Diverting Loop Ileostomy: A Complete Guide to Surgery and Recovery

Key points
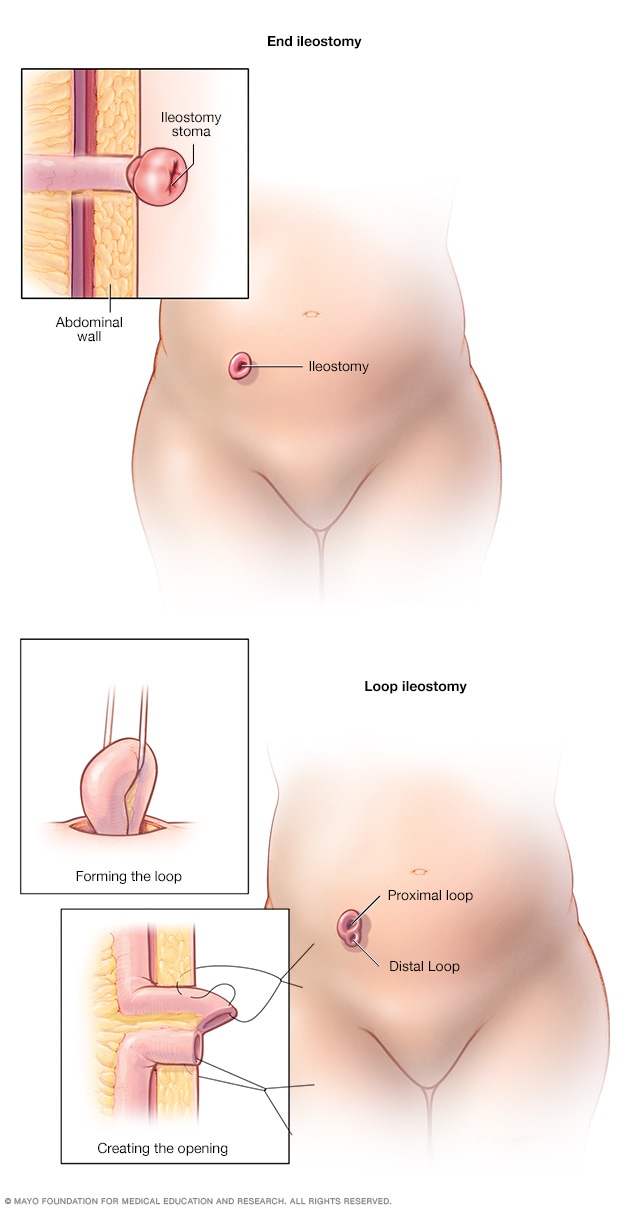
- The Proximal Opening: This is the "active" opening connected to the functioning part of the small intestine. It's where digestive waste (stool) exits the body into an external ostomy pouch.
- The Distal Opening: This "inactive" opening is connected to the resting part of the bowel (the colon and rectum). It only passes a small amount of mucus. This mucus is produced by the goblet cells lining the defunctionalized colon and is completely normal, though it may occasionally cause minor spotting in the pouch.
A diverting loop ileostomy is a surgical procedure that can be a critical step in treating conditions like rectal cancer, inflammatory bowel disease (IBD), and diverticulitis. While the thought of an ostomy can be daunting, understanding the procedure, its purpose, and what to expect during recovery can empower patients and their families. Modern advancements in surgical techniques, enhanced recovery protocols, and specialized ostomy nursing have transformed the patient experience, shifting the focus from mere survival to maintaining an active, high-quality life during the temporary diversion period.
This comprehensive guide synthesizes information from leading medical institutions and recent clinical research to provide a clear, in-depth look at every aspect of a diverting loop ileostomy, from the operating room to daily life. By integrating evidence-based clinical pathways with practical patient-centered strategies, this resource aims to demystify the journey and provide actionable insights for every stage of care.
What is a Diverting Loop Ileostomy?
A diverting loop ileostomy is a surgical procedure that creates a temporary opening, called a stoma, on the abdomen to allow stool to exit the body, bypassing the lower parts of the digestive tract. This physiological rerouting is a deliberate surgical strategy designed to protect vulnerable downstream tissue while preserving the anatomical continuity of the gastrointestinal tract for future restoration.
During the surgery, a loop of the small intestine (specifically, the final section known as the ileum) is brought through an incision in the abdominal wall. The surgeon then makes a cut in this loop and stitches it to the skin, creating a single stoma that has two distinct openings:
- The Proximal Opening: This is the "active" opening connected to the functioning part of the small intestine. It's where digestive waste (stool) exits the body into an external ostomy pouch.
- The Distal Opening: This "inactive" opening is connected to the resting part of the bowel (the colon and rectum). It only passes a small amount of mucus. This mucus is produced by the goblet cells lining the defunctionalized colon and is completely normal, though it may occasionally cause minor spotting in the pouch.
The primary goal of this procedure is to "divert" the fecal stream, giving a downstream surgical connection (anastomosis) or a diseased section of the bowel time to heal without being irritated by waste. As noted by NHS inform, this procedure is almost always intended to be temporary and is later reversed. Understanding the functional anatomy of the ileum is essential: the ileum normally absorbs bile salts, vitamin B12, and remaining nutrients, making its externalization a significant physiological shift that requires careful dietary and fluid management.
The term "loop" refers specifically to the anatomical technique used to exteriorize the bowel. Instead of cutting the intestine completely, the surgeon folds a segment into a U-shape, brings it to the surface, and creates an opening along the antimesenteric border. Historically, a soft plastic or silicone bridge (often called a supporting rod) was placed beneath the loop to prevent it from slipping back into the abdominal cavity during the initial healing phase. Modern surgical techniques often utilize a subcutaneous fascial fixation or internal suturing that eliminates the need for an external rod, thereby improving patient comfort and reducing peristomal skin irritation. When rods are used, they are typically removed at the bedside 7 to 14 days postoperatively, a process that is generally well-tolerated.
Physiologically, the stoma is highly vascularized and should appear pink to red, similar to the mucous membrane inside the mouth. It lacks nerve endings, so touching or cleaning the stoma itself is painless. Over the first 4 to 8 weeks post-operation, the stoma will naturally shrink and mature, changing from a swollen, protruding shape to a more stable, permanent form. Patients are advised to measure their stoma with each pouch change during this maturation phase, as even a 1-2 millimeter reduction in diameter requires adjusting the wafer cut size to maintain a secure seal. Because the colon is bypassed, stool output from a loop ileostomy is typically liquid to pasty, rich in digestive enzymes, and produced more frequently than colonic output. Understanding these baseline characteristics is crucial for successful ostomy management and early complication recognition.
 (Image Source: Mayo Clinic)
(Image Source: Mayo Clinic)
Why is a Diverting Loop Ileostomy Performed?
Surgeons recommend a diverting loop ileostomy in several clinical scenarios, primarily to protect the bowel and reduce the risk of severe complications. According to a review in the Clinics in Colon and Rectal Surgery, fecal diversion is an essential tool for managing complex colorectal conditions. The decision to divert is rarely arbitrary; it stems from a careful risk-benefit analysis weighing the morbidity of stoma creation and eventual reversal against the potentially life-threatening consequences of an unprotected anastomosis.
Key indications include:
- Protecting a New Surgical Anastomosis: This is the most common reason. After a surgeon removes a section of the colon or rectum (e.g., for rectal cancer) and reconnects the two ends, a temporary ileostomy protects this delicate connection from the fecal stream, reducing the consequences of a potential leak. Anastomotic leaks remain one of the most feared complications in colorectal surgery, with mortality and morbidity rates that can significantly impact long-term outcomes. By diverting stool, surgeons effectively create a low-pressure, clean environment that allows microvascular healing to occur undisturbed. Studies consistently show that while diversion does not necessarily prevent a leak, it dramatically mitigates the clinical severity of one, often converting a catastrophic pelvic sepsis event into a manageable, contained process.
- Inflammatory Bowel Disease (IBD): In severe cases of Crohn's disease or ulcerative colitis, an ileostomy allows the inflamed colon and rectum to rest and heal. This is particularly common in patients with medically refractory ulcerative colitis who are staged for a proctocolectomy with ileal pouch-anal anastomosis (IPAA). The loop ileostomy serves as a bridge, permitting the newly constructed J-pouch to mature without exposure to fecal bacteria, which could otherwise cause devastating pouchitis or pelvic sepsis. For Crohn's patients, diversion can also serve as a diagnostic or therapeutic trial to assess symptom improvement and guide long-term biologic therapy.
- Complicated Diverticulitis: For patients with perforated diverticulitis and significant infection (Hinchey III or IV classifications), a surgeon may perform a bowel resection and create a diverting ileostomy to allow the infection and inflammation to resolve before restoring bowel continuity. In the setting of severe peritonitis or hemodynamic instability, primary anastomosis is often deemed unsafe. Diversion in these emergency scenarios buys critical time for broad-spectrum antibiotic efficacy, source control, and hemodynamic stabilization.
- Bowel Obstruction: It can be used as a temporary measure to decompress the bowel in cases of a malignant obstruction. When a tumor completely blocks the large bowel, a loop ileostomy provides rapid decompression, relieves life-threatening symptoms, and allows for nutritional optimization and staging workup before definitive oncologic resection. This bridge-to-surgery approach prevents emergent colectomies under suboptimal conditions.
- Severe Perianal Crohn's Disease: When perianal disease is severe and uncontrolled, diversion can provide symptomatic relief and allow the area to heal. By eliminating the passage of stool through the perineum, complex fistulas and abscesses have a significantly higher chance of responding to medical therapy or surgical drainage. This is especially valuable when seton placement and biologic therapy have failed to achieve remission.
Beyond these primary indications, diversion may also be strategically utilized in cases of severe pelvic radiation damage, complex colorectal trauma, or congenital anorectal malformations in neonates. The decision is heavily weighted by the patient's overall physiological reserve, nutritional status, and the anticipated healing capacity of the pelvic tissues. Multidisciplinary tumor boards and colorectal surgical conferences routinely review these cases to standardize decision-making and align surgical strategies with oncologic timelines and patient quality-of-life goals.
The Surgical Procedure: What to Expect
An ileostomy is considered major surgery, and preparation is key to a smooth recovery. Understanding the perioperative workflow helps reduce anxiety and ensures patients are active participants in their own care pathways.
Preparing for Surgery
Before the operation, your surgical team will conduct a thorough assessment. A specialized Wound Ostomy Continence (WOC) nurse will meet with you to discuss life with a stoma and help mark the ideal location for it on your abdomen—a spot that is flat, visible, and away from skin folds or your beltline. This preoperative stoma siting is a critical evidence-based practice that has been shown to drastically reduce postoperative pouching complications. The marking process involves evaluating the abdomen in multiple positions (sitting, standing, supine, and bending) to account for skin creases, scars from prior surgeries, and the patient's dominant hand. Patients should bring comfortable clothing to this appointment to ensure the mark accommodates everyday wear. You will also receive instructions on bowel preparation, which may range from mechanical cleansing to a simple low-residue diet, depending on institutional protocols and whether concurrent colorectal resection is planned. Additionally, Enhanced Recovery After Surgery (ERAS) protocols are increasingly utilized, incorporating carbohydrate loading up to two hours before anesthesia to reduce postoperative insulin resistance and accelerate gut recovery. Patients on blood thinners or immunosuppressants will receive specific tapering instructions, and prehabilitation programs focusing on light cardiovascular exercise and protein optimization may be recommended to improve surgical resilience.
During the Surgery
The procedure is performed under general anesthesia. It can be done in two ways:
- Open Surgery: Involves one long incision down the abdomen. This approach is often reserved for emergency cases, patients with dense adhesions from multiple prior abdominal surgeries, or when concurrent extensive pelvic dissection is required. Open techniques provide direct tactile feedback to the surgeon, which can be crucial in anatomically complex or heavily scarred pelvic cavities.
- Laparoscopic (Minimally Invasive) Surgery: Uses several small incisions and a camera to perform the procedure. This approach often leads to a faster recovery, reduced postoperative pain, and lower rates of surgical site infections. In many high-volume centers, robotic-assisted platforms are now utilized for enhanced precision, particularly when navigating deep pelvic anatomy or when the ileostomy is being created alongside an ultra-low rectal resection. Regardless of the approach, many surgeons now employ near-infrared fluorescence angiography using indocyanine green (ICG) to visually confirm optimal blood flow to both the stoma segment and the planned anastomotic site, significantly reducing the risk of ischemic complications.
The surgeon creates the stoma as described above, sometimes using a small plastic rod to support the loop of intestine on the outside of the abdomen for the first week. The mesentery (the vascular tissue supplying blood to the intestine) is carefully dissected to ensure the loop reaches the abdominal wall without tension, as ischemic injury is a primary cause of early stoma necrosis. The bowel is then sutured to the dermal layer using absorbable sutures in a mucocutaneous technique that promotes rapid epithelialization. Throughout the procedure, the surgical team continuously monitors stoma perfusion, ensuring a robust arterial supply and adequate venous drainage. The surgical field is irrigated thoroughly, and temporary closure devices or drains may be placed depending on the extent of pelvic dissection.
How Long is Recovery?
As highlighted by Cleveland Clinic, recovery from an ileostomy takes about six to eight weeks. Your initial hospital stay will likely be between 3 and 10 days, where your healthcare team will monitor you closely and teach you the essentials of stoma care. Pain management is typically multimodal, utilizing acetaminophen, NSAIDs, and localized nerve blocks (like TAP blocks) to minimize opioid dependence, which can otherwise paralyze bowel motility. Early ambulation is strongly encouraged on postoperative day one to prevent venous thromboembolism and stimulate gastrointestinal function. The return of bowel sounds and the onset of high-volume stoma output are positive signs that the ileus is resolving. Dietary advancement follows a structured pathway, beginning with ice chips and clear liquids, progressing to full liquids, then a soft low-residue diet, and eventually transitioning to a regular diet as tolerated. Throughout this period, fluid and electrolyte balance is meticulously tracked, with intravenous hydration continued until oral intake is sufficient to match stoma losses. Patients are also taught pouch emptying and changing techniques before discharge, with many hospitals offering a simulated "mock change" session to build confidence.
Recovery and Life with a Loop Ileostomy
Adjusting to life with a stoma takes time and patience, but most people return to their normal activities. The psychological adjustment period, often referred to as "stoma shock," is a normal response to a significant body image change and lifestyle disruption. Multidisciplinary support, including counseling and peer mentorship programs, has been shown to significantly improve long-term quality of life metrics. Patients are encouraged to join support groups, whether hospital-facilitated or through reputable national organizations, to share experiences and learn coping strategies from those who have successfully navigated the same journey.
Caring for Your Stoma at Home
A WOC nurse is an invaluable resource during your recovery. You will learn how to manage your pouching system, which consists of a skin barrier (wafer) that sticks to your skin and a collection pouch that attaches to it. Modern ostomy supplies are highly sophisticated, featuring hydrocolloid and hydrofiber barriers that absorb moisture, odor-neutralizing layers, and charcoal filters to vent gas discreetly. Selecting the right system depends on stoma shape (round, oval, or irregular), abdominal contour (flat, concave, or convex), and skin sensitivity.
- Emptying the Pouch: The pouch should be emptied into the toilet when it is one-third to one-half full, typically 4 to 8 times a day. Allowing the pouch to overfill increases weight on the skin barrier, which can lead to premature detachment and skin breakdown. Most patients find that using a specialized pouching clip or built-in clamp ensures a leak-proof seal after emptying. To maintain hygiene and reduce splash, placing a few squares of toilet paper in the bowl before emptying can minimize mess, and wiping the spout thoroughly afterward prevents residue accumulation.
- Changing the System: The entire system (wafer and pouch) is usually changed about twice a week. Changing too frequently can cause mechanical skin trauma, while waiting too long risks adhesive degradation and leakage. The process involves gently removing the old barrier using an adhesive remover spray or wipe, cleaning the peristomal skin with warm water and a soft cloth (avoiding oily or alcohol-based wipes), assessing the skin for breakdown, and applying a new precut or cut-to-fit wafer. Some patients benefit from ostomy paste, rings, or powder to contour uneven abdominal surfaces or manage weepy skin. The "crusting technique"—applying powder, sealing with a skin prep barrier film, and repeating—is highly effective for irritated peristomal dermatitis.
- Skin Care: Protecting the skin around your stoma (peristomal skin) is crucial. Stool from the small intestine can be very irritating to the skin, so a properly fitting wafer is essential to prevent leakage. Peristomal dermatitis is the most common ostomy-related complication and typically presents as a bright red, painful, weeping rash. Immediate intervention with skin barrier powders, crusting techniques, and adjusting the wafer aperture to within 1-2mm of the stoma base can rapidly resolve mild to moderate irritation. If a rash persists beyond a week or shows signs of fungal infection (pustules, satellite lesions, intense itching), a WOC nurse should be consulted for prescription antifungal barrier pastes or creams.
Diet and Nutrition
After surgery, your stool output will be liquid. Over time, it will thicken to a paste-like consistency. Navigating nutrition post-ileostomy requires a methodical, trial-and-error approach tailored to individual tolerance. Keeping a food and symptom journal for the first 6 to 8 weeks is highly recommended to identify personal triggers and tolerances.
- Hydration is Critical: Because stool is bypassing the colon (where water is absorbed), you are at a higher risk of dehydration. It is vital to drink 8 to 10 cups of fluid daily, but water alone is often insufficient. High ileostomy output rapidly depletes sodium, potassium, and magnesium. Patients are strongly advised to incorporate oral rehydration solutions (ORS), sports drinks, or broths into their daily routine to maintain electrolyte homeostasis and prevent acute kidney injury. A practical tip is to separate fluid intake from meals; drinking large amounts during meals can flush food through the stoma too quickly, whereas sipping fluids 30-45 minutes before or after eating optimizes absorption.
- Initial Diet: For the first few weeks, your doctor will likely recommend a low-fiber, bland diet. Easily digestible foods like white rice, bananas, applesauce, toast, eggs, and lean poultry are excellent starting points. Chewing food thoroughly is non-negotiable, as larger boluses cannot be efficiently digested by the shortened functional pathway. Gradually introduce one new food every two days to monitor tolerance. If a particular food causes cramping, gas, or high output, note it and reintroduce it later in smaller quantities or with a different preparation method (e.g., cooking raw vegetables).
- Food Blockages: Some high-fiber foods (like nuts, corn, and raw vegetables) can potentially cause a blockage. It's important to chew food thoroughly and reintroduce these items one at a time. Other known culprits include popcorn, coconut, mushrooms, and tough meat gristle. If a partial obstruction is suspected (characterized by cramping, bloating, and a sudden drop in output), drinking warm liquids, taking a warm bath, and gentle abdominal massage may help relax the intestinal smooth muscle and restore flow. Persistent symptoms require immediate medical evaluation.
Odor and Gas Management
Odor and excessive gas are common concerns that are highly manageable with dietary adjustments and product selection. Gas-producing foods like carbonated beverages, beans, broccoli, cabbage, onions, and beer should be introduced cautiously. Conversely, foods like yogurt, kefir, cranberry juice, and parsley may naturally help neutralize odors. Eating regular, smaller meals instead of three large ones can regulate bowel motility and reduce gas accumulation. Modern pouches often include integrated charcoal filters that vent odorless gas, though these can become clogged by thick output and may need replacement if blocked. Filter stickers or patches are available to replace clogged filters without changing the entire pouch. Using ostomy deodorant drops or drops inside the pouch can further control odor, and some patients find probiotic supplementation beneficial for regulating gut flora and minimizing foul-smelling byproducts.
 (Image Source: Dr. Neeraj Singh, MD, FACS, FASCRS)
(Image Source: Dr. Neeraj Singh, MD, FACS, FASCRS)
Daily Life and Activities
With proper care, an ileostomy shouldn't limit you. The human body is remarkably adaptable, and with modern pouching technology, ostomates routinely engage in physically demanding hobbies, travel extensively, and maintain active professional lives.
- Showering and Swimming: You can shower and swim with or without your pouch on. Water will not harm the stoma. If bathing without a pouch, the stoma may temporarily expel stool due to warm water stimulation; having a washcloth and towel ready is practical. For swimming, specialized waterproof covers or simply wearing a regular pouch (which does not absorb water like a sponge) are effective. Always ensure the wafer is fully adhered before water exposure, as moisture can compromise the seal if the edges are already lifting.
- Clothing: Most clothing will fit comfortably over your ostomy. Many people prefer avoiding tight waistbands directly over the stoma. High-waisted underwear, ostomy support garments, and seamless fabrics can provide gentle compression without irritating the pouching system. Some patients use lightweight pouch covers made of breathable cotton or moisture-wicking fabric to reduce noise, absorb perspiration, and prevent the pouch from sticking to the skin in warm climates.
- Exercise and Travel: Once you have recovered, you can return to most physical activities. Core strengthening should be reintroduced gradually to prevent parastomal herniation. Focus on diaphragmatic breathing and transverse abdominis engagement before progressing to planks or heavy resistance training. With some planning, travel is entirely possible—just be sure to pack extra supplies in both carry-on and checked luggage, research medical supply availability at your destination, and carry a physician's note for airport security screenings. Most airport scanners and pat-down protocols accommodate ostomy supplies discreetly. Keeping a travel emergency kit (containing extra pouches, barrier wipes, disposal bags, and a change of clothes) ensures peace of mind during long trips.
- Intimacy: Open communication with your partner is key. Smaller pouches or pouch covers can help with confidence. Intimacy does not need to wait until full physical recovery, but consulting your care team about optimal timing and positions that avoid stoma pressure is advisable. Emptying the pouch before intimacy, using a support wrap to minimize bulging, and exploring comfortable positions that reduce direct contact with the stoma area can alleviate concerns. The emotional intimacy fostered through honest conversation often outweighs initial physical insecurities, and many couples report that navigating this phase strengthens their relationship.
Potential Risks and Complications
While generally safe, a loop ileostomy has potential complications. Awareness and early recognition are the best defenses against escalation. Most issues are manageable with conservative measures, but knowing when to seek urgent care can prevent hospitalization.
- Dehydration and Electrolyte Imbalance: Due to high liquid output, this is a primary concern and a frequent reason for hospital readmission. High-output stoma syndrome, defined as greater than 1,500 mL to 2,000 mL of daily output, can rapidly lead to hypovolemia, hyponatremia, hypomagnesemia, and prerenal acute kidney injury. Patients should monitor urine output and color, and seek immediate care if experiencing dizziness, extreme fatigue, dark urine, or tachycardia. Medical management typically includes loperamide or diphenoxylate-atropine to slow motility, along with dietary modifications and structured ORS protocols. In severe cases, patients may require outpatient or inpatient IV hydration, and fiber supplements like psyllium husk can be titrated to naturally thicken output.
- Skin Irritation: Leakage of stool onto the skin can cause painful rashes and breakdown. Peristomal skin complications affect nearly half of all ostomy patients at some point. Preventive measures include precise wafer sizing, using convex barriers for retracted or flush stomas, and avoiding adhesive removers with harsh chemicals. Chronic dermatitis may require prescription topical corticosteroids or antifungal agents. Regular skin assessments using a standardized scale help track healing progress and adjust care plans proactively.
- Stoma Prolapse or Retraction: The stoma may protrude further out (prolapse) due to increased intra-abdominal pressure or fascial widening, or sink below the skin level (retraction) due to inadequate bowel mobilization, weight gain, or ischemia. Mild prolapse is often managed conservatively with support garments and pouching adjustments, while severe cases or symptomatic retraction causing frequent leaks may require surgical revision. Applying gentle, consistent pressure with a cold compress can reduce mild prolapse edema, and avoiding straining during bowel movements or heavy lifting minimizes recurrence risk.
- Parastomal Hernia: The abdominal muscles around the stoma may weaken, causing a bulge. This occurs in up to 50% of patients within the first two years, as the fascial trephine creates a permanent weakness in the abdominal wall. Risk mitigation includes avoiding heavy lifting (>10-15 lbs) during initial healing, maintaining a healthy weight, and wearing prophylactic hernia support belts. Large or symptomatic hernias causing obstruction or pouching difficulties may eventually require mesh repair or stoma relocation. Core stabilization exercises, when properly guided, can actually reduce hernia progression by reinforcing the transversalis fascia.
- Food Blockage: As mentioned, certain foods can obstruct the stoma, causing pain, cramping, and a stop in output. Complete obstructions are surgical emergencies and present with severe, colicky abdominal pain, nausea, vomiting, and absolute absence of stoma output. Early recognition and prompt intervention are critical to prevent bowel ischemia or perforation. Preventive strategies include meticulous chewing, avoiding known problematic foods during the initial adaptation phase, and staying consistently hydrated to maintain optimal stool viscosity.
Loop Ileostomy Reversal (Closure)
The good news is that a diverting loop ileostomy is designed to be temporary. The reversal surgery is a less invasive procedure where the surgeon reconnects the loop of the ileum and closes the stoma site on the abdomen. The procedure typically involves a small elliptical incision around the stoma, dissection to mobilize the bowel, restoration of intestinal continuity via hand-sewn or stapled anastomosis, and layered closure of the abdominal wall.
When is Reversal Performed? The Timing Debate
The traditional timeline for reversal is around 3 to 6 months after the initial surgery. However, recent research, including a 2025 study in Surgery, notes that the actual time to reversal is often longer, with a median of 5.5 months for rectal cancer patients. Delays can be caused by the need for adjuvant chemotherapy, postoperative complications, or scheduling issues. Patients must also meet specific physiological criteria before reversal, including adequate weight maintenance, normalized inflammatory markers, and satisfactory nutritional labs.
Before reversal is approved, the surgical team must verify that the downstream anastomosis is fully healed and functional. This typically involves a contrast enema (Gastrografin study) to rule out strictures or silent leaks, flexible sigmoidoscopy to visually inspect the mucosal healing, and sometimes anorectal manometry to assess sphincter tone. If the distal bowel was radiated or severely diseased, these evaluations are even more critical to prevent catastrophic failure upon restoration of continuity. Digital rectal exams may also be performed to evaluate anal sphincter contractility and rectal compliance.
There's an ongoing clinical debate about the optimal timing:
- Early Reversal (within 2 months): May reduce the time a patient lives with a stoma and its associated complications, but some studies suggest a slightly higher risk of reversal-related complications like bowel obstruction or anastomotic breakdown if tissue healing is incomplete. Early reversal is often favored in younger, healthier patients with straightforward recoveries.
- Delayed Reversal (after 5-6 months): Waiting too long may increase the risk of digestive issues like diarrhea and incontinence after reversal, as the colon can become atrophied or the pelvic floor muscles may decondition from prolonged disuse. There is also a higher risk of stoma-related complications such as dehydration, prolapse, and significant quality of life deterioration. However, delayed timing allows complete resolution of surgical inflammation and uninterrupted completion of neoadjuvant or adjuvant cancer therapies.
The decision is highly individualized and made in consultation with your surgeon. Patient preference, oncologic treatment schedules, nutritional optimization, and anatomical readiness are all factored into the final timeline. Shared decision-making models that incorporate patient-reported outcome measures (PROMs) have proven effective in aligning clinical timelines with personal recovery goals.
Risks of Reversal Surgery
While safer than the initial operation, reversal surgery carries its own risks:
- Anastomotic Leak: The reconnected bowel may leak, potentially causing pelvic abscess or sepsis. Strict preoperative bowel preparation and meticulous intraoperative perfusion assessment help mitigate this risk.
- Small Bowel Obstruction: Scar tissue (adhesions) can form at the surgical site, causing a blockage that may require additional intervention. Early postoperative ambulation and avoiding prolonged fasting when possible support normal motility restoration.
- Incisional Hernia: A hernia can develop at the closed stoma site due to fascial closure under tension or wound infection. Layered closure techniques with slowly absorbable or permanent sutures are commonly used to reinforce the site.
- Infection: As with any surgery, there is a risk of superficial or deep wound infection, often managed with antibiotics or minor drainage procedures. Keeping the surgical incision clean and dry during the first 48 hours is paramount.
- Altered Bowel Habits: Post-reversal, patients frequently experience Low Anterior Resection Syndrome (LARS) symptoms, including clustering, urgency, frequency, and occasional incontinence. Bowel retraining, pelvic floor physical therapy, and dietary fiber modulation are typically prescribed to restore functional control over 6 to 12 months. Biofeedback therapy and sacral nerve modulation are advanced options for refractory cases, but most patients achieve satisfactory control through structured rehabilitation.
Diverting Loop Ileostomy vs. Other Stomas
It's helpful to understand how a loop ileostomy compares to other types of stomas. This knowledge empowers patients to set realistic expectations and understand the surgical rationale behind stoma selection.
Loop Ileostomy vs. End Ileostomy
| Feature | Diverting Loop Ileostomy | End Ileostomy |
|---|---|---|
| Duration | Usually temporary | Usually permanent |
| Structure | A loop of intestine creates one stoma with two openings | The end of the intestine creates one stoma with a single opening |
| Purpose | To divert stool to protect a healing surgical site | To permanently divert stool when the large intestine is removed |
| Reversal | Simpler reversal procedure | Reversal is more complex and often not possible |
| Output Characteristics | Often higher volume initially, easier to reverse due to preserved distal anatomy | Consistent liquid/pasty output, requires lifelong pouch management |
Loop Ileostomy vs. Loop Colostomy
The choice between an ileostomy (small intestine) and a colostomy (large intestine) for temporary diversion is a topic of much clinical research. The selection depends heavily on disease location, surgical access, and patient-specific factors.
- Ileostomy Output: Liquid to paste-like, high volume. Requires diligent hydration and electrolyte monitoring. Pouches fill more frequently but typically use thinner, drainable systems. The effluent contains active digestive enzymes, which can be more caustic to the skin but allows for more predictable pouch drainage patterns.
- Colostomy Output: Thicker to more formed, lower volume. Easier to manage for some patients but carries a higher risk of stoma prolapse due to the larger diameter and redundant nature of the colon. Odor can be more pronounced initially, but formed stool makes irrigation (colostomy irrigation) a viable option for achieving regular, predictable evacuation without constant pouch wear.
A meta-analysis cited by the National Institutes of Health (NIH) found that loop ileostomies are generally preferred because they are associated with lower rates of stoma prolapse and sepsis. However, loop ileostomies carry a significantly higher risk of dehydration and acute kidney injury due to high output. A loop colostomy may be chosen for patients with pre-existing kidney problems, chronic dehydration, or if the diversion is expected to be long-term and distal pelvic healing is less of a priority. The decision is heavily influenced by the surgeon's expertise, the patient's baseline renal function, and the specific anatomical constraints of the primary disease process.
The Clinical Debate: When is Diversion Necessary?
While a diverting ileostomy can be lifesaving, it comes with its own set of complications and a significant impact on quality of life. This has led to a clinical debate on whether it should be used routinely in certain procedures (like low rectal cancer surgery) or only selectively for high-risk patients. Ongoing trials are evaluating predictive biomarkers and intraoperative perfusion metrics to refine patient selection criteria.
The current consensus leans towards selective use. Factors that place a patient at high risk for an anastomotic leak, and therefore make them a strong candidate for a diverting ileostomy, include:
- A very low anastomosis (close to the anus)
- Male gender (associated with a narrower pelvis and technically more challenging dissection)
- Malnutrition (low albumin or prealbumin levels impair tissue repair)
- Pre-operative radiation (compromises microvascular blood flow and tissue elasticity)
- A technically difficult surgery or intraoperative concerns about bowel perfusion
- Chronic steroid use or immunosuppression
Conversely, younger, well-nourished patients with well-vascularized tissue undergoing mid-to-high rectal or colonic anastomoses may safely undergo primary anastomosis without diversion. Risk stratification scores, such as the Dutch Colorectal Risk Score, are increasingly utilized by multidisciplinary tumor boards to objectively weigh the probability of anastomotic leakage against the morbidity of stoma creation and subsequent reversal. Patient-reported outcome measures (PROMs) consistently show that while short-term quality of life dips post-ileostomy, the majority of patients view the procedure favorably if it is clearly framed as a protective, temporary bridge to full recovery. Transparent communication, realistic expectation setting, and comprehensive preoperative counseling are the cornerstones of ethical and effective stoma care.
References
- Mayo Clinic. (2025). Ileostomy. https://www.mayoclinic.org/tests-procedures/ileostomy/about/pac-20582350
- Plasencia, A., et al. (2019). Diverting Ostomy: For Whom, When, What, Where, and Why. Clinics in Colon and Rectal Surgery, 32(3), 156–162. https://pmc.ncbi.nlm.nih.gov/articles/PMC6500738/
- Withe, M. (2024). Loop ileostomy: What to expect, risks, and reversal. Medical News Today. https://www.medicalnewstoday.com/articles/loop-ileostomy
- Cleveland Clinic. (2023). Ileostomy: What Is It, Types, Bags, Surgery & Complications. https://my.clevelandclinic.org/health/procedures/21726-ileostomy
- Boyer, M.E., et al. (2025). Assessing the pathway and timing for ileostomy reversal in rectal cancer: A retrospective cohort study. Surgery. https://www.sciencedirect.com/science/article/abs/pii/S0039606025003599
Frequently Asked Questions
How long will my loop ileostomy need to stay in place?
The duration of a diverting loop ileostomy varies based on the underlying condition, the healing progress of the downstream surgical connection, and whether additional treatments like chemotherapy are required. On average, patients live with a temporary loop ileostomy for 3 to 6 months before it is surgically reversed. However, in complex cases involving severe pelvic radiation, inflammatory bowel disease flare-ups, or delayed tissue healing, the timeline can extend to 8-12 months. Your surgeon will determine the exact timing through imaging studies and clinical evaluation to ensure the reversal is as safe as possible.
Can I take regular medications with an ileostomy?
Most oral medications can still be absorbed effectively, but some require adjustments. Extended-release, sustained-release, or enteric-coated pills may pass through your system too quickly to be fully absorbed. Your pharmacist or physician may need to switch you to immediate-release formulations, liquid medications, or sublingual patches. It is also important to crush pills only if explicitly approved by your healthcare provider, as some medications lose efficacy or cause mucosal irritation when altered. Always consult your care team or a pharmacist before changing how you take any prescription or over-the-counter drug.
What should I do if my stoma stops working or output suddenly drops to zero?
A sudden cessation of stoma output, especially when accompanied by cramping, nausea, bloating, or vomiting, is a potential red flag for a food blockage or mechanical bowel obstruction. Begin by drinking warm fluids like water, herbal tea, or clear broth, and try taking a warm bath or applying a heating pad to your abdomen to relax intestinal muscles. Gently massaging the area around the stoma in a clockwise direction may help stimulate peristalsis. If output does not resume within 6 hours, or if pain becomes severe, contact your surgical team immediately or proceed to the nearest emergency department. Do not attempt to force laxatives, as this can worsen a complete obstruction.
Will I be able to work and exercise normally after reversal surgery?
Yes, most patients return to work and resume their regular exercise routines within 4 to 8 weeks after ileostomy reversal. Initially, you may need to limit heavy lifting (>15 lbs) and high-impact activities to allow the abdominal incision and internal bowel reconnection to heal fully. Core-strengthening exercises, particularly those guided by a physical therapist, are highly beneficial for preventing incisional hernias and improving pelvic floor function. It is normal to experience increased bowel frequency and urgency during the transition period, so keeping a detailed symptom log and scheduling bathroom breaks strategically during your workday can ease the return to professional and athletic life.
How do I manage dehydration when I have high stoma output?
Managing high output requires a strategic approach to fluid replacement that prioritizes electrolytes over plain water. Drinking excessive amounts of water without replacing lost sodium can actually worsen dehydration by further diluting blood electrolyte levels. Instead, aim for a daily intake of specialized oral rehydration solutions (ORS), sports drinks, or broths that contain balanced ratios of sodium, potassium, and glucose. Limit diuretic beverages like coffee, alcohol, and sugary sodas. Incorporating binding foods like bananas, white rice, applesauce, peanut butter, and marshmallows can naturally thicken output. If daily pouch output consistently exceeds 1,500 mL despite these measures, your physician may prescribe antimotility medications like loperamide and monitor your kidney function closely.
Conclusion
A diverting loop ileostomy is a powerful, life-preserving surgical intervention that plays a vital role in the modern management of complex colorectal diseases. While adjusting to a temporary stoma requires patience, education, and proactive self-care, the overwhelming majority of patients successfully navigate the recovery period and ultimately undergo a smooth reversal procedure. By understanding the anatomical rationale, mastering daily pouch management, prioritizing hydration and nutrition, and recognizing the warning signs of complications, patients can maintain a high quality of life throughout their ostomy journey. Close collaboration with your surgical team, WOC nurses, and peer support networks ensures that every phase of care—from initial creation to final reversal and bowel retraining—is guided by evidence-based practices tailored to your unique physiological needs. Ultimately, viewing the ileostomy not as a permanent setback but as a strategic, protective phase in your broader treatment pathway fosters resilience and empowers you to reclaim your health, daily routines, and long-term wellness goals.

About the author
Fatima Al-Jamil, MD, MPH, is board-certified in gastroenterology and hepatology. She is an Assistant Professor of Medicine at a university in Michigan, with a clinical focus on inflammatory bowel disease (IBD) and motility disorders.