Hard Bump Inside Gum: Causes, Diagnosis & Evidence-Based Treatment

Noticing an unusual growth in your mouth can be unsettling, especially when you discover a hard bump inside gum tissue that was not there before. The oral cavity is highly sensitive, and any deviation from normal anatomy naturally raises concerns about dental health, infection, or more serious conditions. Understanding what causes these firm nodules, how clinicians differentiate between benign and pathological growths, and what treatment pathways are available can significantly reduce anxiety and empower you to make informed health decisions. A hard bump inside gum tissue can range from a harmless anatomical variation to a clinically significant lesion requiring professional intervention. Because the mouth serves as a critical entry point for the digestive and respiratory systems, maintaining its structural and microbial integrity is essential for overall systemic wellness. In this comprehensive guide, we will explore the medical science behind intraoral lumps, examine diagnostic protocols, review evidence-based treatment strategies, and provide actionable self-care recommendations to help you navigate this common oral health concern safely and effectively.
What Exactly Is a Hard Bump Inside the Gum?
The gingival tissues and underlying alveolar bone form a complex anatomical landscape that supports dentition and protects against microbial invasion. When a hard bump inside gum tissue appears, it typically originates from one of three primary sources: the mucosal lining, the connective tissue beneath the gingiva, or the alveolar bone itself. These growths vary in size, texture, mobility, and clinical behavior. Some are purely structural adaptations that develop over decades, while others represent acute inflammatory responses, cystic formations, or reactive tissue hyperplasia. The periodontium, consisting of the gingiva, periodontal ligament, cementum, and alveolar bone, responds dynamically to mechanical stress, microbial challenges, and healing processes. When a hard bump inside gum tissue becomes palpable, it often indicates localized cellular proliferation, mineralized tissue formation, or fluid accumulation within a defined capsule. Dental professionals categorize these lesions based on their histological origin, growth velocity, symptomatic presentation, and radiographic appearance. Recognizing the fundamental nature of these growths is the first step in determining whether observation, conservative management, or surgical intervention is warranted.
Common Medical Causes Behind a Hard Bump Inside Gum
Identifying the precise etiology requires understanding the spectrum of oral pathologies. The presence of a hard bump inside gum tissue can stem from genetic predispositions, developmental anomalies, localized trauma, chronic inflammation, or rare neoplastic processes. Below, we examine the most clinically prevalent causes, their pathophysiological mechanisms, and how they manifest in daily life.
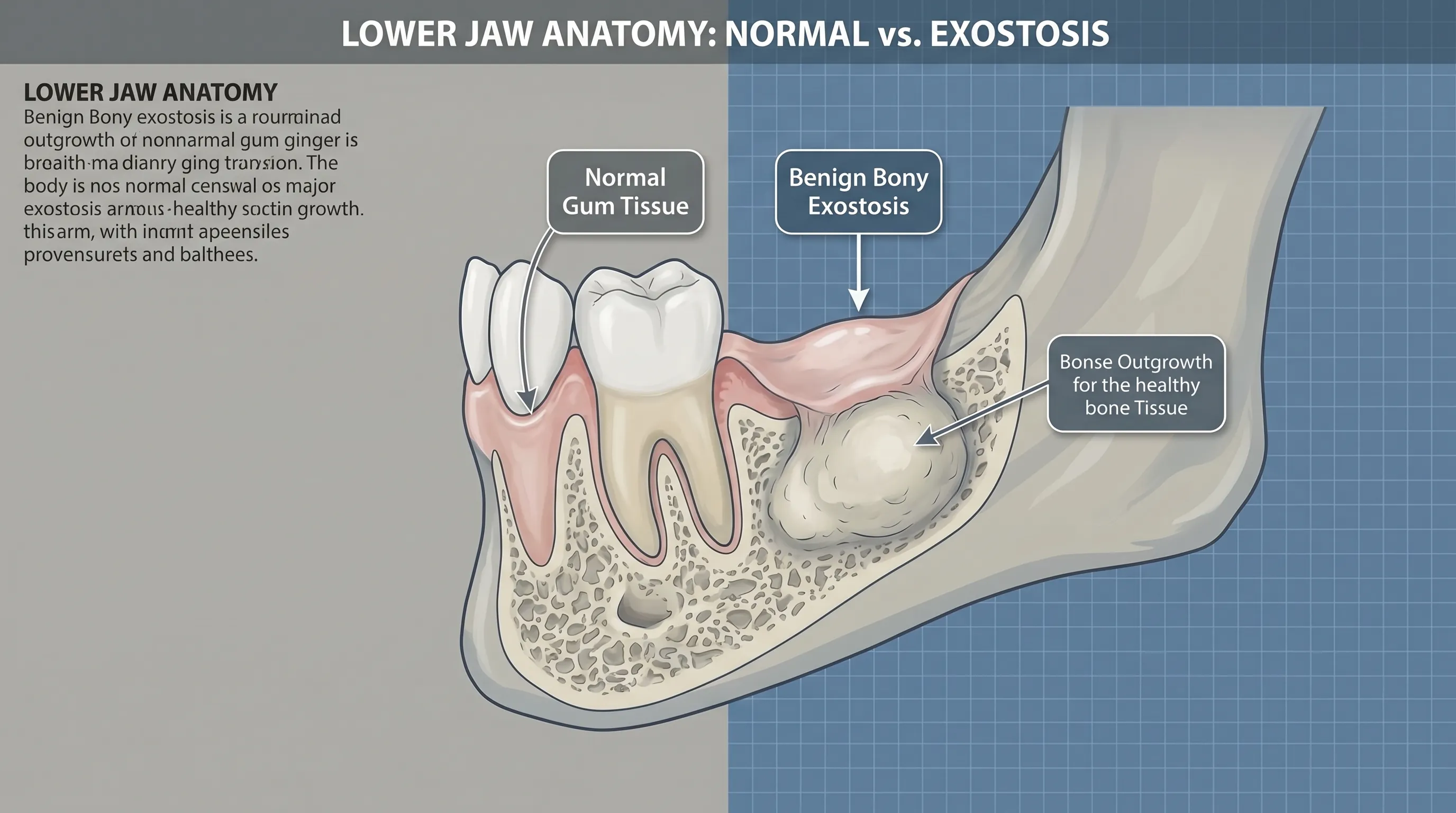
Torus Palatinus and Mandibular Exostosis
Torus palatinus is a benign, slow-growing bony protrusion located on the midline of the hard palate. Mandibular tori (exostosis) develop along the lingual surface of the lower jaw near the premolars. These structures are composed of dense cortical and trabecular bone covered by a thin, tightly adherent mucosal layer. They are considered anatomical variants rather than diseases, with prevalence rates ranging from ten to fifty percent across global populations depending on ethnic background. Genetics play a substantial role, as these growths frequently cluster within families. Environmental factors such as bruxism, heavy masticatory forces, and dietary texture may accelerate their development over time. Patients often remain asymptomatic unless the mucosal covering is ulcerated by hard foods, dental appliances, or aggressive brushing. When a torus is present, it may occasionally be mistaken for a hard bump inside gum tissue, particularly if located near the gingival margin. These growths rarely require treatment unless they interfere with denture fabrication, cause recurrent trauma, or impede surgical procedures. Radiographic evaluation confirms their bony density, distinguishing them clearly from soft tissue masses or cystic lesions.
Dental Abscesses and Localized Infections
A dental abscess forms when bacterial invasion reaches the pulp chamber or deep periodontal tissues, triggering an acute inflammatory cascade. The resulting accumulation of purulent exudate, necrotic debris, and immune cells can create a firm, often painful swelling that mimics a hard bump inside gum tissue. Periapical abscesses originate from untreated caries or cracked teeth, while periodontal abscesses arise from deep periodontal pockets harboring pathogenic biofilm. Clinically, these infections present with localized tenderness, throbbing pain, erythema, and sometimes purulent drainage. If left unmanaged, the pressure from the accumulating exudate may organize into a more consolidated, firm nodule. The body attempts to wall off the infection, leading to fibrous capsule formation that increases tissue density. Systemic symptoms such as low-grade fever, malaise, or cervical lymphadenopathy may accompany advanced cases. Prompt clinical intervention is essential, as untreated odontogenic infections can spread into fascial spaces, compromising airway patency or causing osteomyelitis. Comprehensive dental evaluation, source control, and targeted antimicrobial therapy resolve the majority of infection-related firm swellings.
Impacted Teeth and Healing Bone Spicules
Eruption anomalies frequently manifest as palpable irregularities along the alveolar ridge. Impacted third molars, supernumerary teeth, or odontomas can displace surrounding bone and soft tissue, creating a firm mass that feels like a hard bump inside gum tissue. Radiographic imaging typically reveals the unerupted structure beneath the gingiva, clarifying the diagnosis. Similarly, following surgical tooth extraction or alveoloplasty, patients may develop bone spicules during the remodeling phase. As the socket heals, small fragments of non-viable alveolar bone or calcified debris may migrate toward the surface. These spicules feel sharply firm and may temporarily pierce the mucosa, causing localized irritation. The natural shedding process typically resolves the issue within three to six weeks without surgical intervention. Maintaining meticulous oral hygiene and avoiding manual manipulation of the area prevents secondary infection and accelerates mucosal re-epithelialization. In persistent cases, a periodontist or oral surgeon can safely remove the spicule under local anesthesia, providing immediate relief and preventing chronic mucosal ulceration.
Fibromas, Mucoceles, and Soft Tissue Reactions
Reactive lesions account for a significant proportion of firm intraoral growths. Irritation fibromas develop from chronic friction, biting trauma, or poorly fitted prosthetics, stimulating localized fibroblast proliferation and collagen deposition. Though initially soft, they gradually firm up as connective tissue matures, presenting as smooth, dome-shaped, non-tender nodules. Mucoceles arise from blocked minor salivary gland ducts, typically on the lower lip or buccal mucosa, but occasionally near gingival margins. While classically fluctuant, older mucoceles may feel firmer due to fibrotic encapsulation and recurrent micro-trauma. Epulis fissuratum, or denture-induced hyperplasia, manifests as firm fibrous folds along the denture flange. These reactive conditions are fundamentally protective responses that become clinically problematic when they interfere with function, hygiene, or comfort. Conservative management involves eliminating the source of irritation, optimizing prosthetic fit, and adopting gentle tissue maintenance protocols. Surgical excision with histopathological confirmation remains the gold standard for definitive treatment when lesions persist, enlarge, or cause functional impairment.
Cysts, Granulomas, and Rare Malignancies
Odontogenic cysts and granulomas represent encapsulated pathological cavities that originate from dental developmental remnants or chronic inflammatory stimuli. Radicular cysts, periapical granulomas, and dentigerous cysts can expand within the alveolar bone, thinning the cortical plate and creating a palpable hard bump inside gum tissue. These lesions typically grow slowly and remain asymptomatic until they reach a clinically significant size. Advanced imaging distinguishes them from solid tumors by revealing well-defined radiolucent borders. Granulomatous conditions such as foreign body reactions or localized immune responses to root canal materials can also manifest as firm submucosal nodules. Although exceedingly rare, malignant processes including squamous cell carcinoma, salivary gland neoplasms, or metastatic lesions may present as indurated masses. These malignancies often exhibit rapid growth, tissue fixation, bleeding, ulceration, or neurological symptoms. Early referral to an oral and maxillofacial pathologist ensures accurate tissue characterization and appropriate staging. Vigilant monitoring and timely intervention dramatically improve prognostic outcomes across all cystic and neoplastic entities.
Recognizing Symptoms: When to Be Concerned
The clinical presentation of intraoral lumps varies widely based on etiology, duration, and patient-specific factors. Differentiating between benign adaptations and potentially serious conditions requires careful observation of morphological and symptomatic patterns.
Benign Versus Potentially Serious Characteristics
Benign growths such as tori, fibromas, and healing spicules typically demonstrate slow progression, symmetrical borders, and mobility or fixed attachment without tissue invasion. The overlying mucosa remains intact, normally colored, and resilient to gentle palpation. Discomfort is minimal unless subjected to mechanical trauma. Conversely, clinically suspicious lesions often exhibit irregular contours, rapid expansion, erythema or leukoplakia, spontaneous bleeding, ulceration that fails to heal within fourteen days, or paresthesia. A hard bump inside gum tissue that feels rock-hard, fixed to underlying structures, or accompanied by unexplained weight loss warrants immediate professional evaluation. Pain is not a reliable differentiator, as both acute infections and advanced malignancies can range from asymptomatic to severely painful depending on neural involvement and inflammatory mediators. Documenting changes in size, color, texture, and symptom severity over time provides invaluable data for clinical assessment.
Red Flags Requiring Immediate Professional Evaluation
Certain clinical signs necessitate prompt dental or medical intervention. Persistent swelling beyond two weeks, progressive enlargement, difficulty swallowing or speaking, trismus (reduced mouth opening), unexplained tooth mobility without periodontal disease, and cervical lymphadenopathy are critical warning indicators. Systemic symptoms such as fever, night sweats, or unexplained fatigue further elevate urgency. Patients with compromised immune systems, uncontrolled diabetes, or histories of tobacco and alcohol use face increased vulnerability to aggressive infections and malignant transformations. Delaying evaluation can allow localized pathology to progress into fascial space infections, osteomyelitis, or advanced neoplastic disease requiring complex multidisciplinary management. Establishing a baseline examination with a licensed dentist or periodontist ensures early detection and appropriate intervention pathways.

The Diagnostic Process and Clinical Evaluation
Accurate diagnosis relies on a systematic approach combining clinical observation, advanced imaging, and histopathological analysis. Dental professionals follow standardized protocols to characterize intraoral lesions and rule out serious pathology.
Physical Examination and Palpation Techniques
During the initial assessment, clinicians inspect the lesion under adequate lighting, evaluating color, surface texture, border definition, and relationship to adjacent dentition. Gentle bimanual palpation determines consistency, mobility, tenderness, and attachment to underlying bone or soft tissue. Measuring dimensions in millimeters and documenting anatomical landmarks establishes a clinical baseline. Periodontal probing assesses pocket depth, bleeding on probing, and furcation involvement if the lesion is gingiva-adjacent. Vitality testing of adjacent teeth helps differentiate pulpal pathologies from periodontal or osseous origins. Clinicians also evaluate occlusal patterns, parafunctional habits, and prosthetic contacts that may contribute to reactive tissue formation. This comprehensive physical evaluation guides subsequent diagnostic imaging and treatment planning.
Imaging Techniques and Biopsy Procedures
Radiographic evaluation is indispensable for characterizing bony lesions. Intraoral periapical X-rays, bitewing films, and panoramic radiographs reveal alveolar bone integrity, periapical pathology, impacted teeth, and cystic expansions. Cone-beam computed tomography (CBCT) provides three-dimensional visualization of lesion boundaries, bone resorption patterns, and proximity to vital structures like the inferior alveolar nerve or maxillary sinus. When imaging confirms a soft tissue mass or atypical presentation, an excisional or incisional biopsy is performed under local anesthesia. Tissue samples are preserved in formalin and analyzed by board-certified oral pathologists. Histological examination identifies cellular architecture, inflammatory infiltrates, keratinization patterns, and dysplasia. Molecular markers and immunohistochemical staining further refine diagnoses for ambiguous cases. This evidence-based diagnostic cascade ensures precise classification and guides appropriate therapeutic strategies.
Medical and Surgical Treatment Options
Management strategies are tailored to the underlying diagnosis, symptom severity, and functional impact. Treatment ranges from conservative monitoring to complex surgical reconstruction.
Conservative Management and Symptom Management
Many asymptomatic bony growths and stable fibromas require no active intervention. Patients are educated on gentle brushing techniques, avoidance of abrasive foods, and routine dental monitoring every six months. For mild irritation or post-inflammatory firmness, warm saline rinses two to three times daily promote tissue homeostasis. Nonsteroidal anti-inflammatory drugs provide temporary discomfort relief while healing progresses. Denture wearers undergo relining procedures to redistribute pressure away from reactive tissue zones. Conservative protocols are continuously evaluated for stability, with intervention escalated only if lesions demonstrate progressive enlargement, functional impairment, or malignant transformation risk. This watchful waiting approach prevents unnecessary surgery while preserving anatomical integrity.
Surgical Removal, Bone Contouring, and Oral Surgery
Surgical intervention becomes necessary when a hard bump inside gum tissue compromises oral function, causes recurrent ulceration, or exhibits atypical histology. Torus reduction, exostosis contouring, and lesion excision are performed under local anesthesia with sterile surgical techniques. Electrosurgery or diode lasers minimize bleeding and promote rapid mucosal healing. Alveoloplasty smooths irregular bone margins following extraction or spicule removal. Larger cystic enucleation requires careful dissection, complete capsule removal, and primary closure with resorbable sutures. Postoperative care includes prescribed antimicrobial mouth rinses, soft diet adherence for seven to ten days, and scheduled suture removal. Follow-up imaging confirms complete resolution and guides long-term monitoring. Advanced maxillofacial techniques ensure optimal aesthetic and functional outcomes while preserving vital anatomical structures.
Antibiotic Therapy and Infection Control Protocols
Odontogenic infections demand immediate antimicrobial management. Dentists prescribe targeted antibiotics based on clinical presentation, patient allergy history, and regional resistance patterns. Amoxicillin remains first-line for non-penicillin allergic patients, while clindamycin or azithromycin serves as alternatives. Adjunctive therapy includes professional debridement, root canal therapy, or extraction to eliminate the microbial reservoir. Chlorhexidine gluconate rinses reduce surface biofilm burden. Patients are instructed to maintain hydration, rest, and monitor for spreading infection. Severe cases may require incision and drainage procedures in conjunction with systemic therapy. Strict adherence to prescribed regimens prevents recurrence, resistance development, and systemic complications.
At-Home Care, Prevention, and Long-Term Management
Proactive oral health strategies significantly reduce the likelihood of developing problematic intraoral lesions and promote optimal tissue resilience.
Optimizing Daily Oral Hygiene Routines
Consistent mechanical plaque removal disrupts pathogenic biofilm formation and prevents periodontal inflammation. Use a soft-bristled toothbrush with fluoride toothpaste twice daily, angling the bristles at forty-five degrees to the gingival margin. Incorporate flossing or interdental brushes to clean proximal surfaces inaccessible to toothbrushes. Alcohol-free antimicrobial mouth rinses support microbial balance without causing mucosal desiccation. Replace toothbrushes every three months or after illness. Patients with orthodontic appliances or prostheses utilize specialized cleaning tools to prevent plaque accumulation near tissue margins. Regular professional cleanings remove calculus deposits and polish restorative surfaces, minimizing chronic irritation triggers.
Dietary Modifications and Lifestyle Adjustments
Nutritional choices directly influence oral tissue integrity and immune competence. Consume vitamin C-rich foods to support collagen synthesis and gingival capillary health. Adequate calcium and vitamin D intake maintains alveolar bone density and reduces exostosis progression risk. Limit refined carbohydrates and acidic beverages that accelerate enamel demineralization and alter salivary pH. Avoid excessively hard, crunchy, or sharp foods that traumatize delicate mucosal tissues. Eliminate tobacco products entirely, as they impair microcirculation, delay wound healing, and dramatically increase malignant transformation risk. Moderate alcohol consumption and maintain adequate hydration to preserve optimal salivary flow. These lifestyle modifications create a resilient oral ecosystem less susceptible to reactive and infectious pathologies.
Safe, Temporary Relief Strategies for Discomfort
While awaiting professional evaluation, several evidence-based home measures provide symptomatic relief. Warm saline rinses (half teaspoon salt in eight ounces warm water) reduce inflammation and cleanse the area. Cold compresses applied externally to the cheek for fifteen-minute intervals decrease localized swelling and nerve sensitivity. Over-the-counter topical oral anesthetics containing benzocaine provide temporary numbness, though prolonged use should be avoided to prevent tissue irritation. Avoid aspirin directly on the lesion to prevent chemical burns. Maintain soft food consistency to minimize masticatory stress. Document symptom progression daily and discontinue home care if redness, swelling, or systemic symptoms worsen. These supportive measures bridge the gap between symptom onset and definitive clinical management.
Potential Complications and Prognosis
The long-term outlook for a hard bump inside gum tissue depends entirely on accurate diagnosis and timely intervention. Benign lesions typically remain stable indefinitely, with excellent prognosis following minor surgical contouring if desired. Reactive fibromas and healing spicules resolve completely with appropriate tissue management and hygiene optimization. Odontogenic cysts carry favorable outcomes when enucleated completely, though recurrence is possible if residual epithelial lining remains. Infectious processes require comprehensive source elimination to prevent chronic osteomyelitis or systemic dissemination. Malignant lesions demand multidisciplinary oncology management, with early detection correlating directly with survival rates. Consistent adherence to professional monitoring schedules, prompt reporting of tissue changes, and proactive oral hygiene ensure optimal functional preservation and quality of life. Most patients experience complete resolution without lasting complications when care pathways are followed diligently.
| Feature | Benign Growth (Tori, Fibromas, Healing Spicules) | Infectious Lesion (Abscess, Granuloma) | Potentially Malignant Mass |
|---|---|---|---|
| Growth Rate | Slow (months to years) | Rapid (days to weeks) | Variable (often weeks to months) |
| Surface Texture | Smooth, intact mucosa | Inflamed, may exude pus | Irregular, ulcerated, leukoplakic |
| Pain Level | Typically asymptomatic | Moderate to severe, throbbing | Often painless early, becomes painful |
| Mobility/Fixation | Mobile or firmly attached | Fluctuant then firm | Fixed to underlying tissues |
| Recommended Action | Monitor, optimize hygiene, elective removal | Immediate dental care, source control, antibiotics | Urgent biopsy, specialist referral, staging |
Frequently Asked Questions
Can a hard bump inside the gum go away on its own?
It depends on the underlying cause. Benign bone growths like torus palatinus do not disappear spontaneously and often remain stable for years. Small healing bone spicules or minor traumatic fibromas may resolve within several weeks. However, persistent bumps, painful lumps, or those showing signs of infection typically require professional dental intervention.
Is a hard bump inside the gum a sign of oral cancer?
Most hard bumps inside the gum are benign. Oral cancer lesions typically present as non-healing ulcers, red or white patches, or irregular growths that bleed easily. While any persistent lump should be evaluated by a dentist, a painless, slow-growing hard bump is far more likely to be an exostosis, cyst, or reactive tissue rather than malignancy.
How is a hard bump inside the gum diagnosed?
Dentists diagnose the condition through a comprehensive oral examination, palpation of the tissue, and dental imaging such as panoramic X-rays or cone-beam computed tomography. If the lesion is atypical, a biopsy may be performed to analyze tissue samples under a microscope and rule out pathological conditions.
Does removing a hard bump inside the gum hurt?
Surgical removal is performed under local anesthesia, so patients do not feel pain during the procedure. Postoperative discomfort is typically mild to moderate and managed effectively with over-the-counter pain relievers, cold compresses, and proper wound care prescribed by the dental surgeon.
What causes a hard bump inside the gum after a tooth extraction?
Following an extraction, a hard bump is commonly a bone spicule (sequestrum), which is a small fragment of dead bone working its way through the gum as part of normal healing. Less commonly, it may be a healing socket irregularity, a localized hematoma, or an early-stage infection. Most spicules resolve naturally within weeks.
Key Takeaways
Recognizing a hard bump inside gum tissue can trigger understandable concern, but most intraoral nodules represent benign anatomical variations, reactive tissue formations, or predictable healing processes. Accurate diagnosis requires professional clinical evaluation, appropriate radiographic imaging, and sometimes histopathological analysis. Conservative management and meticulous oral hygiene suffice for asymptomatic lesions, while surgical intervention and targeted antimicrobial therapy address functional impairment and infection. Implementing preventive strategies, avoiding tissue trauma, and maintaining routine dental visits dramatically reduce complication risks. Always consult a licensed dental professional for personalized assessment, as early evaluation remains the most reliable pathway to optimal oral and systemic health outcomes.
For further clinical guidance, consult authoritative resources from the American Dental Association, Mayo Clinic Oral Health Center, and the Cleveland Clinic Dental Care Division. Patients seeking comprehensive anatomical and pathological education may also explore peer-reviewed literature through the National Institutes of Health and the Centers for Disease Control and Prevention Oral Health Portal. Maintaining proactive communication with your dental care team ensures timely intervention and long-term oral wellness.

About the author
Benjamin Carter, MD, is a board-certified otolaryngologist specializing in head and neck surgery, with an expertise in treating throat cancer. He is an associate professor and the residency program director at a medical school in North Carolina.