnancy?
Thick white discharge after ovulation is primarily a normal luteal phase response to progesterone. While early pregnancy can also present with increased creamy white discharge due to sustained progesterone and rising estrogen, this change alone is not a reliable pregnancy indicator. A missed period and a positive home pregnancy test remain the standard clinical confirmation methods.
Why does discharge feel drier after ovulation?
Progesterone downregulates cervical crypt secretions and increases mucus viscosity by altering glycoprotein cross-linking. This physiological mechanism reduces hydration at the cervical os, creating the characteristic dry or pasty sensation. This natural barrier protects the uterus and maintains vaginal pH balance during the non-fertile window.
How do I accurately track discharge for fertility awareness?
Track daily at a consistent time by gently wiping the vaginal opening with clean toilet paper or using a finger. Note color, consistency, volume, and stretchiness. A sustained shift to thick, dry, or sticky mucus for three consecutive days is the clinical marker confirming the post-ovulatory infertile phase in symptothermal tracking methods.
When should I contact a healthcare provider about post-ovulation discharge?
Seek medical evaluation if discharge becomes foul-smelling, green, yellow, or frothy, or if it is accompanied by itching, burning, pelvic pain, abnormal spotting, or dyspareunia. These symptoms may indicate bacterial vaginosis, yeast infections, sexually transmitted infections, or hormonal imbalances requiring clinical assessment.
Does stress affect discharge after ovulation?
Yes. Chronic stress elevates cortisol, which can disrupt the hypothalamic-pituitary-ovarian axis. This disruption may delay ovulation, alter progesterone production, or cause inconsistent cervical mucus patterns. Managing stress through sleep, exercise, and mindfulness supports more predictable luteal phase discharge and overall hormonal equilibrium.
Can hormonal contraceptives alter post-ovulatory mucus patterns?
Combined oral contraceptives and other hormonal methods suppress the natural ovulatory cycle, which eliminates the typical estrogen-to-progesterone mucus transition. Users often experience consistently thin, scant, or absent cervical mucus throughout the month. Progestin-only methods may cause thicker discharge but follow artificial hormone delivery schedules rather than natural physiological cycles.
Conclusion
Discharge after ovulation is a highly regulated, progesterone-driven physiological phenomenon that serves both reproductive timing and protective functions. By understanding how cervical mucus transitions from fertile to infertile consistency, individuals gain valuable insight into their endocrine health, fertility windows, and overall pelvic wellness. Consistent tracking, microbiome-friendly hygiene practices, and awareness of clinical red flags empower you to distinguish normal cycle variations from conditions requiring medical attention. Whether your goal is family planning, hormonal balance, or simply greater bodily literacy, recognizing the predictable rhythm of post-ovulatory discharge transforms uncertainty into informed, proactive health management. Always consult a qualified healthcare provider for personalized guidance, especially when tracking cycles for conception or managing persistent reproductive symptoms.

About the author
Sofia Rossi, MD, is a board-certified obstetrician-gynecologist with over 15 years of experience in high-risk pregnancies and reproductive health. She is a clinical professor at a top New York medical school and an attending physician at a university hospital.