Understanding the Pubic Ramus: Anatomy, Fractures, and Recovery

Key points
- Providing structural support for the upper body. The pelvic ring operates much like a suspension bridge, distributing axial loads from the spine downward through the sacroiliac joints and pubic symphysis to the lower extremities.
- Transferring weight from the spine to the lower limbs. During gait, the pubic rami experience repetitive cyclical loading. They must absorb and dissipate these forces to prevent microdamage accumulation while maintaining joint congruency.
- Serving as attachment points for numerous muscles in the abdomen, groin, and thighs. Muscles such as the rectus abdominis, adductor longus, adductor brevis, and parts of the pelvic diaphragm originate or insert along these bony ridges. Their mechanical advantage relies heavily on the structural integrity of the rami.
- Protecting pelvic viscera. The anterior pelvic arch formed by the pubic bones shields the bladder, distal ureters, and reproductive organs from direct anterior trauma.
- Facilitating locomotion and posture. The symphysis pubis and rami complex allow for minute rotational movements that accommodate pelvic tilt during walking, running, and childbirth, making them biomechanically indispensable despite their relatively compact size.
The term "pubic ramus" often comes up in discussions about pelvic injuries, yet many people are unsure of its exact location or function. This crucial part of the pelvic bone plays a vital role in our stability and movement. A fracture in this area can be a significant, painful event, especially for older adults. Understanding the anatomy, injury mechanisms, and evidence-based treatment pathways is essential for patients, caregivers, and healthcare providers navigating this complex condition. Because pelvic injuries exist on a broad clinical spectrum—from minor stress reactions in athletes to life-threatening disruptions in high-impact trauma patients—recognizing the nuances of pubic ramus pathology is critical for optimizing outcomes.
This comprehensive guide synthesizes information from leading medical sources to cover the anatomy of the pubic ramus, the causes and types of fractures, symptoms, modern diagnostic and treatment approaches, and the path to recovery. By exploring both conservative and surgical management strategies, alongside preventive measures and rehabilitation protocols, this article aims to provide a thorough, clinically accurate resource for anyone affected by or studying this condition.
What is the Pubic Ramus? An Anatomical Overview
The pelvis is a sturdy ring of bones at the base of the spine that connects the trunk to the legs. It's composed of three main bones on each side: the ilium, the ischium, and the pubis. These bones fuse together during late adolescence to form the innominate bone, also known as the os coxae or hip bone. The pubic bone (or pubis) is the most anterior part, located at the very front of the pelvis, and it meets the pubic bone of the opposite side at the midline pubic symphysis, a fibrocartilaginous joint that allows slight movement during activities like walking and childbirth.
The term "ramus" is Latin for "branch." The pubic bone has two such branches that extend from its main body, creating a structural framework that distributes mechanical loads throughout the lower body.
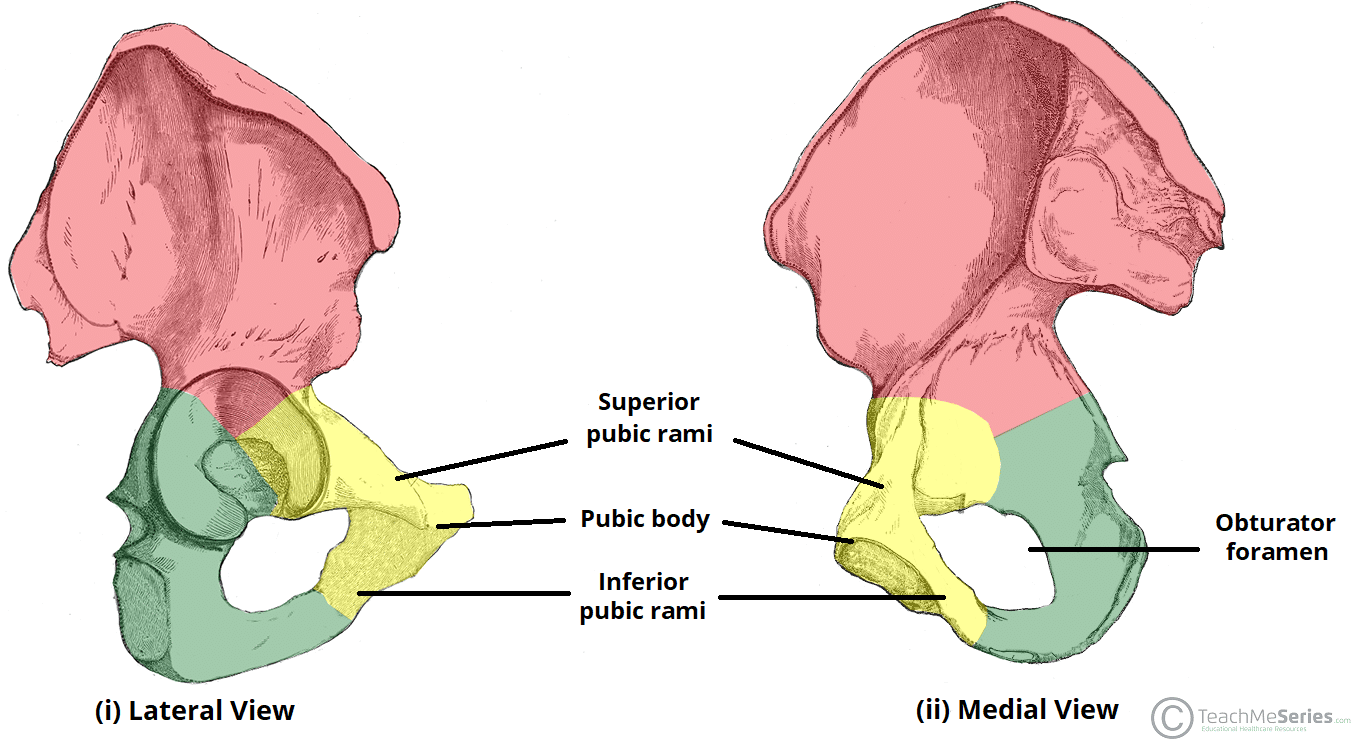 Image Source: TeachMeAnatomy
Image Source: TeachMeAnatomy
Superior and Inferior Pubic Rami
- Superior Pubic Ramus: This is the upper branch. It extends upwards and outwards from the body of the pubis, connecting to the ilium to help form the acetabulum—the socket of the hip joint. The superior ramus serves as a critical load-bearing conduit, transferring forces from the hip joint medially toward the pubic symphysis. It also provides attachment for the pectineus muscle, a primary hip flexor and adductor, and serves as a passage point for the obturator nerve and vessels.
- Inferior Pubic Ramus: This is the lower branch. It projects downwards and laterally, joining with the ramus of the ischium (the bone you sit on). The junction of these two bones forms the conjoined ischiopubic ramus. This structure is thinner than its superior counterpart but remains highly functional, providing anchor points for the adductor muscle group, the gracilis, and portions of the pelvic floor musculature, which are essential for urinary continence and core stability.
These two rami, along with the ischium, form a large opening called the obturator foramen, which allows nerves and blood vessels to pass through to the legs. The foramen is largely covered by the obturator membrane in living tissue, leaving only a small canal for the neurovascular bundle to exit the pelvis and enter the medial thigh compartment.
Function in the Pelvic Girdle
The pubic rami are integral to the pelvic ring's stability. Their key functions include:
- Providing structural support for the upper body. The pelvic ring operates much like a suspension bridge, distributing axial loads from the spine downward through the sacroiliac joints and pubic symphysis to the lower extremities.
- Transferring weight from the spine to the lower limbs. During gait, the pubic rami experience repetitive cyclical loading. They must absorb and dissipate these forces to prevent microdamage accumulation while maintaining joint congruency.
- Serving as attachment points for numerous muscles in the abdomen, groin, and thighs. Muscles such as the rectus abdominis, adductor longus, adductor brevis, and parts of the pelvic diaphragm originate or insert along these bony ridges. Their mechanical advantage relies heavily on the structural integrity of the rami.
- Protecting pelvic viscera. The anterior pelvic arch formed by the pubic bones shields the bladder, distal ureters, and reproductive organs from direct anterior trauma.
- Facilitating locomotion and posture. The symphysis pubis and rami complex allow for minute rotational movements that accommodate pelvic tilt during walking, running, and childbirth, making them biomechanically indispensable despite their relatively compact size.
Pubic Ramus Fractures: Causes and Types
A pubic ramus fracture is a break in one or both of these bony branches. As a component of the pelvic ring, it is officially classified as a type of pelvic fracture. The pelvic ring is a highly stable structure, meaning it typically requires substantial force to break. However, when the ring does fracture, it rarely occurs in isolation. Clinicians evaluate these injuries within the broader context of pelvic ring mechanics, often utilizing classification systems like the Young-Burgess or Tile classifications to predict instability, guide management, and anticipate associated injuries.
Common Causes
Fractures of the pubic ramus can occur from different types of force, each producing distinct fracture patterns and clinical presentations:
- High-Energy Trauma: In younger individuals, these fractures usually result from significant force, such as a car accident, a crush injury, or a fall from a substantial height. Anterior-posterior compression forces, lateral compression impacts, and vertical shear mechanisms all manifest differently in the pelvic ring. High-energy injuries frequently involve concurrent damage to intra-abdominal organs, major blood vessels, or the urethra and bladder, necessitating rapid trauma team activation and hemodynamic stabilization before orthopedic intervention.
- Low-Energy Trauma (Fragility Fractures): This is the most common cause in older adults. Due to weakened bones from conditions like osteoporosis, a simple fall from a standing position can be enough to cause a fracture. Age-related declines in bone mineral density, altered collagen matrix composition, and decreased estrogen or testosterone levels all contribute to skeletal fragility. Even minor mechanical stress, such as twisting in bed or slipping on a wet floor, can exceed the structural yield point of osteoporotic pubic bone.
- Repetitive Stress: Athletes, particularly long-distance runners, cyclists, military recruits undergoing intense drill, and gymnasts can develop stress fractures in the pubic ramus from overuse and repetitive impact. Stress fractures represent a physiological response to unaccustomed cyclic loading where bone resorption temporarily outpaces formation. Without adequate rest and gradual load progression, microcracks coalesce into visible cortical disruption.
- Pathological Fractures: Rarely, metastatic bone disease (such as from breast, prostate, or lung cancer), primary bone tumors, or metabolic disorders like osteomalacia and hyperparathyroidism can severely compromise bone integrity, leading to fractures with minimal or no identifiable trauma.
Stable vs. Unstable Fractures: A Critical Distinction
The most important factor in diagnosing a pubic ramus fracture is determining if it is stable or unstable. This distinction dictates the entire course of treatment.
- Stable Fracture (Isolated Injury): A stable fracture is a single break in the pelvic ring, like a crack in a pretzel. The bones are not significantly out of place. Most pubic rami fractures caused by low-energy falls are stable. They are often managed without surgery, and the prognosis is generally good. In stable injuries, the posterior tension band of the pelvis—comprising the sacrospinous and sacrotuberous ligaments and the posterior sacroiliac joint—remains intact, preserving the ring's mechanical continuity.
- Unstable Fracture (Indicator of Broader Injury): An unstable fracture means the pelvic ring is broken in two or more places, causing the entire structure to lose its integrity. A pubic ramus fracture can be one component of a much larger, unstable injury that also involves a fracture of the sacrum (the back of the pelvis) or disruption of the sacroiliac joints. As one study from the National Institutes of Health (NIH) notes, fractures of the pubic rami are often associated with overlooked posterior pelvic ring injuries. This is a severe, often life-threatening injury that typically requires surgery. Unstable patterns allow abnormal pelvic movement, which can lacerate the highly vascular presacral venous plexus or internal iliac arteries, leading to rapid hemorrhagic shock. Early recognition and volume resuscitation, often alongside pelvic binders or external fixation, are lifesaving measures in trauma bay settings.
Symptoms and Diagnosis
Recognizing the signs of a pubic ramus fracture is the first step toward getting proper care. Clinical presentation varies widely based on fracture type, patient age, and injury mechanism. Healthcare providers maintain a high index of suspicion for pelvic fractures in any patient reporting groin or lower abdominal pain following trauma, even when overt deformity is absent.
Recognizing the Signs
The most common symptoms include:
- Severe pain in the groin, hip, and/or lower back. The pain is typically sharp and localized anteriorly, though it may refer to the medial thigh due to shared innervation via the obturator nerve.
- Pain that worsens significantly with movement, walking, or standing. Patients often report an inability to perform the straight-leg raise test or roll over in bed without excruciating discomfort.
- Swelling and bruising in the pelvic or groin area. Ecchymosis may track along the inguinal ligament, perineum, or even down to the scrotum or labia (Destot's sign or Roux's sign), indicating retroperitoneal bleeding.
- Difficulty walking or inability to bear weight on the affected side. An antalgic gait or complete refusal to ambulate is highly suggestive of structural compromise.
- Numbness or tingling in the groin or legs. Neurological deficits, though less common in isolated fractures, may occur if bony fragments impinge the obturator, ilioinguinal, or genitofemoral nerves.
- Associated systemic symptoms in unstable fractures, including tachycardia, hypotension, pallor, diaphoresis, and altered mental status secondary to significant blood loss. Urethral injury may present with blood at the meatus, urinary retention, or high-riding prostate on digital exam, while bladder rupture can cause gross hematuria or peritoneal signs if intraperitoneal.
Medical Diagnosis
If a pubic ramus fracture is suspected, immediate medical evaluation is necessary. A doctor will perform a physical exam and order imaging tests to confirm the diagnosis and determine its severity. The clinical assessment begins with evaluating hemodynamic stability, followed by a gentle pelvic compression and separation test (only performed once in the trauma setting to avoid displacing unstable clots), and a thorough neurovascular examination of the lower extremities.
- X-rays: This is the initial imaging test used to identify a fracture. The standard pelvic anteroposterior (AP) view, combined with inlet and outlet views, provides comprehensive visualization of ring integrity. However, plain X-rays can sometimes miss associated fractures in the back of the pelvis (sacrum) or minimally displaced stress fractures in early stages. Subtle cortical buckling or trabecular disruption may require higher-resolution modalities for detection.
- Computed Tomography (CT) Scans: A CT scan provides detailed, cross-sectional images and is crucial for assessing the full extent of the pelvic injury, especially for identifying displacement and posterior ring injuries that classify a fracture as unstable. Multiplanar reconstructions and 3D surface rendering allow surgeons to precisely map fracture lines, plan surgical approaches, and evaluate for intra-articular extension into the acetabulum.
- Magnetic Resonance Imaging (MRI): For patients with negative X-rays but persistent, activity-related groin pain, MRI is the gold standard for detecting occult stress fractures, bone marrow edema, and soft tissue injuries. It is particularly valuable in athletes and elderly patients with atypical pain patterns where early intervention can prevent complete cortical failure.
- Bone Density Scans (DEXA): In the context of fragility fractures, a dual-energy X-ray absorptiometry scan is often ordered during the acute or subacute phase to quantify bone mineral density, confirm osteoporosis diagnosis, and establish a baseline for medical management.
 Image Source: Radiopaedia.org
Image Source: Radiopaedia.org
Treatment and Management of Pubic Ramus Fractures
Treatment is tailored to whether the fracture is stable or unstable, the patient's overall physiological reserve, comorbid conditions, and functional demands prior to injury. A patient-centered approach balances the risks of prolonged immobilization against the complications of surgical intervention, always prioritizing early mobilization to mitigate secondary morbidity.
Non-Surgical Treatment for Stable Fractures
Most isolated, stable pubic ramus fractures can be treated conservatively. The primary goals are pain control, maintenance of joint mobility, prevention of muscle atrophy, and gradual return to weight-bearing activities without risking displacement.
- Pain Management: Medications are used to control pain and make the patient comfortable. A multimodal analgesic regimen is typically preferred to minimize opioid dependence. This includes scheduled acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs) if not contraindicated by renal or gastrointestinal conditions, and short-term opioids for breakthrough pain. Neuropathic agents like gabapentin may be considered if radicular or nerve-related pain is prominent. Regional anesthesia techniques, such as fascia iliaca blocks, are increasingly utilized in acute care settings.
- Walking Aids: Patients will use crutches or a walker to limit weight-bearing on the injured side, typically for several weeks. Weight-bearing status is determined by fracture morphology and healing progress. Partial weight-bearing (25-50% of body weight) is often advanced to weight-bearing as tolerated over 2-6 weeks, contingent upon pain resolution and radiographic evidence of callus formation.
- Physical Therapy: Early mobilization under the guidance of a physical therapist is key to maintaining strength and preventing stiffness. Therapy begins with isometric contractions of the quadriceps, glutes, and adductors to preserve neuromuscular control without stressing the healing bone. Breathing exercises, seated balance drills, and safe transfer techniques are incorporated to promote independence.
- Deep Vein Thrombosis (DVT) Prophylaxis: Pelvic fractures significantly elevate the risk of venous thromboembolism due to vascular trauma, venous stasis from immobility, and hypercoagulable inflammatory responses. Mechanical prophylaxis (sequential compression devices) and pharmacological agents (low-molecular-weight heparin, fondaparinux, or direct oral anticoagulants) are routinely prescribed for 4-6 weeks post-injury, adjusted for bleeding risk and renal function.
Surgical Treatment for Unstable Fractures
Unstable fractures, where the pelvic ring is disrupted, almost always require surgery to restore alignment and stability. Surgical intervention is also indicated for open fractures, fractures with significant displacement (>1 cm), intra-articular extension, failure of conservative management, or when early mobilization is medically necessary (e.g., in polytrauma patients to prevent pulmonary complications).
- External Fixation: In emergencies, a surgeon may place pins into the iliac crests or pubic bones that connect to an external frame. This temporarily stabilizes the pelvis, reduces pelvic volume to tamponade bleeding, and allows for resuscitation and definitive planning. It may be used as a bridge to internal fixation or as definitive treatment in select cases with high soft-tissue injury risk.
- Open Reduction and Internal Fixation (ORIF): This is the most common definitive procedure. The surgeon realigns the broken bone fragments and holds them in place with metal plates and screws. According to the AO Foundation Surgery Reference, a leading resource for trauma surgeons, the goal of ORIF is to achieve a stable fixation that allows for early mobilization. Surgical approaches vary based on fracture location; anterior approaches (Pfannenstiel or modified Stoppa) provide direct visualization of the pubic rami and quadrilateral surface, while posterior approaches address sacroiliac disruptions. Minimally invasive percutaneous screw fixation is increasingly utilized for select stable patterns, reducing soft tissue dissection and accelerating recovery.
- Postoperative Care: Following ORIF, patients undergo aggressive pulmonary hygiene, DVT prophylaxis, wound monitoring, and progressive physical therapy. Hardware complications, infection risk, and heterotopic ossification formation are closely monitored through serial clinical and radiographic follow-up.
A Special Focus: Fragility Fractures in the Elderly
Pubic ramus fractures in the elderly are often called a "neglected injury." Research published by the National Institutes of Health (NIH) highlights that these fractures are far from benign. They represent a sentinel event, signaling underlying systemic bone fragility and significantly elevated fall risk.
- High Risk of Complications: They are associated with significant pain, loss of mobility, and a high one-year mortality rate. Prolonged immobilization precipitates a cascade of geriatric syndromes: pneumonia from shallow breathing, pressure ulcers from sustained supine positioning, urinary tract infections from catheterization or incomplete voiding, delirium from pain medications and environmental disorientation, and rapid sarcopenia. Each complication exponentially increases morbidity and strains healthcare resources.
- Frequently Underdiagnosed: A simple pubic ramus fracture seen on an X-ray can mask a more severe, unstable sacral fracture. This is why many experts now recommend CT scans for elderly patients with these injuries, especially if they have persistent pain and difficulty mobilizing. Occult posterior ring injuries are present in up to 40% of initially "stable" fragility fractures, fundamentally altering prognosis and treatment pathways.
- Need for Multidisciplinary Care: Optimal management requires a team approach involving orthopedic surgeons, geriatricians, physical therapists, occupational therapists, and primary care physicians. The Fracture Liaison Service (FLS) model has proven highly effective, ensuring systematic osteoporosis evaluation, pharmacological intervention (bisphosphonates, denosumab, teriparatide, or romosozumab), calcium and vitamin D repletion, home safety assessments, and balance training programs like Tai Chi or Otago exercises.
- Nutritional and Metabolic Optimization: Adequate protein intake (1.0-1.5 g/kg/day) is crucial for bone and muscle repair, often overlooked in geriatric populations prone to anorexia of aging. Correcting vitamin D deficiency, managing secondary hyperparathyroidism, and addressing malabsorption issues (e.g., celiac disease, prior bariatric surgery) form the metabolic cornerstone of recovery and secondary fracture prevention.
Recovery, Rehabilitation, and Long-Term Outlook
Recovery is a gradual process that requires patience and adherence to a rehabilitation plan. The healing trajectory is influenced by fracture severity, surgical vs. non-surgical management, age, nutritional status, smoking history, and comorbid conditions like diabetes or autoimmune disorders. Consistent follow-up ensures timely progression through rehabilitation phases while monitoring for complications.
Healing Timeline
The bone itself typically takes 6 to 8 weeks to heal. However, full recovery of strength and function can take several months to a year. Clinical and radiographic union usually precedes functional recovery. Radiographically, bridging callus formation becomes visible on X-rays around week 4-6, with cortical consolidation completing by months 3-6. Patients often notice substantial pain reduction by week 8, but endurance, core stability, and confidence in ambulation continue to improve for 9-12 months. Athletes and laborers may require 4-6 months before returning to full-duty activities, with sport-specific testing guiding safe clearance.
Standardized Rehabilitation Protocols
A structured physical therapy program is essential for a successful recovery. Rehabilitation is periodized to align with biological healing phases and progressively overloaded to stimulate tissue adaptation without compromising structural integrity.
- Early Phase (0-6 weeks): Focus on pain control, gentle range-of-motion exercises, and limited weight-bearing as instructed by the surgeon. Interventions include transcutaneous electrical nerve stimulation (TENS), cryotherapy, diaphragmatic breathing, pelvic floor awareness exercises, and safe bed-to-chair transfers. Isometric gluteal and quadriceps sets, ankle pumps, and heel slides prevent venous stasis and maintain joint capsule elasticity. Hydrotherapy or aquatic therapy may be introduced if incisions are healed and weight-bearing restrictions permit buoyancy-assisted movement.
- Mid Phase (6-12 weeks): As the bone heals, weight-bearing is gradually increased. Exercises focus on strengthening the muscles around the hip and pelvis. Progressive resistance training targets the hip abductors, extensors, and adductors using therabands, light weights, and closed-chain kinetic movements like mini-squats and step-ups. Proprioceptive drills on balance boards or foam surfaces retrain neuromuscular pathways disrupted by pain and immobilization. Cardiovascular conditioning via stationary cycling or elliptical training rebuilds aerobic capacity without high-impact joint loading.
- Late Phase (3+ months): The goal is to return to normal daily activities. Therapy will focus on improving balance, endurance, and functional mobility. Advanced functional training incorporates single-leg stance progressions, stair climbing, gait pattern normalization, and activity-specific simulations (e.g., lifting mechanics, sports agility drills). Patients are educated on long-term joint protection strategies, ergonomic adjustments, and home exercise program independence to sustain gains.
Potential Long-Term Complications
While many patients recover well, those with severe, unstable fractures can face long-term challenges, including:
- Chronic Pain: Persistent pain in the hip or lower back. May stem from post-traumatic osteoarthritis, sacroiliac joint dysfunction, nerve entrapment, or central sensitization syndromes. Multidisciplinary pain management, including cognitive behavioral therapy and interventional procedures, often yields better outcomes than prolonged opioid therapy.
- Neurological Injury: Damage to the nerves passing through the pelvis can cause weakness or sensory issues. Lumbosacral plexus injuries or obturator neuropathy may require electromyography (EMG) studies, neurolysis, or specialized rehabilitation. Nerve recovery is notoriously slow, often progressing at approximately 1 mm/day, requiring sustained therapeutic support.
- Urogenital and Sexual Dysfunction: Due to the proximity of the bladder and reproductive organs, these issues can sometimes occur. Urethral strictures, bladder dysfunction, or pudendal nerve involvement may necessitate urological or pelvic floor specialist referral. Sexual health counseling should be proactively integrated into recovery discussions to address intimacy concerns, pain with intercourse, and psychological barriers.
- Malunion or Nonunion: The fracture may heal in an incorrect position (malunion) or fail to heal at all (nonunion), which may require further surgery. Risk factors include inadequate immobilization, smoking, NSAID overuse in early healing phases, severe displacement, and poor nutritional status. Nonunion management often involves bone grafting, biophysical stimulation (ultrasound or electromagnetic fields), and revision internal fixation.
A comprehensive, multidisciplinary follow-up is critical to manage these potential issues and optimize long-term quality of life. Regular clinical assessments, patient-reported outcome measures (PROMs), and periodic imaging guide individualized care adjustments. Emphasizing psychological resilience, peer support groups, and gradual lifestyle reintegration significantly enhances overall satisfaction and functional independence post-injury.
Frequently Asked Questions
How long should I stay in bed after a pubic ramus fracture?
Prolonged bed rest is strongly discouraged. While brief periods of rest are necessary during the acute pain phase, early mobilization is a cornerstone of modern fracture care. Remaining bedridden increases the risk of life-threatening complications such as deep vein thrombosis, pulmonary embolism, pneumonia, pressure sores, and rapid muscle wasting. Most patients are encouraged to sit in a chair, perform seated transfers, and begin short, supervised walks with assistive devices within the first 24 to 72 hours post-injury or post-surgery, strictly adhering to weight-bearing restrictions outlined by their orthopedic surgeon. The goal is progressive, pain-guided movement rather than strict immobilization.
Can I drive after suffering a pubic ramus fracture?
Driving should be avoided until you can safely perform an emergency stop, comfortably operate all pedals without significant pain, and have regained adequate reaction time and lower extremity strength. This typically takes 4 to 8 weeks for non-surgical stable fractures and often 8 to 12 weeks or longer following surgery or left-sided fractures in right-hand drive vehicles. You must be off narcotic pain medications before attempting to drive, as they impair cognitive and motor function. Always obtain clearance from your surgeon or physical therapist, and consider practicing in a controlled, empty parking lot before resuming regular traffic driving. Additionally, verify with your auto insurance provider, as policies regarding recent fractures and medical clearance vary.
Are pubic ramus fractures common in pregnant women?
While pregnancy itself does not typically cause pubic ramus fractures, the physiological changes of gestation can predispose women to pelvic girdle pain and symphysis pubis dysfunction. Relaxin and progesterone naturally loosen pelvic ligaments to prepare for childbirth, while increased fetal weight alters biomechanical loading. In rare cases, women with severe underlying osteoporosis, metabolic bone disease, or those who experience high-impact trauma during pregnancy may sustain rami fractures. Management during pregnancy requires careful coordination between obstetricians and orthopedic specialists to balance maternal pain control, fetal safety, and delivery planning. Vaginal delivery may be contraindicated if significant pelvic ring instability exists, potentially necessitating a cesarean section.
What dietary changes can accelerate pubic ramus healing?
Nutrition plays a vital role in bone regeneration and soft tissue repair. Adequate caloric intake is essential, as bone healing increases metabolic demands. Prioritize high-quality protein (1.2-1.5 g/kg/day) to support collagen synthesis and muscle preservation. Ensure sufficient calcium intake (1,000-1,200 mg/day for adults, higher for elderly) through dairy, fortified plant milks, leafy greens, or supplements if deficient. Vitamin D (600-2,000 IU/day) is crucial for calcium absorption; serum 25-hydroxyvitamin D levels should ideally exceed 30 ng/mL. Vitamin C supports collagen cross-linking, vitamin K2 directs calcium to bone rather than soft tissue, and magnesium facilitates bone crystal formation. Avoid excessive alcohol and quit smoking, as both profoundly impair osteoblast function, reduce blood flow to healing bone, and significantly increase nonunion risk. Stay hydrated and maintain balanced electrolytes to support cellular repair processes.
Is surgery always necessary for bilateral pubic ramus fractures?
Not necessarily. Bilateral fractures can occur in both stable and unstable contexts. If both fractures are minimally displaced and the posterior pelvic ring (sacroiliac joints and sacrum) remains intact, the injury may still be mechanically stable and amenable to conservative management. In these cases, patients are closely monitored with weight-bearing restrictions, pain control, and early mobilization. However, bilateral fractures significantly compromise the anterior pelvic arch, often indicating higher-energy mechanisms or severe fragility. If imaging reveals displacement greater than 1 cm, rotational or vertical instability, posterior ring involvement, or failure to progress with conservative care, surgical stabilization is typically recommended. The decision is highly individualized, factoring in patient age, bone quality, functional demands, and overall medical fitness.
Conclusion
Pubic ramus fractures represent a clinically significant spectrum of pelvic injuries that demand precise diagnosis, individualized treatment, and dedicated rehabilitation. Whether resulting from high-impact trauma in younger populations or fragility fractures in the elderly, these injuries profoundly impact mobility, independence, and quality of life. The distinction between stable and unstable patterns serves as the critical pivot point in management, guiding the choice between conservative care and surgical intervention. Modern orthopedic practice emphasizes early mobilization, multimodal pain control, thromboprophylaxis, and multidisciplinary coordination to mitigate complications and optimize functional outcomes.
For older adults, a pubic ramus fracture is far more than a localized bone break; it is a warning sign of systemic skeletal vulnerability requiring comprehensive osteoporosis management, fall prevention strategies, and metabolic optimization. Meanwhile, athletes and younger patients benefit from precise imaging, structured rehabilitation protocols, and careful return-to-activity planning to prevent re-injury. Regardless of the mechanism, successful recovery hinges on patient education, adherence to rehabilitation milestones, nutritional support, and consistent follow-up with healthcare providers. By integrating evidence-based medical treatment with proactive lifestyle modifications and psychological support, patients can navigate the recovery journey with confidence and regain long-term mobility, strength, and resilience.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare professional for diagnosis and treatment of medical conditions.
References
- American Academy of Orthopaedic Surgeons (AAOS). (n.d.). Pelvic Fractures. OrthoInfo. Retrieved from https://orthoinfo.aaos.org/en/diseases--conditions/pelvic-fractures/
- van Berkel, D., et al. (2020). The truth behind the pubic rami fracture: identification of pelvic fragility fractures at a university teaching hospital. National Center for Biotechnology Information (NCBI). Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC7243566/
- AO Foundation. (n.d.). ORIF - Pubic ramus plate. AO Surgery Reference. Retrieved from https://surgeryreference.aofoundation.org/orthopedic-trauma/adult-trauma/pelvic-ring/pubic-ramus/orif-pubic-ramus-plate
- University Hospitals Dorset NHS Foundation Trust. (n.d.). Pubic rami fracture [Patient Information Leaflet]. Retrieved from https://www.uhd.nhs.uk/uploads/about/docs/our_publications/patient_information_leaflets/orthopaedics/Pubic_rami_fracture.pdf
- Upswing Health. (n.d.). What Is a Pubic Ramus Fracture & How Can You Heal Pelvic Injuries?. Retrieved from https://upswinghealth.com/conditions/pubic-ramus-fracture/

About the author
Samuel Jones, MD, is a board-certified orthopedic surgeon specializing in joint replacement and orthopedic trauma. He is a team physician for a professional sports team and practices at a renowned orthopedic institute in Georgia.