Strangulated Hernia: A Comprehensive Guide to Symptoms, Risks, and Emergency Treatment

Key points
- Sudden, severe, and rapidly worsening pain at the hernia site or in the abdomen. The pain often shifts from a dull, positional ache to a constant, unrelenting, and excruciating sensation that does not resolve with rest or over-the-counter analgesics.
- A hernia bulge that becomes firm, tender, and cannot be pushed back in. The skin overlying the bulge may feel tense, hot to the touch, or exquisitely sensitive to even light palpation.
- Red, purple, or dark discoloration of the skin over the hernia. This color change reflects superficial vascular congestion and underlying tissue ischemia. It is a late and highly ominous sign that necrosis may already be underway.
- Nausea and vomiting. These gastrointestinal symptoms occur as the digestive tract becomes obstructed or as the body mounts a systemic stress response to tissue injury and early sepsis.
- Fever. An elevated temperature indicates an inflammatory or infectious process. In the context of a hernia, it strongly suggests bacterial translocation, localized abscess formation, or systemic infection.
- Inability to pass gas or have a bowel movement (a sign of bowel obstruction). Complete mechanical obstruction halts peristalsis and prevents the passage of intestinal contents, leading to progressive distension and discomfort.
A hernia might start as a small, painless bulge, but it holds the potential to become a life-threatening medical emergency. When a hernia becomes strangulated, it's a race against time where immediate medical intervention is critical. Understanding the signs, risks, and the necessity for urgent treatment can be the difference between a full recovery and devastating complications.
This comprehensive guide synthesizes information from leading medical institutions and patient experiences to provide a complete picture of what a strangulated hernia is, how to recognize it, and what to expect from treatment. The physiological mechanisms behind hernia strangulation are complex, but recognizing the clinical pathway can empower patients and caregivers to act swiftly when symptoms arise. Early recognition, prompt emergency response, and specialized surgical intervention form the cornerstone of survival and optimal recovery in these high-acuity scenarios.
What is a Strangulated Hernia?
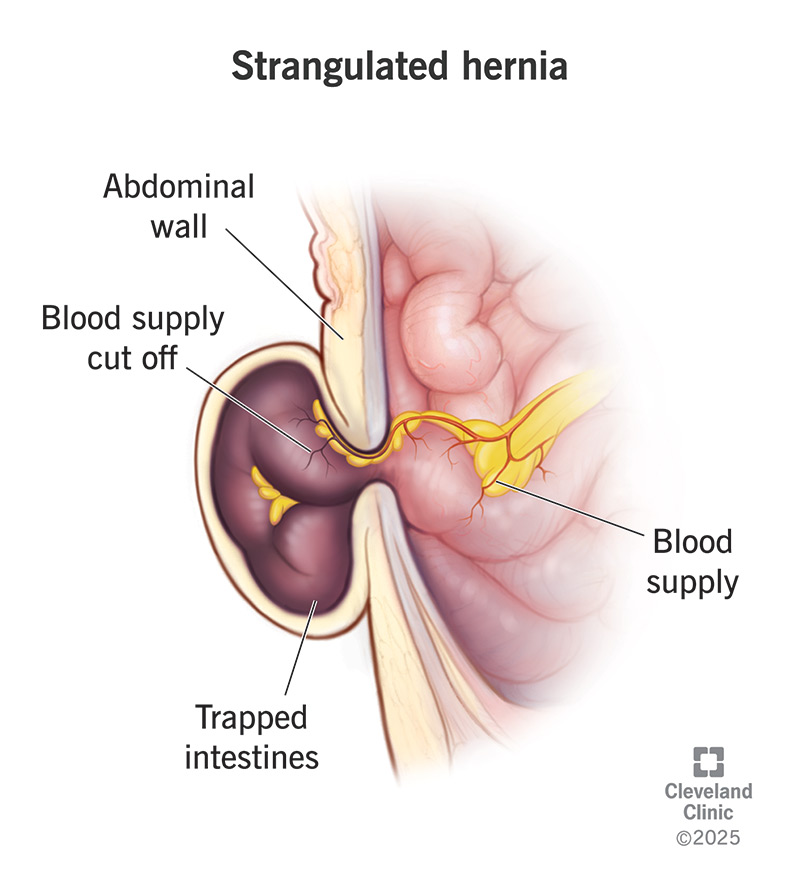
A strangulated hernia is the most severe complication of a hernia. It occurs when a section of tissue, often part of the intestine or abdominal fat, pushes through a weak spot in the abdominal wall and becomes so tightly trapped that its blood supply is completely cut off.
According to the Cleveland Clinic, this lack of blood flow causes the tissue to be starved of oxygen, leading to cell death (necrosis) and potentially gangrene within hours. This is not just a worsening of hernia pain; it is a surgical emergency that can prove fatal if left untreated.
 Source: Cleveland Clinic
Source: Cleveland Clinic
The pathophysiology of strangulation involves a cascade of vascular compromise. Initially, the constriction impedes venous outflow, causing the trapped tissue to swell and become edematous. This swelling increases pressure within the confined space, which subsequently obstructs arterial inflow. Without oxygenated blood, cellular metabolism shifts to anaerobic pathways, producing lactic acid and causing local tissue acidosis. If perfusion is not rapidly restored, ischemic necrosis sets in. When intestinal tissue is involved, the mucosal barrier breaks down, allowing gut bacteria to translocate into the peritoneal cavity. This bacterial translocation is what precipitates severe intra-abdominal infections and systemic inflammatory responses. Omental tissue can also become strangulated, though it generally presents a slightly less acute infectious risk compared to bowel involvement. Regardless of the tissue type, the principle remains: compromised blood flow equals impending tissue loss and systemic toxicity.
The Progression: From Reducible to Strangulated
A hernia doesn't typically become strangulated overnight. It follows a dangerous progression:
- Reducible Hernia: An early-stage hernia where the protruding bulge can be gently pushed back into the abdomen. It may cause discomfort but is not an immediate danger. At this stage, the fascial defect is large enough to allow tissue to move freely without constricting its vascular pedicle. Many patients live for years with reducible hernias under medical observation.
- Incarcerated (or Irreducible) Hernia: The herniated tissue becomes trapped in the abdominal wall and cannot be pushed back in. As Healthline clarifies, an incarcerated hernia can lead to a bowel obstruction and is a precursor to strangulation, but it is not yet life-threatening on its own. The transition from reducible to incarcerated often occurs during sudden spikes in intra-abdominal pressure, such as heavy lifting, severe coughing fits, or straining. Once trapped, the tissue is subjected to continuous mechanical pressure from the surrounding fascial rings.
- Strangulated Hernia: The pressure from the surrounding muscle on the incarcerated tissue becomes so intense that it cuts off the blood flow. This is the critical stage where tissue begins to die, releasing toxins into the bloodstream and setting the stage for severe infection and sepsis. The transition from incarceration to strangulation can occur anywhere from a few hours to several days, but the median timeframe is alarmingly brief. Clinical studies suggest that the majority of strangulations develop within 12 to 48 hours of symptom onset following incarceration.
The timeline from incarceration to strangulation and necrosis can be alarmingly short. Tissue can become gangrenous within hours, highlighting the need for immediate action. Patients should never attempt forceful manual reduction of an incarcerated hernia at home, as this can cause iatrogenic bowel perforation, push necrotic tissue back into the peritoneal cavity, or mask ongoing strangulation while tissue continues to die internally.
Recognizing the Warning Signs: Symptoms of a Strangulated Hernia
It is crucial to distinguish the discomfort of a simple hernia from the severe symptoms of a strangulated one. If you have a known hernia and experience the following, seek emergency medical help immediately.
According to experts at the Mayo Clinic and Johns Hopkins Medicine, the key warning signs include:
- Sudden, severe, and rapidly worsening pain at the hernia site or in the abdomen. The pain often shifts from a dull, positional ache to a constant, unrelenting, and excruciating sensation that does not resolve with rest or over-the-counter analgesics.
- A hernia bulge that becomes firm, tender, and cannot be pushed back in. The skin overlying the bulge may feel tense, hot to the touch, or exquisitely sensitive to even light palpation.
- Red, purple, or dark discoloration of the skin over the hernia. This color change reflects superficial vascular congestion and underlying tissue ischemia. It is a late and highly ominous sign that necrosis may already be underway.
- Nausea and vomiting. These gastrointestinal symptoms occur as the digestive tract becomes obstructed or as the body mounts a systemic stress response to tissue injury and early sepsis.
- Fever. An elevated temperature indicates an inflammatory or infectious process. In the context of a hernia, it strongly suggests bacterial translocation, localized abscess formation, or systemic infection.
- Inability to pass gas or have a bowel movement (a sign of bowel obstruction). Complete mechanical obstruction halts peristalsis and prevents the passage of intestinal contents, leading to progressive distension and discomfort.
- A rapid heart rate. Tachycardia is an early compensatory mechanism for pain, dehydration, and impending hypovolemic or septic shock.
- Bloating or a full, round abdomen. As trapped bowel loops fill with fluid and gas, abdominal distension increases, often accompanied by a feeling of intense pressure or visible asymmetry.
When to Go to the ER: If you have a hernia and develop any of the symptoms listed above, do not wait. Go to the nearest emergency room or call for an ambulance immediately. This is a life-threatening condition.
It is also important to recognize atypical presentations. Elderly patients, individuals on chronic corticosteroids, or those with compromised immune systems may not mount a robust inflammatory response. In these populations, classic signs like fever or severe localized pain might be blunted or absent, leading to delayed diagnosis. Conversely, they may present primarily with confusion, generalized weakness, hypotension, or unexplained acidosis. Clinicians maintain a high index of suspicion for these vulnerable groups, often utilizing laboratory markers and imaging even when physical exam findings are equivocal. Additionally, pediatric hernias, particularly congenital indirect inguinal hernias in infants, can strangulate with startling speed. Parents should watch for persistent inconsolable crying, abdominal distension, vomiting (especially bilious green fluid), and a firm, discolored groin or scrotal bulge.
Risk Stratification: Who Is Most at Risk?
While any hernia can theoretically become strangulated, certain hernia types and patient factors carry a significantly higher risk.
High-Risk Hernia Types
- Femoral Hernias: Occurring in the upper thigh/groin, these have the highest risk of strangulation due to the narrow and rigid nature of the femoral canal where they protrude. The femoral ring is bounded by the inguinal ligament anteriorly, the pectineal ligament posteriorly, and the lacunar ligament medially, creating an unforgiving anatomical tunnel. Because of this, up to 20-40% of femoral hernias present as emergencies, and they are significantly more common in women due to wider pelvic anatomy.
- Indirect Inguinal Hernias: These are more likely to strangulate than direct inguinal hernias because they traverse the deep inguinal ring and the inguinal canal, often descending into the scrotum or labia. The internal ring can act as a constricting band, particularly in younger patients with a narrow canal.
- Hernias with Small Defects: Counterintuitively, hernias pushing through a smaller, tighter opening in the muscle are more likely to become trapped and have their blood supply constricted. A large fascial defect allows ample room for tissue movement, whereas a defect measuring 2-3 centimeters can act like a tourniquet around the hernia sac neck.
High-Risk Patient Profiles
- Patients with Irreducible Hernias: An inability to push the hernia back in is the most significant warning sign. Once a hernia becomes chronically incarcerated, the risk of progression to strangulation increases exponentially with each passing day.
- Individuals with Worsening Symptoms: Increasing pain, even without other signs, should prompt a visit to the doctor. Pain that changes character, intensity, or frequency often signals evolving mechanical stress or early vascular compromise.
- Factors Increasing Abdominal Pressure: Conditions like a chronic cough, straining during bowel movements, pregnancy, and strenuous heavy lifting can force tissue into the hernia sac and increase the risk of entrapment. Chronic obstructive pulmonary disease (COPD), benign prostatic hyperplasia (BPH), chronic constipation, and obesity all contribute to sustained intra-abdominal hypertension.
- Age and Tissue Quality: As individuals age, collagen cross-linking decreases, and fascial tissues lose elasticity. This degeneration makes the abdominal wall more susceptible to enlargement of hernia defects and less capable of accommodating shifting tissue without compromising perfusion.
- Previous Abdominal Surgeries: Scar tissue from prior operations creates adhesions that can tether bowel loops, creating fixed points that are prone to catching in hernia openings. These adhesions can also complicate surgical reduction and increase the likelihood of iatrogenic injury during emergency intervention.
- Connective Tissue Disorders: Conditions like Ehlers-Danlos syndrome or Marfan syndrome inherently weaken collagenous structures throughout the body. Patients with these disorders experience higher rates of hernia formation, faster hernia progression, and an elevated baseline risk for incarceration and strangulation.
Diagnosis and Immediate Medical Response
A strangulated hernia is typically diagnosed in an emergency room based on a physical examination and a review of the patient's severe symptoms. A doctor can often identify it by the firm, tender, and discolored bulge.
To confirm the diagnosis and assess the extent of the damage, imaging tests are often used:
- Abdominal Ultrasound or CT Scan: These tests can show the trapped tissue, check for signs of bowel obstruction, and confirm the lack of blood flow. A contrast-enhanced CT scan of the abdomen and pelvis is the gold standard for emergency evaluation. It provides detailed cross-sectional anatomy, clearly delineates the hernia neck, identifies the sac contents (bowel vs. omentum), and reveals complications like bowel wall thickening, mesenteric edema, free fluid, or pneumatosis intestinalis (gas within the bowel wall), which strongly indicates ischemia. Ultrasound is particularly valuable for pediatric patients, pregnant individuals, or as a rapid bedside tool to assess vascular flow using color Doppler. Absent or reversed arterial flow on Doppler is a direct confirmation of strangulation.
In addition to imaging, emergency physicians rely heavily on laboratory diagnostics to gauge systemic impact. Elevated white blood cell (WBC) counts, increased C-reactive protein (CRP), and rising lactic acid levels are common in strangulated hernias. Metabolic acidosis with an elevated anion gap suggests anaerobic metabolism and tissue necrosis. These biomarkers, combined with clinical and radiographic findings, help surgical teams prioritize the case and anticipate intraoperative findings.
Once diagnosed, the only course of action is immediate surgery. Time from ER presentation to the operating room is a critical metric in surgical quality programs. Protocols are activated immediately: nothing by mouth (NPO) status is enforced, intravenous access is established, broad-spectrum antibiotics and fluid resuscitation are initiated, and a surgical team is paged for urgent intervention.
!Medical professionals reviewing a CT scan
Treatment: Emergency Surgery is Essential
Surgery is the only treatment for a strangulated hernia and must be performed as soon as possible. The primary goals of the operation are to release the trapped tissue, restore blood flow, and repair the hernia defect.
The surgical procedure typically involves:
- Making an incision over the hernia. Open surgery is often preferred in emergencies to allow the surgeon a clear view. The direct access enables rapid decompression of the strangulating ring, thorough inspection of compromised tissues, and effective management of contamination if bowel necrosis is present. While minimally invasive techniques are standard for elective repairs, the complexity and unpredictability of strangulation often necessitate an open approach, particularly when bowel resection or extensive adhesiolysis is anticipated.
- Releasing the trapped tissue (reducing the hernia). The surgeon carefully divides the constricting fascial ring or ligament under direct visualization to relieve pressure. This step must be performed with extreme caution to avoid damaging adjacent nerves, blood vessels, or the already ischemic bowel itself.
- Assessing tissue viability. The surgeon carefully inspects the tissue to see if it is still alive. If blood flow returns and the tissue appears healthy, it is returned to the abdominal cavity. Viability assessment involves observing the return of color, peristalsis, and pulsatile mesenteric bleeding. Intraoperative fluorescence imaging (using indocyanine green) is increasingly utilized to objectively evaluate microvascular perfusion when visual assessment is equivocal.
- Bowel Resection. If the tissue (often a part of the intestine) is necrotic or dead, that section must be surgically removed, and the healthy ends of the intestine are reconnected. In cases of severe contamination, widespread edema, or hemodynamic instability, the surgeon may opt to create a temporary ostomy (colostomy or ileostomy) rather than perform a primary anastomosis. This allows the bowel to rest and heal while diverting fecal matter away from a compromised surgical site.
- Hernia Repair. The weakened area in the abdominal wall is repaired, often using stitches or a synthetic mesh to reinforce the area and prevent recurrence. However, the decision to use mesh in contaminated fields is highly nuanced. While modern lightweight meshes and biologic alternatives have expanded options, surgeons traditionally prefer primary suture repair or biologic grafts in the presence of frank infection or bowel resection to minimize the risk of mesh colonization and chronic infection.
A complex case published by the American College of Surgeons details a multi-stage, multidisciplinary approach involving both abdominal and thoracic surgeons to save a patient with a severely strangulated hiatal hernia, underscoring the gravity and complexity of these emergencies.
Post-operative care in the immediate setting involves intensive monitoring. Patients are typically managed in a surgical ward or intensive care unit depending on the degree of systemic insult. Intravenous antibiotics are continued to cover gram-negative and anaerobic organisms common in gastrointestinal flora. Pain is managed through multimodal analgesia, and early mobilization is encouraged as soon as hemodynamically stable to prevent venous thromboembolism and pulmonary complications.
Recovery, Prognosis, and Long-Term Outlook
The prognosis after surgery for a strangulated hernia depends almost entirely on how quickly the patient received treatment.
Prognosis and Mortality Rates
When a hernia strangulates, the outlook becomes much more serious. A large Swedish study highlighted by The British Hernia Centre found that:
- The risk of death after an emergency hernia operation is 7 times higher than for a planned, elective repair.
- If a bowel resection is required due to dead tissue, the mortality risk is 20 times higher.
Delayed treatment is the most significant factor in poor outcomes. The presence of bowel necrosis dramatically worsens the prognosis and increases the risk of post-operative complications like severe infection (peritonitis), sepsis, and shock. The physiological toll of emergency surgery, combined with the inflammatory cascade of necrotic bowel, places immense strain on cardiopulmonary and renal systems. Patients with significant comorbidities such as diabetes, chronic kidney disease, or cardiovascular disease face disproportionately higher risks.
The Recovery Process and Long-Term Quality of Life
Recovery from emergency surgery is more involved than from an elective procedure. A hospital stay of several days is usually required, and patients may need antibiotics for infection. Full recovery can take several weeks, with restrictions on strenuous activity and heavy lifting. The immediate post-operative period focuses on wound care, infection surveillance, and gradual dietary advancement. Initially, a clear liquid diet is introduced and slowly advanced to full liquids and soft foods as bowel function returns, confirmed by the return of flatus and bowel movements.
Long-term complications can include:
- Chronic Pain: A small percentage of patients experience chronic pain at the surgical site. This neuropathic or inflammatory pain can result from nerve entrapment, mesh irritation, or scar tissue formation. Specialized pain clinics and targeted nerve blocks may be required for refractory cases.
- Hernia Recurrence: There is a risk that the hernia can return. Recurrence rates are slightly higher in emergency settings compared to elective repairs due to tissue inflammation, compromised healing capacity, and sometimes the omission of synthetic mesh.
- Mesh Complications: In rare cases, issues can arise with the surgical mesh used in the repair. These can include chronic inflammation, adhesion formation, or infection. Biologic meshes, while more expensive, offer a favorable safety profile in contaminated environments.
Despite these risks, most patients who receive timely treatment go on to live a full and healthy life. Structured rehabilitation programs, including core-strengthening exercises under physical therapy guidance, significantly reduce recurrence risk and improve functional outcomes. Psychological support is also increasingly recognized as a vital component of recovery, as the trauma of a near-fatal emergency and subsequent major surgery can lead to anxiety, depression, or post-traumatic stress symptoms that benefit from professional counseling.
The Dangers of Delay: What Happens if Left Untreated?
Ignoring a hernia can have devastating consequences, as one patient shared in a harrowing account on Health.com. After ignoring her doctor's advice for years, she experienced excruciating pain that she initially mistook for a stomach bug. By the time she reached the hospital, she had a strangulated hernia and a severe infection in her colon. Her doctors told her that waiting another 24 hours could have been fatal.
This experience highlights a critical truth: hernias do not go away on their own. The "watch and wait" approach is only safe under a doctor's supervision and for hernias that are asymptomatic and at low risk of complications. An untreated strangulated hernia will lead to:
- Gangrene of the trapped intestine. The complete cessation of blood flow causes irreversible tissue death. The affected segment turns black, becomes friable, and loses all structural integrity.
- Perforation (a hole) in the bowel wall. As necrosis advances, the intestinal wall thins and ruptures, spilling highly caustic digestive enzymes and fecal bacteria directly into the sterile peritoneal cavity.
- Peritonitis, a severe infection of the abdominal lining. The chemical and bacterial contamination triggers an aggressive inflammatory response, causing intense abdominal rigidity (guarding), rebound tenderness, systemic fever, and rapid clinical deterioration.
- Sepsis, a body-wide, life-threatening reaction to infection. The systemic inflammatory response syndrome (SIRS) leads to widespread vasodilation, capillary leak, myocardial depression, and microvascular thrombosis. Without aggressive ICU support including vasopressors, mechanical ventilation, and renal replacement therapy, multi-organ failure ensues.
- Death. Mortality rates skyrocket once sepsis progresses to septic shock or when bowel perforation leads to overwhelming peritonitis. The window for successful intervention closes rapidly once systemic organ dysfunction establishes itself.
Elective hernia repair remains the single most effective strategy to prevent these catastrophic outcomes. By addressing hernias while they are still reducible and asymptomatic, surgeons can utilize optimal tissue conditions, employ standard mesh reinforcement techniques, and schedule procedures during peak patient health, virtually eliminating the risk of strangulation.
Frequently Asked Questions (FAQ)
What is a strangulated hernia?
A strangulated hernia is a life-threatening medical emergency that occurs when the blood supply to tissue trapped in a hernia (often a part of the intestine) is cut off by the surrounding muscle. This lack of blood flow leads to tissue death (necrosis), which can cause severe complications like gangrene, sepsis, and bowel perforation if not treated with immediate surgery. The term "strangulation" specifically refers to vascular compromise, distinguishing it from simple incarceration where tissue is trapped but still perfused.
How can you tell if your hernia is strangulated?
Key signs of a strangulated hernia include: sudden, severe, and worsening pain at the hernia site; a bulge that is firm, tender, and cannot be pushed back in; redness, purple, or dark discoloration of the skin over the hernia; nausea and vomiting; fever; bloating and an inability to pass gas or have a bowel movement; and a rapid heart rate. If you experience these symptoms, seek emergency medical care immediately. Note that symptom severity does not always correlate directly with the degree of tissue damage; some patients present with profound ischemia despite moderate pain, particularly if analgesics have been taken or if nerve function is compromised by local edema.
What happens if a hernia bursts or ruptures?
A hernia 'bursting' or rupturing is a rare but catastrophic medical emergency. It means the weakened muscle tissue has torn completely, allowing the hernia's contents (like the intestine) to spill into the body cavity or through the skin in severe neglected cases. This can lead to severe internal bleeding, widespread infection (peritonitis), and tissue death. It requires immediate emergency surgery, which is often more complex and has a longer recovery than a planned hernia repair. Rupture through the skin, known as an open or eviscerated hernia, carries an exceptionally high infection risk and necessitates immediate wound coverage, aggressive resuscitation, and emergent operative debridement.
How long can you live with an untreated hernia?
While a person can live for months or even years with a small, asymptomatic hernia, it is not recommended to leave it untreated. Hernias do not heal on their own and tend to worsen over time. The primary danger is the risk of it becoming incarcerated (trapped) and then strangulated, which is a life-threatening emergency that can develop suddenly. The unpredictability of hernia behavior makes proactive surgical consultation advisable for virtually all diagnosed hernias, particularly those that are growing, symptomatic, or located in high-risk anatomical regions like the femoral canal.
Can a strangulated hernia happen without noticeable pain?
Yes, though it is uncommon. Patients with advanced age, diabetes-induced neuropathy, chronic opioid use, or immunosuppressive therapy may experience blunted pain responses. In these populations, the primary warning signs may be subtle, such as unexplained lethargy, low-grade fever, mild nausea, or a firm groin mass that simply "doesn't look right." Healthcare providers emphasize that absence of severe pain does not rule out strangulation in high-risk demographics, and clinical suspicion should drive imaging and surgical evaluation.
Is mesh always used when repairing a strangulated hernia?
No. The decision to use mesh during emergency hernia surgery depends heavily on the degree of contamination and tissue viability. In clean cases where bowel is viable and reduced, synthetic mesh is commonly placed to reduce recurrence risk. However, when bowel necrosis requires resection, the surgical field is classified as contaminated or dirty-infected. In these scenarios, placing permanent synthetic mesh carries a high risk of bacterial colonization and chronic infection. Surgeons typically opt for primary tissue suture repair or biologic/absorbable mesh in contaminated fields, with a plan for definitive elective mesh reinforcement at a later date once the patient has fully healed.
What lifestyle changes can prevent hernias from strangulating?
Preventing progression begins with early medical evaluation. Beyond surgical intervention, maintaining a healthy weight reduces chronic intra-abdominal pressure. Proper lifting techniques (engaging legs rather than the core), managing chronic cough with appropriate medications, treating constipation with adequate fiber and hydration, and addressing urinary retention or prostate enlargement all contribute to minimizing strain on the abdominal wall. Smoking cessation is particularly critical, as tobacco use impairs collagen synthesis and tissue healing, significantly increasing both hernia formation and recurrence rates.
Conclusion
A strangulated hernia represents one of the most urgent acute surgical conditions encountered in clinical medicine. The transition from a benign, reducible bulge to a life-threatening vascular emergency can occur with alarming speed, making patient awareness and rapid medical response absolutely essential. Recognizing the hallmark symptoms—sudden severe pain, an irreducible firm bulge, skin discoloration, systemic signs like fever and tachycardia, and gastrointestinal obstruction—can save lives.
Understanding risk factors, including hernia type, anatomical defect size, chronic intra-abdominal pressure, and individual patient health profiles, empowers individuals to seek timely elective evaluation before emergencies arise. When strangulation occurs, modern emergency protocols, advanced imaging, and skilled surgical intervention work in tandem to restore perfusion, resect necrotic tissue, and reconstruct the abdominal wall. While emergency surgery carries higher morbidity and mortality compared to elective repair, the vast majority of patients who receive prompt treatment achieve successful outcomes and return to their normal activities.
The overarching message is unequivocal: hernias are progressive anatomical defects that will not resolve spontaneously. Proactive management, adherence to surgical recommendations, and a healthy lifestyle that minimizes abdominal strain remain the most effective defenses against strangulation. If you suspect a hernia or experience sudden changes in a known hernia, do not delay. Seek immediate emergency care, as in cases of strangulation, minutes and hours dictate the difference between a straightforward recovery and a fight for survival.
References
- Cleveland Clinic. (2025). Strangulated Hernia: Signs & Symptoms, Treatment.
- Healthline. (2017). Strangulated Hernia: Symptoms, Treatment, Outlook, and More.
- The British Hernia Centre. Strangulated Hernia.
- Mayo Clinic. Inguinal hernia - Symptoms & causes.
- Mayo Clinic. (2023). Hernia: Symptoms, Causes, and Complications.
- American College of Surgeons. (2025). A Catastrophic Complication: Strangulated Hiatal Hernia....

About the author
Michael O'Connell, DO, is a board-certified emergency medicine physician working as an attending physician at a busy Level I Trauma Center in Philadelphia, Pennsylvania. He also serves as a clinical instructor for medical residents and is active in wilderness medicine.