Extracted Wisdom Tooth Healing: Complete Recovery Timeline & Evidence-Based Care Guide

Key points
- Maintain Gentle Oral Hygiene: Beginning 24 hours post-surgery, rinse gently with warm saline solution (1/2 teaspoon of non-iodized salt dissolved in 8 ounces of lukewarm water) two to three times daily, particularly after meals. This isotonic solution reduces bacterial load, soothes inflamed tissues, and mechanically clears food debris without disrupting the clot.
- Prioritize Head Elevation: Sleep with two or three pillows propping your head elevated above your heart for the first 48 to 72 hours. This simple gravitational adjustment significantly reduces nocturnal swelling and throbbing pain.
- Adopt a Nutrient-Rich Soft Diet: Consume cool or lukewarm foods that require minimal mastication. Excellent options include Greek yogurt, protein shakes, mashed sweet potatoes, scrambled eggs, smoothies, and lukewarm broths. Adequate protein intake (1.2 to 1.5 grams per kilogram of body weight daily) provides the amino acids necessary for collagen synthesis and fibroblast proliferation.
- Use Cold and Heat Strategically: Ice packs for the first 48 hours limit inflammation. Switch to moist heat packs thereafter to relax masticatory muscles and improve local circulation.
The removal of third molars, commonly known as wisdom teeth, is one of the most frequently performed outpatient oral surgeries in the United States, with nearly five million procedures completed annually. While the thought of dental surgery can be intimidating, understanding the biological journey of extracted wisdom tooth healing transforms anxiety into empowerment. Recovery is not a random event but a highly orchestrated physiological process involving hemostasis, inflammatory resolution, tissue proliferation, and eventual bone remodeling. Whether you are preparing for an upcoming extraction or navigating the immediate post-operative days, a comprehensive grasp of the healing timeline, evidence-based aftercare protocols, and complication management is essential for a smooth, predictable recovery.
Successful extraction recovery hinges on patient compliance. The body knows exactly how to repair the surgical site, but it requires a carefully protected environment to execute its natural regenerative programs. Factors such as nutrition, hydration, oral hygiene habits, and adherence to post-operative restrictions directly influence cellular regeneration rates and complication profiles. This guide provides an in-depth, clinically backed exploration of every phase of recovery, translating complex dental literature into actionable, patient-centered advice.
Understanding the Biology of Extracted Wisdom Tooth Healing
Dental extraction wounds heal through a sophisticated cascade of biological events that mirror general soft tissue and bone repair mechanisms, but with unique anatomical considerations. The oral cavity is a highly vascularized environment with constant exposure to microorganisms, saliva, and mechanical stress from chewing. Consequently, the body prioritizes rapid clot stabilization and epithelial migration to seal the wound against infection.
The Critical Role of the Blood Clot
Within minutes of tooth removal, vasoconstriction occurs to limit hemorrhage, followed rapidly by platelet aggregation and fibrin mesh formation. This resulting blood clot is the absolute cornerstone of extracted wisdom tooth healing. As noted in NHS clinical guidelines, "A blood clot will form over the wound, which helps it to heal. You'll be given advice about things to do for the first few days to help your recovery." This clot serves multiple vital functions: it acts as a biological bandage sealing nerve endings and underlying bone, provides a provisional matrix rich in growth factors that attract fibroblasts and osteoprogenitor cells, and creates a sterile microenvironment for initial tissue ingrowth. Disruption of this clot during the first 72 hours is the primary etiology of alveolar osteitis, commonly known as dry socket, which drastically prolongs pain and delays recovery.
Cellular Phases of Tissue Regeneration
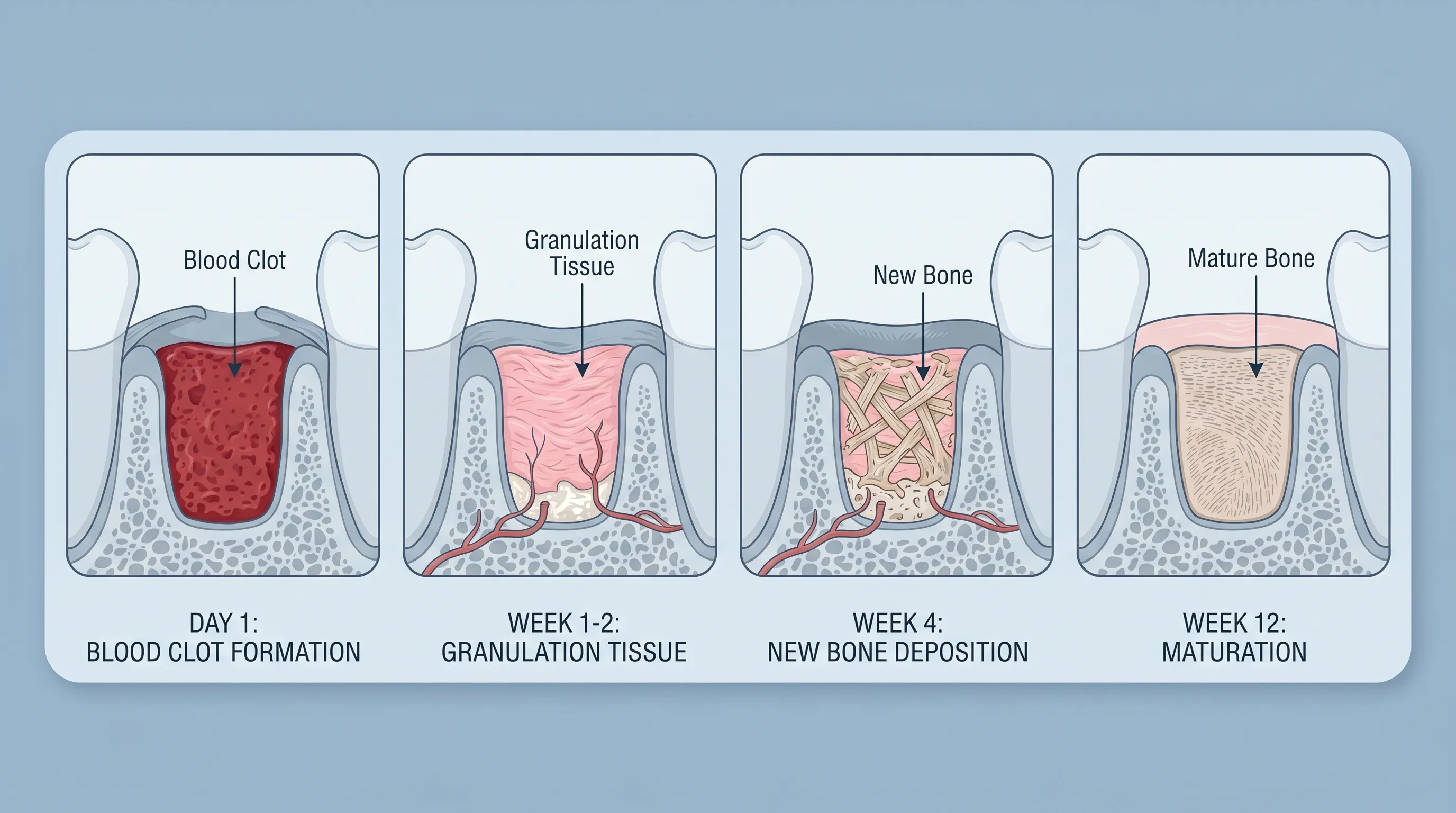
Following clot stabilization, the inflammatory phase peaks within 48 to 72 hours. Macrophages and neutrophils migrate to the site to phagocytose debris and bacteria. By days 3 to 5, the proliferative phase begins. Fibroblasts synthesize type III collagen, forming granulation tissue that gradually replaces the clot. Concurrently, endothelial cells initiate angiogenesis, establishing new capillary networks essential for delivering oxygen and nutrients. Epithelial cells at the wound margins undergo mitosis and migrate inward, progressively reducing the socket's diameter. Finally, the remodeling phase spans several weeks to months. Osteoclasts resorb initial woven bone, which is subsequently replaced by mature lamellar bone deposited by osteoblasts. This meticulous progression underscores why extracted wisdom tooth healing cannot be rushed; cellular biology operates on fixed metabolic timelines.
The Day-by-Day Healing Timeline
Clinical recovery follows a highly predictable trajectory, though individual variations exist based on surgical complexity, patient age, systemic health, and genetic factors. Understanding what to expect at each stage reduces unnecessary panic and enables timely intervention when deviations occur.
Day 1: Immediate Post-Operative Phase
The first 24 hours represent the most critical window for hemostasis and clot maturation. As local anesthesia wears off, patients typically experience a throbbing ache, moderate oozing, and initial facial swelling. Biting firmly on a sterile gauze pad for 30 to 60 minutes post-surgery applies direct pressure, promoting platelet plug stabilization. Minor oozing or blood-tinged saliva is entirely normal, but profuse bleeding requires intervention.
Swelling initiates immediately as inflammatory mediators increase vascular permeability. Applying ice packs externally in 20-minute intervals during the first 12 hours induces vasoconstriction, limiting edema formation. Patients are advised to keep their head elevated above heart level, even during sleep, to leverage gravity in reducing hydrostatic pressure at the surgical site. Numbness persists for several hours; attempting to chew or drink hot beverages before sensation fully returns risks accidental self-injury or premature clot disruption.
Days 2–4: Peak Inflammation and Management
Inflammatory responses typically culminate around 48 to 72 hours post-extraction. This period often brings maximum swelling, jaw stiffness (trismus), and peak discomfort. Trismus results from localized muscle spasm and inflammation affecting the pterygomasseteric sling. It is entirely temporary and resolves as edema subsides.
During these days, patients often require scheduled analgesics rather than waiting for pain to become severe. Alternating nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen with acetaminophen provides synergistic pain control by targeting both peripheral inflammation and central pain pathways. Transitioning to warm compresses after 48 hours enhances vasodilation, accelerating the clearance of metabolic waste and reducing muscle stiffness. Rest remains paramount; taking one to two days off work or school allows the immune system to allocate maximum resources toward tissue repair.
Days 5–14: Soft Tissue Closure and Granulation
By the end of the first week, most acute symptoms dramatically diminish. Swelling recedes, jaw mobility improves, and the extraction site begins to visibly close. Granulation tissue, appearing as a creamy yellowish or pinkish layer, replaces the initial dark clot. Patients often mistake this for pus or infection, but it is a healthy sign of proliferative healing. Dissolvable sutures, if placed, typically undergo hydrolysis and fall out naturally within 7 to 10 days.
Patients can gradually reintroduce soft solids and resume gentle brushing near the surgical site, provided no direct trauma is inflicted to the socket. The epithelial bridge across the socket forms, sealing it from the oral environment. Most individuals feel functionally normal by day 7 to 10, allowing a return to routine activities, light exercise, and standard dietary choices. As Jennifer Archibald, DDS, notes in medically reviewed literature, "Recovery typically takes between 3 days and 2 weeks" for functional normalization, though underlying structural changes continue.
Weeks 3–8: Deep Bone Remodeling
While the gum tissue appears healed, the underlying alveolar socket is actively remodeling. Osteoprogenitor cells differentiate into mature osteoblasts, depositing immature woven bone that gradually mineralizes and organizes into dense cortical bone. This radiographic closure takes 4 to 8 weeks on average. During this phase, the site may occasionally feel tender during vigorous chewing or exhibit slight clicking sensations as bone contours reshape. These sensations are benign and resolve spontaneously. Complete radiographic healing, where the socket is indistinguishable from surrounding mandibular bone on X-ray, typically concludes within 3 to 6 months.
Evidence-Based Aftercare Protocol
Optimal outcomes in extracted wisdom tooth healing are heavily dependent on meticulous post-operative self-care. The following protocols are derived from consensus guidelines published by the American Dental Association (ADA), NHS England, and peer-reviewed oral surgery literature.
Essential Do’s for Optimal Recovery
- Maintain Gentle Oral Hygiene: Beginning 24 hours post-surgery, rinse gently with warm saline solution (1/2 teaspoon of non-iodized salt dissolved in 8 ounces of lukewarm water) two to three times daily, particularly after meals. This isotonic solution reduces bacterial load, soothes inflamed tissues, and mechanically clears food debris without disrupting the clot.
- Prioritize Head Elevation: Sleep with two or three pillows propping your head elevated above your heart for the first 48 to 72 hours. This simple gravitational adjustment significantly reduces nocturnal swelling and throbbing pain.
- Adopt a Nutrient-Rich Soft Diet: Consume cool or lukewarm foods that require minimal mastication. Excellent options include Greek yogurt, protein shakes, mashed sweet potatoes, scrambled eggs, smoothies, and lukewarm broths. Adequate protein intake (1.2 to 1.5 grams per kilogram of body weight daily) provides the amino acids necessary for collagen synthesis and fibroblast proliferation.
- Use Cold and Heat Strategically: Ice packs for the first 48 hours limit inflammation. Switch to moist heat packs thereafter to relax masticatory muscles and improve local circulation.
Critical Don’ts and Risk Factors
- Avoid Smoking and Vaping Completely: Nicotine induces potent vasoconstriction, starving the healing socket of oxygenated blood and essential immune cells. Studies consistently demonstrate that smokers face a three- to fourfold increased risk of alveolar osteitis. Abstaining for at least 72 hours, preferably one week, is non-negotiable for safe recovery.
- Eliminate Suction Activities: Using straws, spitting forcefully, or playing wind instruments creates negative intraoral pressure capable of dislodging the fragile clot. Always drink directly from a glass.
- Avoid Strenuous Physical Exertion: Elevated heart rate and systemic blood pressure can rupture newly formed capillaries, causing renewed bleeding or hematoma formation. Limit heavy lifting, running, and high-intensity workouts for 5 to 7 days.
- Restrict Certain Foods and Temperatures: Hot liquids can dissolve clots prematurely. Hard, crunchy, spicy, or acidic foods can physically traumatize the socket or cause chemical irritation to exposed nerve endings. Avoid these entirely for the first 10 days.
- Do Not Drive While Impaired: Residual effects of sedation or general anesthesia can persist for 24 to 48 hours, impairing reflexes and cognitive function.
Nutritional Guidelines for Tissue Repair
Nutrition is the foundation of extracted wisdom tooth healing. Deficiencies in key micronutrients can stall epithelial migration and collagen cross-linking. Vitamin C is indispensable for hydroxylating proline and lysine residues in collagen molecules. Zinc acts as a cofactor for over 300 enzymes involved in DNA synthesis and cellular proliferation. Patients should consider supplementing with a standard multivitamin or consuming fortified foods if dietary intake is compromised by post-op appetite suppression. Hydration remains equally critical; dehydration thickens saliva, impairs immune function, and increases the risk of secondary infection. Aim for 2 to 3 liters of water daily, sipping slowly and frequently.
| Recovery Phase | Primary Physiological Process | Recommended Pain Management | Dietary Focus | Activity Level |
|---|---|---|---|---|
| Day 1 | Clot stabilization, initial hemostasis | Scheduled NSAIDs, ice therapy | Cool liquids, purees | Strict rest, head elevation |
| Days 2–4 | Peak inflammation, trismus onset | NSAID + acetaminophen alternation | Soft, lukewarm, high-protein | Light indoor activity only |
| Days 5–7 | Granulation tissue, epithelial migration | Tapering analgesics | Transition to soft solids | Sedentary work, light walking |
| Weeks 2–4 | Bone remodeling initiation | OTC only as needed | Normal diet, avoid hard edges | Moderate exercise, routine hygiene |
| Months 1–3 | Cortical bone maturation | Rarely required | Balanced, nutrient-dense diet | Full activity, dental follow-up |
Recognizing and Managing Complications
While extracted wisdom tooth healing proceeds uneventfully for the vast majority of patients, approximately 5% of routine extractions and up to 30% of surgically complex impacted mandibular extractions encounter complications. Early recognition and prompt professional intervention prevent prolonged morbidity.
Dry Socket (Alveolar Osteitis)
Dry socket remains the most common post-extraction complication. It typically manifests 2 to 4 days post-surgery when the protective blood clot is lost. Patients report sudden, severe, throbbing pain that radiates to the ear, eye, or neck on the affected side. The socket appears empty, with exposed bone that is exquisitely sensitive to air or fluids. Management requires a clinical visit where the dentist irrigates the site with sterile saline and places a medicated dressing containing eugenol or chlorhexidine to soothe nerve endings and promote secondary granulation. Pain relief is usually immediate. Prevention through strict adherence to suction-free and smoke-free protocols is vastly superior to treatment.
Post-Operative Infection
Infections typically arise from bacterial colonization of the socket or compromised immune defenses. Warning signs include pain and swelling that worsen after day 3 rather than improve, purulent exudate, foul taste or odor, lymphadenopathy, and systemic fever exceeding 100.4°F (38°C). Treatment involves professional debridement, saline irrigation, and a targeted course of antibiotics such as amoxicillin or clindamycin for penicillin-allergic patients. Maintaining gentle saline rinses and avoiding food impaction significantly reduces infection risk.
Nerve Sensitivity and Temporary Paresthesia
The inferior alveolar nerve and lingual nerve run in close proximity to lower wisdom tooth roots. Surgical retraction or bone removal can cause transient neuropraxia, resulting in numbness, tingling, or altered sensation in the lower lip, chin, or tongue. This occurs in roughly 1 to 2% of cases and typically resolves spontaneously within weeks to months as the myelin sheath regenerates. Permanent injury is exceedingly rare (<0.5%) but requires immediate neurosurgical consultation if motor deficits or persistent sensory loss extend beyond 3 months.
Prolonged Bleeding and Hemostasis
Some oozing is expected for the first 12 to 24 hours. However, continuous bleeding indicates inadequate clot formation or premature dislodgement. Initial management involves biting firmly on a moistened black tea bag for 30 to 45 minutes. Tea contains tannic acid, a natural astringent that promotes vasoconstriction and protein precipitation. If bleeding persists beyond 48 hours despite conservative measures, or if large clots are repeatedly expectorated, urgent dental evaluation is necessary to rule out coagulopathies or arterial injury.
Pain Management and Symptom Relief
Effective analgesia is not merely about comfort; unmanaged pain elevates cortisol levels, suppresses immune function, and indirectly delays extracted wisdom tooth healing. A multimodal approach targeting different pain pathways yields the best outcomes.
Pharmacological Interventions
NSAIDs like ibuprofen (400 to 600 mg every 6 to 8 hours) are first-line agents because they inhibit cyclooxygenase enzymes, reducing prostaglandin synthesis at the site of tissue injury. Combining ibuprofen with acetaminophen (500 to 1000 mg every 6 hours) provides superior analgesia compared to opioid monotherapy, with fewer side effects like nausea, constipation, or respiratory depression. Opioids should only be utilized as rescue medication for breakthrough pain in cases of multiple impacted extractions, and strictly at the lowest effective dose for the shortest duration. Always consume NSAIDs with food to protect gastric mucosa.
Natural and Supportive Therapies
Adjunctive therapies can significantly enhance comfort. Clove oil (eugenol) possesses natural analgesic and antibacterial properties. Applying a tiny amount diluted in carrier oil on a cotton swab near the socket (never directly into it) can temporarily numb pain. Arnica montana supplements or topical gels are widely used in Europe to reduce bruising and edema, though clinical evidence remains mixed. Mindfulness techniques, controlled breathing exercises, and elevating the head during rest periods activate the parasympathetic nervous system, lowering heart rate and pain perception.
Frequently Asked Questions
How long does complete extracted wisdom tooth healing take?
Soft tissue closure typically occurs within 7 to 14 days, allowing patients to resume normal eating and speaking. However, the underlying alveolar bone requires 4 to 8 weeks for structural consolidation, with full radiographic healing and complete bone density restoration taking 3 to 6 months. Age, surgical complexity, and compliance with aftercare significantly influence this timeline.
Why does my jaw feel stiff and locked after surgery?
Trismus, or jaw stiffness, results from localized inflammation affecting the masseter and pterygoid muscles, combined with trauma from keeping the mouth open during the procedure. It is a normal physiological response that peaks around days 3 to 4. Gentle warm compresses, gradual jaw stretching exercises, and anti-inflammatory medications typically restore full range of motion within 10 to 14 days.
When can I safely brush my teeth after wisdom tooth extraction?
You should brush your remaining teeth the day after surgery using a soft-bristled brush. However, strictly avoid the surgical site for the first 5 to 7 days to prevent mechanical disruption of the healing clot. Instead, rely on gentle warm saltwater rinses to keep the area clean. After one week, resume gentle circular brushing over the gum tissue surrounding the socket as tolerance allows.
Is yellow or white material in the extraction socket a sign of infection?
Not necessarily. A yellowish-white film often represents normal granulation tissue, fibrin, or food debris trapped in the socket. Unlike infectious exudate, which is accompanied by worsening pain, swelling, foul odor, and fever, granulation tissue indicates healthy healing. If you are uncertain, gently rinse with saline. Persistent thick pus, escalating pain, or systemic symptoms warrant immediate clinical evaluation.
Can I drink coffee or alcohol during recovery?\nHot coffee should be avoided for at least 48 hours, as heat and caffeine can increase local blood flow and disrupt the clot. Alcohol is strongly discouraged for the first 5 to 7 days. It dehydrates tissues, impairs immune cell function, and interacts dangerously with prescription pain medications and antibiotics. Lukewarm water, electrolyte solutions, and non-citrus herbal teas are far safer alternatives.
How do I prevent dry socket most effectively?\nThe single most impactful modifiable factor is complete cessation of smoking and vaping for at least one week post-surgery. Additionally, strictly avoid all suction activities (straws, spitting, forceful rinsing), maintain meticulous but gentle oral hygiene, follow your surgeon's prescribed analgesic regimen, and consume a soft diet. Compliance with these protocols reduces dry socket incidence from 20–30% in high-risk cases to under 2%.
Conclusion
Extracted wisdom tooth healing is a remarkably predictable biological journey when supported by informed, consistent patient care. From the critical initial 24-hour clot formation to the months-long process of alveolar bone remodeling, each phase relies on a protected environment, adequate nutrition, and disciplined adherence to post-operative guidelines. While discomfort and temporary swelling are inevitable components of the recovery process, severe complications like dry socket, infection, or nerve injury are largely preventable with proper precautions.
Patients who prioritize rest, avoid suction and nicotine, maintain gentle saline hygiene, and manage pain proactively consistently experience smoother, faster recoveries. Always maintain open communication with your dental surgeon, attend scheduled follow-up appointments, and seek immediate professional evaluation if symptoms deviate from the expected trajectory. By understanding the science behind recovery and applying evidence-based aftercare, you empower your body to regenerate efficiently, ensuring a swift return to optimal oral health and long-term dental wellness. For further reading on clinical guidelines and recovery expectations, consult the comprehensive resources provided by the NHS, Healthline's medically reviewed timelines, and the American Dental Association's patient education materials.
Remember, patience is your greatest ally. Trust the biological process, honor your body's need for rest, and follow your care team's instructions meticulously. The temporary inconvenience of recovery yields decades of improved oral alignment, reduced infection risk, and enhanced overall well-being.

About the author
Benjamin Carter, MD, is a board-certified otolaryngologist specializing in head and neck surgery, with an expertise in treating throat cancer. He is an associate professor and the residency program director at a medical school in North Carolina.