Receding Gums: Causes, Treatments, and Visual Reference Guide

Gingival recession represents one of the most prevalent yet frequently overlooked conditions in modern dental practice. Characterized by the apical migration of the gingival margin away from the crown, this progressive condition gradually exposes the underlying tooth root, creating vulnerable anatomical pathways for bacterial colonization and structural degradation. For patients attempting early self-diagnosis, reviewing clinical receding gums images provides a crucial visual baseline for understanding how healthy tissue margins should appear versus advanced pathological migration. The condition develops insidiously, often without overt pain during initial stages, which explains why nearly half of all adults remain unaware until root sensitivity or aesthetic concerns prompt clinical evaluation. Understanding the pathophysiology, recognizing early warning signs, and accessing evidence-based therapeutic interventions can effectively halt disease progression and restore periodontal stability.
The visual and tactile changes associated with gingival recession require professional contextualization, which is why high-quality receding gums images serve as essential educational tools for both patients and practitioners. These reference materials help demystify clinical terminology, illustrate varying degrees of tissue loss according to standardized classification systems, and empower individuals to make informed decisions about oral health management. By integrating authoritative clinical guidelines with practical self-monitoring strategies, patients can navigate the complex landscape of periodontal health with confidence and proactive precision.
Understanding Gingival Recession: Clinical Markers and Visual Identification
The human periodontium consists of highly specialized tissues including the gingiva, periodontal ligament, cementum, and alveolar bone. Each component functions synergistically to anchor teeth, distribute masticatory forces, and maintain a biological seal against oral pathogens. When this delicate equilibrium is disrupted, the gingival margin begins to migrate apically, exposing the cementoenamel junction and root surfaces. Visualizing receding gums images allows patients and clinicians to identify precise anatomical deviations, track progressive tissue loss, and determine appropriate intervention thresholds based on established staging criteria.
Visual Identification and Clinical Markers
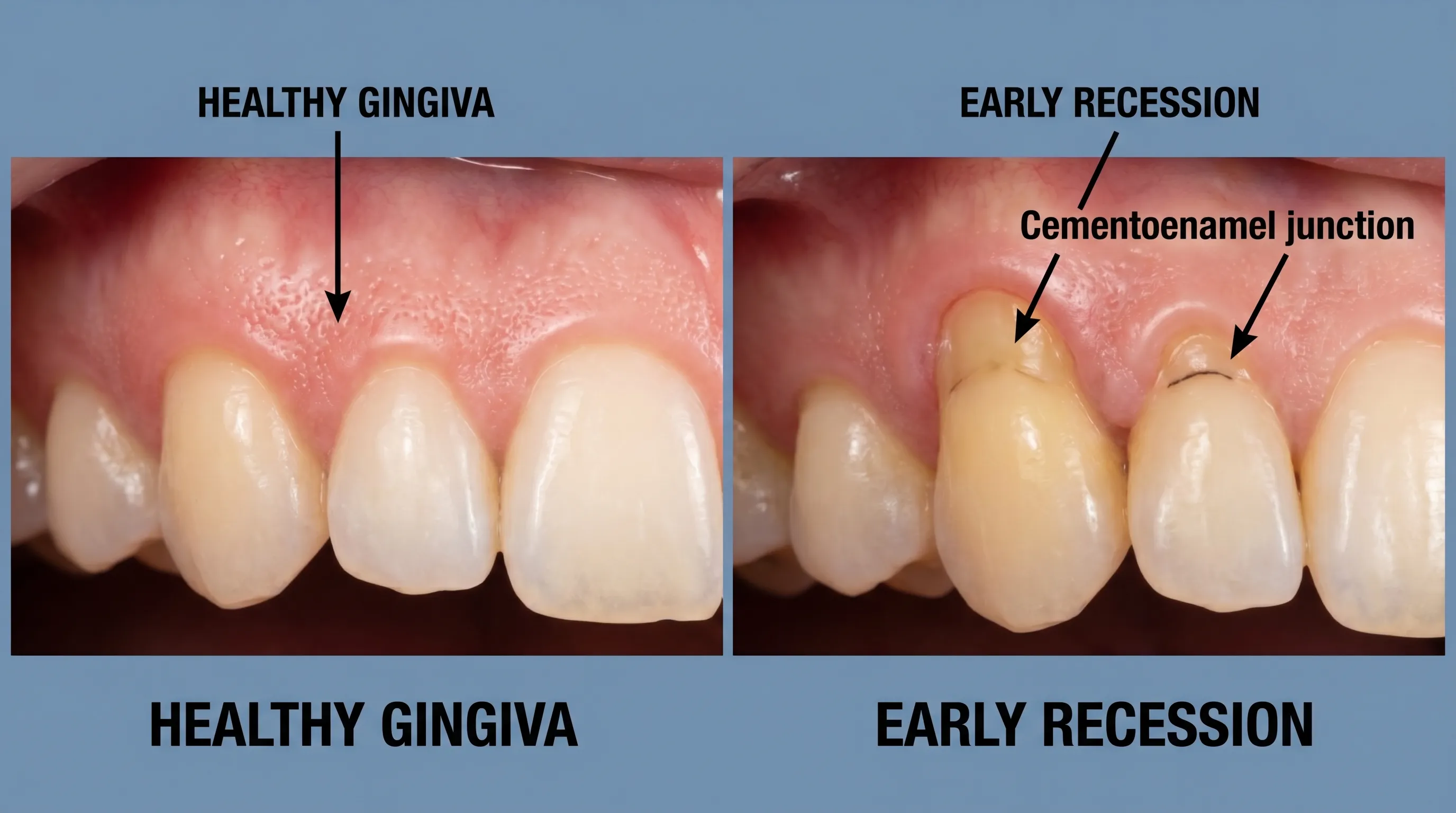
Early-stage gingival recession often manifests as subtle changes in gum contour rather than dramatic tissue loss. Patients may first notice increased tooth length, particularly on facial surfaces of anterior teeth and premolars. The gingival margin, which should normally rest approximately 1 to 2 millimeters coronal to the cementoenamel junction in healthy dentition, gradually shifts apically. As recession advances, the exposed root surface appears yellower than the enamel crown due to underlying dentin composition. Additionally, patients frequently report hypersensitivity to thermal, chemical, or tactile stimuli when dentinal tubules become exposed to the oral environment. Reviewing standardized receding gums images helps differentiate mild tissue migration from more severe pathological states requiring immediate therapeutic intervention.
Clinically, practitioners assess recession severity using the Miller Classification System, which categorizes tissue loss based on the extent of bone destruction and adjacent papilla preservation. Class I and II recessions involve marginal tissue loss that does not extend to the mucogingival junction, with intact interproximal bone and soft tissue, making them highly predictable for surgical correction. Class III and IV recessions present more complex anatomical challenges due to concurrent bone loss or papilla recession, which limits complete root coverage potential. Analyzing receding gums images within this framework provides objective staging metrics that guide prognosis and treatment selection.
The Role of Receding Gums Images in Self-Assessment
Self-monitoring oral health requires both tactile awareness and visual reference. When examining receding gums images in clinical literature or dental educational resources, patients can compare their own tissue architecture against documented progression patterns. Healthy gingiva exhibits a stippled, coral-pink appearance with firm consistency and knife-edge margins. Recession disrupts this presentation, creating smooth, flattened, or scalloped contours that follow the underlying bone architecture. Notch formations at the cervical tooth line, known as abfractions, frequently accompany recession and indicate chronic mechanical stress or occlusal trauma.
Photographic documentation becomes particularly valuable when tracking recession velocity over time. Consistent intraoral imaging under standardized lighting allows clinicians to measure marginal migration in millimeters across multiple appointments. For patients, reviewing comparative receding gums images during educational consultations clarifies why early intervention prevents irreversible attachment loss. Digital intraoral cameras and smartphone applications with calibrated measurement tools have revolutionized self-monitoring, though professional validation remains essential for accurate diagnosis.
Normal Gum Anatomy Versus Recession Patterns
Distinguishing between physiological gum contours and pathological recession requires understanding foundational periodontal architecture. The free gingiva forms a 0.5 to 2 millimeter sulcus around each tooth, creating a protective barrier against microbial invasion. The attached gingiva extends apically from the free gingival margin to the mucogingival junction, providing resilient tissue that withstands functional stress and orthodontic movement. When recession occurs, the mucogingival junction shifts coronally as tissue migrates apically, reducing the zone of attached gingiva and compromising periodontal stability.
Recession patterns vary significantly based on etiology. Brushing-induced trauma typically produces symmetrical, localized defects on highly visible facial surfaces. Periodontal disease-driven recession often presents with concurrent papillary blunting, erythema, bleeding on probing, and widespread pocket formation. Orthodontic or anatomical predisposition may cause asymmetrical migration following specific tooth root prominence. Studying receding gums images across these etiological categories enables precise differential diagnosis and targeted preventive strategies tailored to individual anatomical vulnerabilities.
Primary Causes and Underlying Risk Factors
Gingival recession rarely develops from a single isolated trigger. Instead, it emerges through complex interactions between microbial colonization, mechanical stress, genetic susceptibility, and systemic health status. Recognizing multifactorial etiology prevents oversimplified treatment approaches and ensures comprehensive management strategies address both immediate tissue loss and underlying predisposing conditions. Evidence consistently demonstrates that proactive risk factor modification significantly reduces recession incidence and progression velocity.
Periodontal Disease and Bacterial Accumulation
Chronic periodontitis represents the leading pathological driver of gingival recession worldwide. Dental plaque biofilm accumulates along the gingival margin, initiating inflammatory cascades that compromise connective tissue attachment and alveolar bone integrity. As bacterial metabolites penetrate periodontal tissues, macrophages and lymphocytes release matrix metalloproteinases and pro-inflammatory cytokines that degrade collagen fibers anchoring the gingiva to cementum. This attachment loss creates periodontal pockets, which deepen over time and facilitate further microbial colonization in a self-perpetuating pathological cycle.
NIDCR guidelines emphasize that dental plaque not removed daily hardens into calculus, which provides an ideal surface for pathogenic bacteria such as Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola. These microorganisms produce proteolytic enzymes that directly degrade periodontal ligaments and stimulate osteoclastic activity. When reviewing receding gums images associated with advanced periodontitis, clinicians typically observe widespread marginal tissue migration accompanied by purulent exudate, suppuration, and pronounced alveolar bone loss on radiographs. Effective biofilm disruption remains the cornerstone of preventing disease-driven recession.
Genetic Predisposition and Systemic Health
Approximately 30 percent of the population carries genetic variants that significantly increase susceptibility to periodontal breakdown, independent of oral hygiene practices. Polymorphisms in interleukin-1 genes alter inflammatory response thresholds, causing exaggerated tissue destruction in response to normal bacterial loads. This genetic predisposition explains why some individuals maintain meticulous oral care yet still develop progressive recession, while others tolerate suboptimal hygiene without significant attachment loss. Understanding this hereditary component validates the necessity of personalized monitoring protocols and frequent professional maintenance for genetically susceptible populations.
Systemic conditions further modulate periodontal health trajectories. Uncontrolled diabetes mellitus impairs neutrophil function and collagen synthesis, accelerating tissue breakdown and impairing wound healing. Hormonal fluctuations during puberty, pregnancy, and menopause increase vascular permeability and gingival inflammatory responses, temporarily heightening recession risk during these transitional periods. Autoimmune disorders, nutritional deficiencies in vitamin C and D, and chronic stress-mediated cortisol elevation similarly compromise periodontal tissue integrity. Comprehensive clinical evaluation must integrate medical history review when assessing receding gums images and determining intervention urgency.
Mechanical Trauma and Oral Habits
Physical forces exerted on teeth and gingiva play a substantial role in tissue migration patterns. Aggressive tooth brushing with hard-bristled implements generates abrasive trauma that gradually wears away both enamel and marginal gingiva. Horizontal scrubbing motions produce characteristic wedge-shaped cervical defects and localized recession on dominant brushing surfaces. Similarly, malocclusion and traumatic occlusal forces create excessive lateral pressure on periodontal ligaments, inducing bone remodeling that manifests as apical tissue migration. Bruxism, or chronic teeth grinding, amplifies these destructive forces during sleep, often accelerating recession velocity when combined with pre-existing attachment loss.
Oral piercings represent another frequently overlooked mechanical risk factor. Lip and tongue jewelry repeatedly contact facial and lingual gingiva during speech, mastication, and habitual manipulation. This chronic irritation induces localized ischemia, epithelial erosion, and progressive tissue recession around piercing sites. Tobacco use compounds mechanical damage by reducing gingival vascularity, impairing immune surveillance, and promoting thickened plaque accumulation that resists mechanical removal. Analyzing receding gums images through the lens of mechanical etiology clarifies why behavioral modification and occlusal stabilization are mandatory components of comprehensive recession management.
Clinical Diagnosis and Staging
Accurate diagnosis of gingival recession requires systematic evaluation beyond visual inspection. Practitioners employ standardized measurement protocols, radiographic imaging, and medical correlation to differentiate physiological variations from pathological tissue loss. Early intervention dramatically improves treatment predictability and long-term stability, making timely professional assessment essential when self-monitoring reveals suspicious anatomical changes.
Periodontal Probing and Pocket Depth Measurement
Periodontal probing remains the gold standard for quantifying recession severity and periodontal health status. Using a calibrated probe marked in millimeters, clinicians measure the distance from the gingival margin to the base of the periodontal pocket. Healthy gingiva exhibits probing depths between 1 and 3 millimeters without bleeding or discomfort. Depths measuring 4 millimeters or greater with bleeding on probing indicate active inflammation and attachment loss consistent with periodontal disease-driven recession.
Clinicians also measure recession depth separately by recording the distance from the cementoenamel junction to the current gingival margin. This measurement determines total attachment loss when combined with probing depth, providing a comprehensive picture of periodontal support compromise. Reviewing receding gums images alongside clinical charting data enables practitioners to track progression velocity, evaluate treatment efficacy, and adjust maintenance intervals accordingly. Consistent probing records establish objective baselines that prevent subjective assessment errors.
Radiographic Evaluation and Bone Loss Assessment
While soft tissue examination reveals marginal recession extent, underlying bone architecture requires radiographic documentation. Bitewing and periapical X-rays visualize alveolar crest height relative to cementoenamel junctions, identifying horizontal or vertical bone defects that accompany attachment loss. Cone-beam computed tomography provides three-dimensional visualization for complex cases involving root morphology anomalies, fenestrations, or dehiscences. Radiographic findings directly correlate with recession severity, as bone loss dictates the biological limits of tissue regeneration potential.
Dental radiographs also reveal secondary complications such as cervical caries on exposed root surfaces, pulpal calcification from chronic inflammation, and occlusal trauma indicators like widened periodontal ligament spaces. These imaging findings integrate with clinical recession measurements to formulate comprehensive treatment plans. Patients reviewing their own radiographs alongside receding gums images gain deeper understanding of subclinical disease progression and the rationale behind surgical intervention recommendations.
Differential Diagnosis and When to See a Specialist
Not all gingival migration constitutes pathological recession. Gingival enlargement from medications, systemic inflammation, or genetic overgrowth syndromes can create illusionary recession when tissue volume fluctuates. Orthodontic tooth movement, physiological aging, and post-extraction socket remodeling similarly alter gingival contours without indicating disease. Differential diagnosis requires distinguishing true attachment loss from positional variations, inflammatory swelling, or developmental anomalies.
Referral to a board-certified periodontist becomes necessary when recession progresses beyond Miller Class II, involves aesthetic zone teeth, coincides with severe mobility or mobility progression, or fails to respond to non-surgical therapy. Periodontists possess specialized training in mucogingival surgery, regenerative biology, and advanced occlusal management. Consulting a specialist ensures access to microsurgical techniques, predictable grafting protocols, and interdisciplinary coordination with orthodontists and prosthodontists when comprehensive rehabilitation is required. Analyzing complex receding gums images often necessitates this level of expertise for accurate staging and treatment sequencing.

Evidence-Based Treatment Pathways
Therapeutic intervention for gingival recession prioritizes disease stabilization, root surface protection, and aesthetic restoration when indicated. Treatment selection depends on recession classification, etiology, patient systemic health, and aesthetic demands. Both non-surgical and surgical modalities demonstrate strong clinical evidence for halting progression and restoring functional tissue architecture when appropriately indicated and meticulously executed.
Non-Surgical Interventions and Deep Cleaning Protocols
Initial management focuses on eliminating etiological factors and establishing optimal oral hygiene conditions. Scaling and root planing constitute the foundational non-surgical protocol, involving meticulous removal of subgingival plaque, calculus, and endotoxin-contaminated cementum. This procedure reduces bacterial load, eliminates chronic inflammation, and smooths exposed root surfaces to discourage plaque reattachment. Patients typically experience reduced bleeding, decreased pocket depths, and improved tissue firmness following thorough debridement.
Adjunctive antimicrobial therapy may accompany mechanical debridement when aggressive periodontopathogens persist. Localized delivery of minocycline microspheres or doxycycline gels targets residual bacteria within deep pockets, while systemic antibiotics reserve for rapidly progressing generalized disease. Chlorhexidine gluconate rinses provide short-term bacterial suppression during initial healing phases. Non-surgical management successfully halts mild to moderate recession progression when combined with behavioral modification and consistent maintenance. Monitoring post-therapy receding gums images demonstrates tissue stability and reduced inflammatory markers, confirming treatment efficacy.
Surgical Restoration and Tissue Grafting Techniques
When non-surgical therapy proves insufficient or recession compromises aesthetics, thermal sensitivity, or root integrity, surgical intervention becomes necessary. Connective tissue grafting represents the gold standard for root coverage, utilizing autogenous tissue harvested from the palatal vault and positioned over exposed roots. This technique provides predictable keratinized tissue regeneration, thickens biotype to resist future recession, and covers sensitive dentin surfaces effectively. Free gingival grafts similarly augment keratinized tissue zones but primarily address functional stability rather than complete root coverage.
Guided tissue regeneration procedures incorporate barrier membranes, bone graft materials, or enamel matrix derivatives to stimulate natural periodontal reconstruction. These techniques prove particularly valuable when concurrent bone loss requires structural restoration before soft tissue coverage. Surgical outcomes depend heavily on proper wound management, suturing precision, and patient compliance with postoperative restrictions. Successful surgical intervention transforms clinical appearance, as documented in comparative receding gums images showing preoperative tissue loss versus postoperative root coverage and margin stabilization.
Minimally Invasive Procedures and Recovery Expectations
The pinhole surgical technique represents a revolutionary advancement in periodontal surgery, eliminating traditional flap elevation and palatal harvesting. Through a small needle-created portal, specialized instruments loosen existing gingiva, allowing clinicians to coronally reposition tissue over exposed roots. Collagen strips stabilize the repositioned tissue during initial healing, while minimal incision size reduces postoperative discomfort and accelerates recovery. Patients typically resume normal activities within 48 hours, with final aesthetic stabilization occurring over three to six months.
Recovery protocols emphasize gentle oral hygiene, antimicrobial rinses, soft dietary modifications, and temporary occlusal protection when bruxism contributes to etiology. Follow-up appointments at one, three, and six months monitor tissue integration, vascularization, and pocket reduction. Evaluating sequential receding gums images during recovery validates healing progression and identifies areas requiring secondary refinement. Minimally invasive approaches continue evolving, expanding treatment accessibility while maintaining predictable long-term stability.
Prevention Strategies and Daily Oral Care Routines
Preventing gingival recession requires sustained behavioral commitment, mechanical technique refinement, and professional monitoring integration. While genetic predisposition influences baseline susceptibility, consistent preventive practices dramatically reduce progression velocity and treatment necessity. Implementing evidence-based daily protocols creates a resilient periodontal environment resistant to inflammatory and mechanical breakdown.
Proper Brushing and Flossing Techniques
Brushing methodology directly impacts gingival margin stability. Patients must utilize extra-soft or soft-bristled brushes with rounded filament tips to minimize abrasion potential. The modified Bass technique positions bristles at a 45-degree angle to the gingival margin, allowing gentle vibratory motions that disrupt subgingival plaque without tissue trauma. Horizontal scrubbing generates destructive shear forces that accelerate recession and create cervical notching. Electric toothbrushes with pressure sensors provide real-time feedback when excessive force compromises tissue integrity.
Interdental cleaning removes plaque from embrasure spaces that toothbrushes cannot access. Traditional floss, interdental brushes, or water flossers should be used daily, selecting devices that fit comfortably without forcing tissue trauma. Water flossers demonstrate particular efficacy for patients with existing recession, orthodontic appliances, or compromised manual dexterity. Consistent biofilm disruption prevents the inflammatory cascades that initiate attachment loss, preserving gingival architecture over decades.
Lifestyle Modifications and Risk Reduction
Dietary patterns significantly influence periodontal tissue resilience. Diets rich in antioxidants, omega-3 fatty acids, and vitamin C support collagen synthesis and modulate inflammatory responses. Conversely, high-sugar and refined carbohydrate diets fuel pathogenic bacterial proliferation while increasing systemic oxidative stress. Tobacco cessation remains the single most impactful lifestyle intervention for recession prevention, as smoking compromises vascular perfusion, impairs immune function, and accelerates tissue breakdown. Patients reviewing receding gums images from long-term smokers versus non-smokers frequently observe stark differences in tissue quality and recession velocity.
Stress management directly impacts periodontal health through cortisol-mediated immune suppression and bruxism exacerbation. Mindfulness practices, cognitive behavioral therapy, and regular physical activity reduce physiological stress responses that contribute to tissue degradation. Custom-fitted night guards protect against occlusal trauma and grinding forces that mechanically compromise gingival attachment. Integrating these lifestyle interventions with clinical care creates comprehensive protection against recession initiation and progression.
Professional Monitoring and Maintenance Schedules
Preventive oral health extends beyond daily routines to include structured professional maintenance. Patients with existing recession or high susceptibility require periodontal maintenance visits every three to four months rather than standard six-month intervals. These appointments include comprehensive pocket reassessment, radiographic monitoring when indicated, professional biofilm removal from recessed areas, and technique reinforcement. Early detection of marginal migration allows non-surgical intervention before surgical correction becomes necessary.
Maintenance protocols also address secondary caries prevention on exposed roots through fluoride varnish applications, desensitizing agents, and remineralizing therapies. Regular charting creates longitudinal data that reveals progression patterns invisible during isolated examinations. When patients understand that recession is progressive but highly manageable, compliance with maintenance schedules increases substantially. Tracking receding gums images during routine visits provides visual reinforcement of treatment stability and preventive success.
| Treatment Category | Procedure Type | Indication | Predictability | Recovery Duration |
|---|---|---|---|---|
| Non-Surgical | Scaling and Root Planing | Mild recession, pocket depth ≤4mm | High for disease stabilization | 1-2 weeks |
| Non-Surgical | Local/Topical Antibiotics | Adjunctive bacterial reduction | Moderate enhancement of cleaning outcomes | 3-5 days |
| Surgical | Connective Tissue Graft | Moderate-severe recession, aesthetic demands | 80-95% root coverage | 4-6 weeks healing |
| Surgical | Pinhole Technique | Mild-moderate recession, patient preference | 75-90% coverage | 2-3 days initial |
| Surgical | Guided Tissue Regeneration | Concurrent bone loss, deep defects | 70-85% structural restoration | 6-8 weeks |
Visual Progression and Photographic Documentation
Photographic documentation serves dual purposes in periodontal care: clinical assessment accuracy and patient education enhancement. Standardized intraoral photography captures precise tissue margins, color variations, and architectural changes that facilitate objective treatment planning. When patients understand how their condition compares to documented receding gums images, compliance improves and anxiety decreases through demystification of clinical processes.
How Dentists Use Receding Gums Images for Treatment Planning
Periodontists and general dentists utilize calibrated photography software to measure recession depth, calculate attachment loss percentages, and simulate surgical outcomes. Digital overlays allow practitioners to compare current tissue architecture against baseline photographs taken during previous visits, identifying subtle migration that tactile examination alone might miss. These visual records integrate with periodontal charts to create comprehensive diagnostic narratives that guide intervention selection.
Treatment simulations often incorporate digital smile design software, projecting post-surgical outcomes based on existing tissue parameters. Patients reviewing projected receding gums images alongside actual clinical photographs gain realistic expectations regarding coverage potential, healing timelines, and aesthetic improvements. This transparency fosters informed consent and reduces postoperative dissatisfaction when results align with documented clinical realities.
Tracking Your Own Gum Health Over Time
Personal health documentation empowers patients to participate actively in periodontal management. Smartphone cameras equipped with macro capabilities can capture intraoral changes when combined with cheek retractors and adequate lighting. Consistent monthly documentation under identical conditions reveals progression velocity that annual dental visits might overlook. Comparing personal photographs with authoritative receding gums images helps patients recognize warning signs requiring immediate professional consultation.
Digital tracking applications increasingly incorporate artificial intelligence algorithms that estimate recession severity from uploaded photographs. While these tools cannot replace clinical diagnosis, they provide valuable screening alerts when tissue migration accelerates. Maintaining organized photographic archives enables practitioners to visualize disease trajectories during consultations, facilitating more accurate prognostic assessments and personalized maintenance recommendations.
Misinterpretations and Common Visual Pitfalls
Self-diagnosis based solely on receding gums images carries inherent limitations. Lighting variations, camera angles, tissue inflammation, and temporary gingival swelling can create optical illusions that mimic recession or mask actual tissue loss. Erythematous gums from recent brushing trauma may appear recessed due to edema-induced margin displacement, while naturally thin gingival biotypes may appear healthy despite minimal attachment reserve. Clinical probing and radiographic correlation remain mandatory for accurate staging.
Patients frequently mistake gingival papilla recession for marginal recession, or confuse physiological black triangles with pathological attachment loss. Orthodontic relapse, occlusal trauma, and post-inflammatory shrinkage similarly alter tissue contours without indicating progressive disease. Consulting a dental professional ensures photographic observations translate into accurate diagnoses rather than unnecessary anxiety. Educational receding gums images must always contextualize within comprehensive clinical evaluation to maintain diagnostic integrity.
Frequently Asked Questions
Can receding gums grow back naturally without surgery?
Once gum tissue has receded, it does not naturally regenerate or grow back on its own. The exposed root surface and lost connective tissue attachment require professional intervention. However, non-surgical treatments like scaling and root planing can halt progression, and surgical procedures like soft tissue grafting or the pinhole surgical technique can effectively restore coverage.
How do I distinguish between gum recession and normal aging?
While minor tissue changes can occur with age, true recession involves measurable pocket depths exceeding 3 millimeters, visible root exposure, and often accompanies tooth sensitivity or notching near the gumline. Comparing your oral condition with clinical receding gums images can help identify abnormal tissue migration versus natural anatomical variations.
Does aggressive brushing permanently damage gums?
Yes, using a hard-bristled brush or applying excessive horizontal force can cause mechanical trauma that wears away both enamel and gingival tissue. This condition, known as abrasion-induced recession, creates V-shaped notches and accelerates tissue loss. Switching to a soft-bristled brush and using gentle circular motions typically prevents further damage.
Are dental implants a better alternative to gum grafting?
Dental implants replace entire lost teeth but do not treat recession. Gum grafting specifically addresses tissue loss around existing natural teeth. If recession progresses to severe bone loss and tooth loss occurs, an implant may eventually be needed, but preserving your natural teeth through periodontal therapy is always the clinical priority.
How long does recovery take after pinhole surgical technique?
Recovery from the pinhole surgical technique is typically rapid due to its minimally invasive nature. Most patients experience mild swelling for 24 to 48 hours and can return to normal eating and speaking within two to three days. Complete tissue stabilization and final aesthetic results usually manifest within three to six months.
Conclusion
Gingival recession represents a manageable yet progressive condition that demands proactive clinical attention, precise visual assessment, and sustained preventive commitment. Understanding the multifactorial etiology behind tissue migration enables patients and practitioners to implement targeted interventions that halt attachment loss, protect exposed roots, and restore functional architecture. Evidence-based therapies ranging from deep debridement protocols to advanced microsurgical grafting offer predictable outcomes when matched to appropriate clinical staging. Reviewing authoritative receding gums images throughout the treatment journey demystifies pathological progression, reinforces preventive behaviors, and validates therapeutic success. Prioritizing gentle oral hygiene techniques, consistent professional maintenance, and timely specialist consultation ensures long-term periodontal stability. Early recognition remains the most powerful predictor of favorable outcomes, making routine self-monitoring and clinical evaluation indispensable components of comprehensive dental health.
For authoritative guidance on periodontal disease management and prevention strategies, consult resources from the National Institute of Dental and Craniofacial Research and explore comprehensive patient education materials provided by WebMD's Oral Health Guide. Maintaining optimal periodontal health requires integrating clinical expertise with daily preventive practices, ensuring lasting structural integrity and functional comfort throughout your lifespan.

About the author
Benjamin Carter, MD, is a board-certified otolaryngologist specializing in head and neck surgery, with an expertise in treating throat cancer. He is an associate professor and the residency program director at a medical school in North Carolina.