Understanding Pancreatic Cancer Poop: Warning Signs, Causes, and What to Do

Noticing a change in your bowel habits can be unsettling, but it often serves as an early biological signal that your digestive system needs attention. When tumors develop in the pancreas, they can disrupt the delicate balance of bile flow and digestive enzyme production, leading to highly noticeable alterations in stool appearance, consistency, and behavior. Understanding the connection between pancreatic health and digestive output is crucial for early detection and timely medical intervention. Many individuals dismiss subtle changes in their bathroom habits, attributing them to dietary shifts or temporary gastrointestinal upset. However, recognizing the specific characteristics of pancreatic cancer stool changes can empower patients to seek appropriate care before the condition advances. This comprehensive guide explores the physiological mechanisms behind these changes, differentiates them from common digestive disorders, outlines critical warning signs, and provides evidence-based strategies for monitoring your health. By staying informed and attentive to your body’s signals, you can navigate digestive concerns with confidence and ensure that any necessary diagnostic evaluations occur promptly.
The Digestive Connection: How the Pancreas Influences Stool
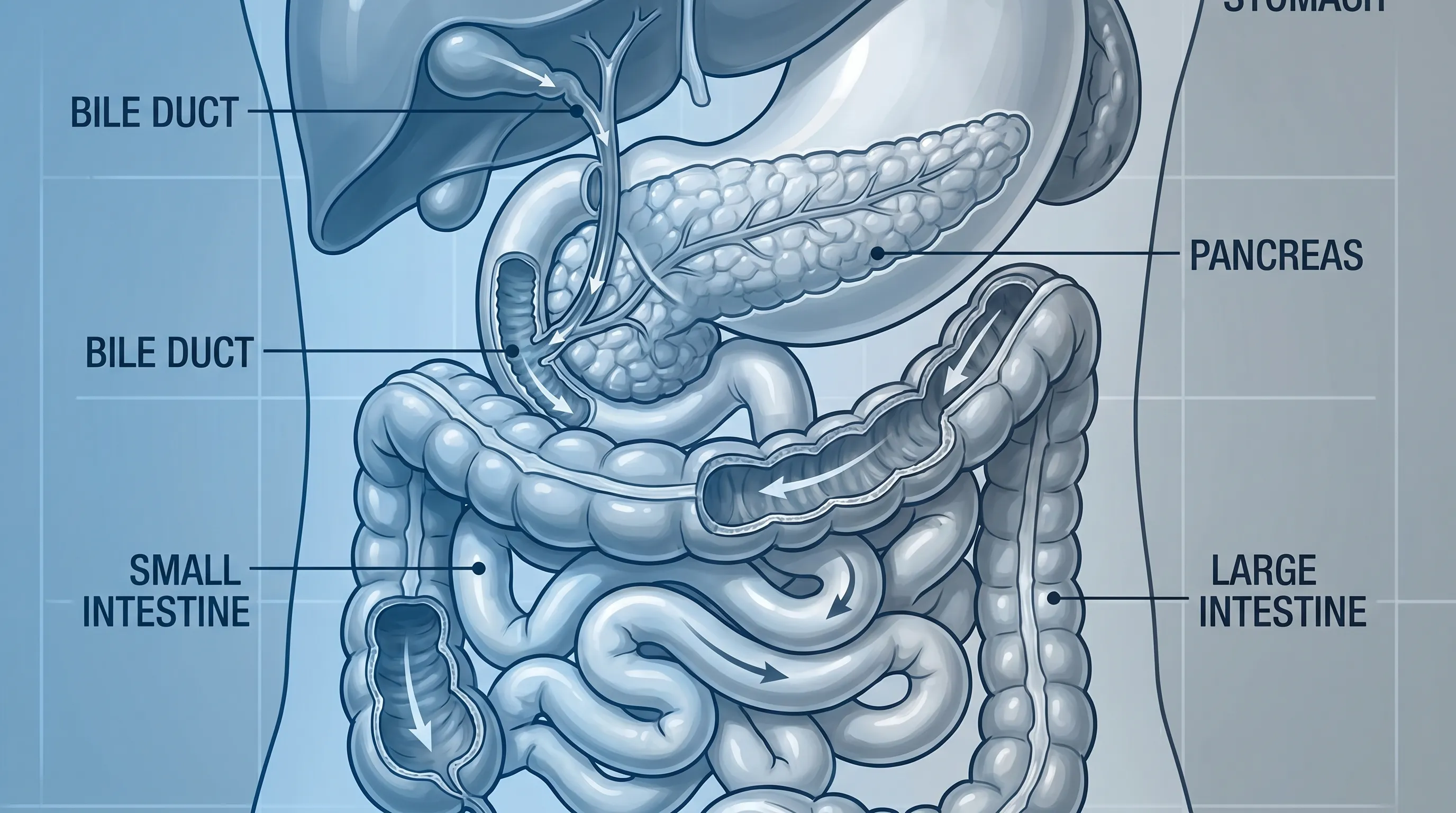
The pancreas is a vital dual-function organ located deep within the abdomen, positioned behind the stomach. It serves two primary roles: endocrine and exocrine, as detailed by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). The endocrine portion produces hormones like insulin and glucagon that regulate blood sugar, while the exocrine portion is responsible for manufacturing digestive enzymes. These enzymes, including lipase for fat breakdown, amylase for carbohydrate digestion, and protease for protein metabolism, are secreted into the small intestine to facilitate nutrient absorption. Simultaneously, the pancreas acts as a conduit for bile, a yellow-green fluid produced by the liver and stored in the gallbladder. Bile travels through the common bile duct, which passes directly through or near the head of the pancreas before entering the duodenum. Bilirubin, a byproduct of red blood cell breakdown explained by the Cleveland Clinic, gives bile its pigment and ultimately imparts the characteristic brown color to healthy stool.
When pancreatic cancer develops, it frequently disrupts this intricate anatomical and physiological harmony. Tumors typically arise from the exocrine cells of the pancreas, which account for approximately 90% of all cases. Depending on the tumor’s size, growth rate, and precise location, the disruption can manifest in several ways that directly impact bowel movements. The head of the pancreas is anatomically adjacent to the common bile duct, making it a common site for tumors that cause early bile duct compression. When bile cannot reach the intestines, the digestive process falters, and stool loses its normal coloration. Conversely, tumors located in the body or tail of the pancreas may not immediately affect bile flow but can severely compromise enzyme production. This exocrine insufficiency prevents proper breakdown of dietary fats, leading to malabsorption that drastically alters stool texture, buoyancy, and odor. Understanding this anatomical relationship clarifies why digestive changes often precede or accompany other systemic symptoms in pancreatic disease.
Mechanisms Behind Pancreatic Cancer Poop Changes
Stool alterations in pancreatic cancer are not random; they follow predictable physiological pathways driven by mechanical obstruction and biochemical deficiency. Recognizing these two primary mechanisms provides a clearer picture of what is happening internally when digestive output shifts unexpectedly.
Bile Duct Obstruction and Pigment Loss
The most common cause of dramatic stool discoloration in pancreatic cancer is mechanical blockage of the biliary system. When a tumor grows in the head of the pancreas, it frequently presses against the common bile duct, narrowing or completely sealing the passageway. Under normal conditions, bile flows continuously from the liver into the small intestine, where bilirubin undergoes bacterial metabolism to produce stercobilin, the pigment responsible for brown stool. When obstruction occurs, bilirubin cannot enter the intestines and instead backs up into the bloodstream. This accumulation triggers jaundice, a condition characterized by yellowing of the skin and the whites of the eyes. Without bilirubin reaching the colon, stools become noticeably pale, ranging from light gray to clay-colored or even chalky white. This acholic stool presentation is one of the most reliable clinical indicators of extrahepatic biliary obstruction and often prompts immediate medical investigation.
Exocrine Insufficiency and Fat Malabsorption
Pancreatic cancer frequently destroys or replaces the acinar cells responsible for synthesizing and secreting digestive enzymes. Even before a tumor causes complete obstruction, the progressive loss of healthy pancreatic tissue reduces enzyme output below the threshold required for efficient digestion. This condition, known as exocrine pancreatic insufficiency (EPI), is particularly problematic for lipid metabolism. Lipase is the primary enzyme tasked with breaking down triglycerides into absorbable fatty acids. When lipase levels drop, dietary fats remain largely undigested as they transit through the gastrointestinal tract. These unabsorbed lipids bind to water and remain suspended in the stool, creating a visibly greasy or oily appearance. The undigested fats also increase the stool’s overall volume and decrease its density, causing it to float rather than sink. Additionally, bacterial fermentation of undigested proteins and fats generates volatile organic compounds that produce a distinctly foul, rancid odor. These combined changes represent a classic presentation of steatorrhea, a hallmark of pancreatic exocrine dysfunction.
Clinical Presentation: Identifying Warning Signs
Monitoring your digestive output requires attention to specific visual and physical characteristics. While occasional dietary variations can temporarily alter stool consistency, persistent changes lasting more than a week or two warrant careful evaluation. The following breakdown highlights the most clinically significant features associated with pancreatic disease.
Color, Texture, and Consistency Variations
Healthy stool typically ranges from medium to dark brown, maintains a firm but pliable consistency, and breaks apart easily upon wiping. In contrast, pancreatic cancer poop frequently exhibits stark deviations from this baseline. Pale or clay-colored stools indicate a significant interruption in bile delivery, suggesting either pancreatic head tumors, bile duct strictures, or gallbladder pathology. The loss of pigment is often accompanied by a dry, crumbly texture that lacks the normal moisture provided by healthy bile emulsification. Alternatively, some patients experience loose, watery stools that resemble diarrhea. This occurs because undigested fats and carbohydrates draw excess water into the intestinal lumen through osmotic pressure, accelerating transit time and preventing proper stool formation. In either case, tracking these changes alongside food intake and symptom patterns can provide valuable diagnostic clues.
| Stool Characteristic | Typical Appearance in Pancreatic Disease | Primary Physiological Cause |
|---|---|---|
| Color | Pale, gray, clay-like, or unusually light yellow | Bilirubin blockage preventing normal pigment formation |
| Texture | Greasy, oily, or coated with visible fat droplets | Lipase deficiency causing incomplete fat digestion |
| Buoyancy | Floats persistently on water surface | High fat content reducing stool density |
| Odor | Unusually strong, rancid, or foul-smelling | Bacterial fermentation of undigested fats and proteins |
| Volume | Large, bulky, or excessively voluminous | Poor nutrient absorption and osmotic water retention |
Odor and Buoyancy Clues
While many people rarely notice stool odor unless it is exceptionally pronounced, a sudden, persistent change can be a significant clinical marker. The malodor associated with pancreatic-related steatorrhea is distinct from typical digestive gas or mild dietary changes. It often resembles spoiled dairy or rancid oil and tends to linger in the bathroom long after flushing. Buoyancy is another easily observable metric. Normal stool typically sinks or breaks apart partially upon hitting the water. Floating stools that remain buoyant for an extended period strongly suggest elevated fat content, which occurs when the body cannot adequately digest lipids. Keeping a simple symptom journal that records stool color, consistency, odor intensity, and accompanying abdominal sensations can streamline your conversation with a healthcare provider and accelerate the diagnostic process.

Distinguishing Pancreatic Changes from Common Conditions
It is vital to emphasize that experiencing pale, greasy, or floating stools does not automatically confirm a pancreatic malignancy. Numerous benign and highly treatable gastrointestinal conditions produce nearly identical digestive output. Differentiating these possibilities requires careful symptom correlation and professional diagnostic testing, as outlined by the CDC.
Gallbladder vs. Pancreatic Symptoms
Gallstones are among the most frequent causes of temporary bile duct obstruction and pale stools. When a stone lodges in the common bile duct, it can mimic pancreatic head tumor symptoms, including jaundice, right upper quadrant pain, and acholic stool. However, gallstone-related blockage often presents with acute, colicky pain following fatty meals and typically resolves once the stone passes or is surgically removed. Chronic pancreatitis, another significant differential, shares the steatorrhea and enzyme deficiency profile of pancreatic cancer but usually follows a history of heavy alcohol use, recurrent abdominal pain episodes, or genetic predisposition. Imaging studies and serum inflammatory markers help clinicians distinguish between chronic inflammation and malignant growth.
Celiac Disease and Inflammatory Bowel Disease
Autoimmune and inflammatory conditions frequently disrupt fat absorption and produce greasy stools. Celiac disease triggers an immune response to gluten that damages the small intestinal lining, reducing surface area for nutrient uptake. Crohn’s disease and ulcerative colitis cause chronic intestinal inflammation that accelerates transit time and impairs fat processing. Both conditions typically present with additional markers like anemia, joint pain, skin rashes, or visible blood in the stool. Liver disease, including hepatitis or cirrhosis, reduces bilirubin conjugation and bile salt production, leading to similar stool discoloration. Certain medications, such as orlistat (a weight-loss drug that intentionally blocks fat absorption) or high-dose antibiotics, can also temporarily alter stool consistency. A thorough medical history, targeted blood work, and imaging effectively separate these manageable conditions from more serious pancreatic pathology.
Associated Symptoms That Require Immediate Attention
Stool changes rarely occur in isolation when pancreatic cancer is present. The disease typically generates a constellation of systemic and localized symptoms that collectively signal the need for comprehensive medical evaluation. Recognizing these accompanying warning signs significantly improves diagnostic accuracy and intervention timelines.
Jaundice and Skin Manifestations
Yellowing of the skin and sclera is one of the most visible and reliable indicators of biliary obstruction. As bilirubin accumulates in the bloodstream due to blocked bile flow, it deposits in cutaneous and ocular tissues, creating a distinct yellow hue. Jaundice is frequently accompanied by intense pruritus (itching) caused by bile salt deposition under the skin. Dark urine, ranging from amber to cola-colored, occurs because the kidneys filter excess conjugated bilirubin from the blood. When jaundice, dark urine, and pale stools occur simultaneously, they form a classic clinical triad that strongly points to extrahepatic biliary obstruction, often requiring urgent imaging to identify the precise blockage site.
Unexplained Weight Loss and Metabolic Shifts
Involuntary weight loss exceeding 5% of body mass over six months, particularly when paired with reduced appetite, is a common feature of pancreatic malignancy. Tumors release cytokines and other metabolic byproducts that accelerate muscle breakdown and suppress hunger signals. Additionally, malabsorption from exocrine insufficiency deprives the body of essential calories and fat-soluble vitamins (A, D, E, and K), compounding nutritional deficits. New-onset diabetes or sudden worsening of previously stable glycemic control also frequently accompanies pancreatic disease, as tumor growth damages insulin-producing beta cells. Other systemic manifestations include unexplained fatigue, early satiety, nausea, vomiting, and occasionally, unprovoked deep vein thrombosis or blood clots. Abdominal pain that originates in the upper abdomen and radiates directly through to the mid-back is particularly characteristic, often worsening when lying flat and improving when leaning forward.
Diagnostic Pathways and Medical Evaluation
When clinical suspicion arises from persistent stool changes and associated symptoms, healthcare providers follow a structured diagnostic algorithm. Initial evaluation typically involves a comprehensive blood panel assessing liver function (ALT, AST, ALP, bilirubin), pancreatic enzymes (amylase and lipase), and tumor markers (CA 19-9, though not definitive for screening). Fecal elastase-1 testing is frequently ordered to objectively measure exocrine pancreatic function, with levels below 200 µg/g stool indicating moderate to severe insufficiency.
Imaging plays a pivotal role in visualizing the pancreas and surrounding biliary structures. Contrast-enhanced computed tomography (CT) of the abdomen remains the gold standard for detecting pancreatic masses, assessing tumor size, and evaluating local vascular involvement. Magnetic resonance imaging (MRI) with magnetic resonance cholangiopancreatography (MRCP) provides superior visualization of the bile and pancreatic ducts without ionizing radiation, making it ideal for mapping strictures or identifying small lesions. Endoscopic ultrasound (EUS) offers high-resolution imaging of the pancreatic parenchyma and allows for fine-needle aspiration biopsy during the same procedure, providing definitive histopathological confirmation. If bile duct obstruction is confirmed, endoscopic retrograde cholangiopancreatography (ERCP) can simultaneously diagnose the blockage and place a stent to restore bile flow, providing rapid symptom relief. Collaboration with gastroenterologists, oncologists, and surgical specialists ensures a multidisciplinary approach to diagnosis and management.
The Future of Non-Invasive Stool Screening
Traditional pancreatic cancer detection relies heavily on symptom presentation, which unfortunately often occurs at advanced stages due to the organ’s deep anatomical location. Emerging research is actively exploring stool-based biomarker screening as a revolutionary, non-invasive alternative, supported by ongoing NIH/NCI cancer screening initiatives. According to a 2022 study published in Biomolecules by Sammallahti and colleagues, oncogenomic alterations from pancreatic tumor-derived cells, cell-free nucleic acids, and extracellular vesicles can be reliably detected in fecal samples. The gastrointestinal tract continuously sheds cells and releases genetic material into the intestinal lumen, which travels through the colon and appears in stool. Researchers are currently analyzing chromosomal aberrations, driver gene mutations (such as KRAS, TP53, and CDKN2A), epigenetic modifications, and non-coding RNA profiles to develop highly sensitive stool screening panels.
Combining genomic markers with microbiome analysis represents the next frontier in early detection. Pancreatic tumors alter the composition of gut bacteria, creating unique microbial signatures that could complement DNA-based testing. Stool offers an exceptionally convenient, painless, and cost-effective sampling medium that patients can collect at home, potentially enabling routine screening for high-risk individuals. While these technologies remain in clinical validation phases and are not yet widely available for routine primary care use, they underscore the critical importance of stool monitoring in future oncology practice. As research advances, regular digestive tracking may transition from symptom response to proactive early warning, fundamentally changing survival trajectories for pancreatic disease.
Managing Symptoms and Nutritional Support
Whether stool changes stem from a confirmed diagnosis, suspected insufficiency, or a benign gastrointestinal condition, implementing practical dietary and lifestyle strategies can significantly improve comfort and digestive efficiency. Prescription pancreatic enzyme replacement therapy (PERT) is the cornerstone of medical management for exocrine insufficiency. These enteric-coated microspheres release lipase, amylase, and protease at the optimal pH in the small intestine, mimicking natural physiological secretion. Patients are instructed to take the full dose at the beginning of each meal, with half-doses for snacks, and to avoid crushing or chewing the capsules to protect the enteric coating.
Dietary adjustments further enhance symptom control. Emphasizing a moderate-fat diet (rather than severe restriction, which can worsen malnutrition) paired with lean proteins, complex carbohydrates, and abundant vegetables supports sustainable digestion. Small, frequent meals reduce the enzymatic load per sitting, preventing overwhelming the pancreas. Staying well-hydrated with water, electrolyte solutions, or herbal teas compensates for fluid losses from frequent or loose bowel movements. Tracking fiber intake carefully is essential, as both excessive insoluble fiber and severe deficiency can exacerbate digestive discomfort. Working with a registered dietitian specializing in oncology or gastroenterology ensures nutritional plans remain balanced, address fat-soluble vitamin deficiencies, and align with individual tolerance levels. Regular monitoring of weight, bowel patterns, and energy levels provides objective feedback to adjust treatment protocols before complications arise.
Frequently Asked Questions
What does pancreatic cancer poop look like?
Stool changes associated with pancreatic cancer typically include pale, clay-colored, or grayish stools due to bile duct blockage. The stool may also appear greasy, oily, or float in the toilet because of undigested fats. It often has an unusually strong, foul odor and can be larger or bulkier than normal due to fat malabsorption.
Can pale or greasy stools definitely indicate pancreatic cancer?
No. While pale, greasy, or floating stools can be a warning sign of pancreatic cancer, they are also common symptoms of several other conditions. Gallstones, chronic pancreatitis, celiac disease, Crohn’s disease, liver disorders, and certain medications can all cause similar stool changes. Medical evaluation is necessary for an accurate diagnosis.
How quickly do stool changes develop in pancreatic cancer?
Stool changes can develop gradually or appear suddenly depending on tumor growth and location. Tumors in the head of the pancreas near the common bile duct often cause noticeable changes earlier because they obstruct bile flow. In contrast, tumors in the body or tail may not cause visible stool changes until the disease is more advanced.
What tests are used to diagnose stool changes related to pancreatic issues?
Physicians typically order blood tests (like liver function panels, CA 19-9, and amylase/lipase levels), abdominal imaging (CT scans, MRI, or endoscopic ultrasound), and stool analysis (fecal elastase or fat quantification). If bile duct obstruction is suspected, ERCP or MRCP may be used for detailed visualization and therapeutic intervention.
How is steatorrhea managed if it is caused by pancreatic insufficiency?
Management usually involves prescription pancreatic enzyme replacement therapy (PERT) taken with meals and snacks. Patients are often advised to follow a balanced, moderate-fat diet, stay hydrated, and avoid heavy or highly processed fatty foods. Nutritional supplements and dietary counseling from a registered dietitian can significantly improve symptom control and quality of life.
Conclusion
Understanding the physiological and clinical dimensions of pancreatic cancer poop empowers individuals to monitor their digestive health proactively and recognize warning signs that demand medical attention. While stool changes such as paleness, greasiness, floating consistency, and foul odor can indicate serious underlying conditions, they also overlap with numerous manageable gastrointestinal disorders. Persistent alterations in bowel habits, especially when accompanied by jaundice, unexplained weight loss, back-radiating pain, or metabolic shifts, should never be ignored. Timely consultation with a healthcare provider facilitates accurate diagnostic testing, appropriate enzyme therapy, and specialized nutritional support. As research continues to pioneer stool-based genomic screening and refine non-invasive detection methods, digestive tracking will remain a vital tool in early intervention. Prioritizing symptom awareness, maintaining detailed health records, and seeking expert guidance remain the most effective strategies for safeguarding pancreatic and overall digestive health.

About the author
Fatima Al-Jamil, MD, MPH, is board-certified in gastroenterology and hepatology. She is an Assistant Professor of Medicine at a university in Michigan, with a clinical focus on inflammatory bowel disease (IBD) and motility disorders.