Amnesia vs. Dementia: Key Differences in Memory Loss

Key points
- Short-Term Memory: Holds small amounts of information for a few seconds or minutes, like remembering a phone number just long enough to dial it.
- Long-Term Memory: Stores information for days, years, or a lifetime. This includes explicit memories (facts, events) and implicit memories (skills, habits).
- Working Memory: A system for temporarily holding and manipulating information for complex tasks like problem-solving.
Memory is the diary we all carry with us, linking us to our past and shaping our identity. When memory begins to falter, two terms often come to mind: amnesia and dementia. While both involve memory problems, they are distinct conditions with different causes, symptoms, and outcomes. Understanding the difference between amnesia and dementia is crucial for accurate diagnosis and proper care. Globally, millions of individuals and their families navigate the complexities of cognitive decline, making public awareness and clinical literacy more important than ever. As our population ages, distinguishing between isolated memory impairment and broader neurodegenerative syndromes has become a cornerstone of modern neurological and geriatric practice.
 Image: An illustration of the human brain highlighting the hippocampus, a region crucial for forming new memories. Damage to this area is often associated with amnesia.
Image: An illustration of the human brain highlighting the hippocampus, a region crucial for forming new memories. Damage to this area is often associated with amnesia.
What is Memory and Why Do We Forget?
Before comparing amnesia and dementia, it's helpful to understand memory itself. Our brain uses several systems to store and retrieve information:
- Short-Term Memory: Holds small amounts of information for a few seconds or minutes, like remembering a phone number just long enough to dial it.
- Long-Term Memory: Stores information for days, years, or a lifetime. This includes explicit memories (facts, events) and implicit memories (skills, habits).
- Working Memory: A system for temporarily holding and manipulating information for complex tasks like problem-solving.
The hippocampus is vital for forming new long-term memories, while other areas like the cerebral cortex store them. Normal forgetting is a natural process; our brains filter out unnecessary information. Occasional lapses due to stress or fatigue are common and not typically a cause for concern. However, severe memory loss that interferes with daily life may signal a more serious issue like amnesia or dementia.
From a neurobiological perspective, memory operates through three fundamental stages: encoding, consolidation, and retrieval. Encoding is the initial processing of sensory input into a neural representation. During this phase, the brain determines which stimuli are worth retaining and which should be discarded. Consolidation follows, a complex and time-sensitive process where short-term traces are stabilized into long-term storage. This largely occurs during sleep, particularly during slow-wave and REM stages, where the hippocampus "replays" recent experiences to strengthen synaptic connections and transfer information to the neocortex for permanent storage. Retrieval is the final stage, involving the reactivation of stored neural networks when a cue or trigger is encountered.
Forgetting is rarely a failure of storage; more often, it results from retrieval failure, interference from competing memories, or natural synaptic pruning. Age-related memory changes, sometimes called age-associated memory impairment (AAMI), involve a gradual slowing of processing speed and mild word-finding difficulties. These changes do not significantly impair independence or daily functioning. In contrast, pathological memory loss disrupts the fundamental architecture of cognitive networks, leading to functional decline. Neurotransmitters like acetylcholine, glutamate, and dopamine play pivotal roles in synaptic plasticity and memory formation. Disruptions in these chemical pathways, whether from localized trauma, vascular compromise, or protein misfolding, can manifest as clinically significant cognitive deficits.
What is Amnesia?
Amnesia is a form of memory loss where a person cannot recall information, experiences, or events, or struggles to form new memories. It involves significant memory gaps that go beyond everyday forgetfulness.
Key Characteristics:
- Primary Symptom is Memory Loss: This can be retrograde amnesia (loss of past memories) or anterograde amnesia (inability to form new memories).
- Intelligence and Identity are Preserved: Individuals with amnesia typically retain their intelligence, personality, and sense of self. They know who they are but may have large gaps in their life story.
- Specific Causes: Amnesia is often caused by a specific event, such as:
- Traumatic brain injury (e.g., concussion)
- Stroke affecting memory centers
- Brain infections like encephalitis
- Lack of oxygen to the brain
- Severe alcohol abuse (Wernicke-Korsakoff syndrome)
- Psychological trauma (dissociative amnesia)
Diagnosis and Treatment: Diagnosis involves a medical history, cognitive tests, and brain imaging (MRI or CT scans) to identify damage. Treatment focuses on addressing the underlying cause and using cognitive rehabilitation to help the person develop coping strategies. Memory aids like calendars, notebooks, and smartphone apps are essential tools for managing daily life. The prognosis varies; some forms of amnesia are temporary, while others caused by severe brain damage can be permanent.
To fully grasp amnesia, clinicians categorize it into organic and dissociative subtypes. Organic amnesia stems from direct physiological injury or disease affecting brain structures like the medial temporal lobes, diencephalon, or basal forebrain. A classic example is Transient Global Amnesia (TGA), a sudden, temporary episode of memory loss that typically resolves within 24 hours without lasting neurological damage. Its exact cause remains debated but is thought to involve temporary hippocampal ischemia or venous flow disturbances. In contrast, dissociative amnesia is psychogenic, often triggered by severe emotional trauma or overwhelming stress. The brain essentially blocks access to painful memories as a protective mechanism, while procedural memory and cognitive faculties remain entirely intact.
Wernicke-Korsakoff syndrome represents a severe, alcohol-induced form of amnesia. Chronic alcohol abuse leads to thiamine (Vitamin B1) deficiency, causing acute encephalopathy (Wernicke’s) that, if untreated, progresses to permanent Korsakoff psychosis. Patients exhibit profound anterograde amnesia and frequently "confabulate," unconsciously fabricating memories to fill cognitive gaps. Neuroimaging typically reveals atrophy of the mammillary bodies and medial thalamus.
In clinical practice, amnesia management requires a multidisciplinary approach. Neurologists and neuropsychologists work together to map cognitive deficits. Cognitive rehabilitation therapy employs errorless learning, spaced retrieval techniques, and environmental modification to maximize remaining function. For instance, establishing rigid daily routines, using color-coded labels, and implementing digital reminder systems can dramatically improve autonomy. Family education is equally vital, as caregivers must learn to avoid constant testing of memory, which can increase patient anxiety and depression. Instead, focusing on preserved skills, emotional connection, and validation therapy fosters better psychological outcomes. While permanent organic amnesia currently has no pharmacological cure, emerging research into hippocampal neurogenesis and targeted neurotrophic factors offers hope for future restorative therapies.
What is Dementia?
Dementia is not a single disease but an umbrella term for a syndrome characterized by a progressive decline in multiple cognitive abilities—including memory, thinking, and behavior—severe enough to interfere with daily life.
Key Characteristics:
- Widespread Cognitive Decline: While memory loss (especially of recent events) is a common early symptom, dementia also affects language, judgment, reasoning, and problem-solving.
- Progressive Worsening: Most types of dementia, such as Alzheimer's disease, are progressive, meaning symptoms start slowly and worsen over time.
- Impact on Daily Functioning: As the condition progresses, individuals lose the ability to perform everyday tasks independently, such as managing finances, cooking, or personal hygiene.
- Common Causes: Dementia is caused by diseases that damage brain cells. The most common types include:
- Alzheimer’s Disease: The most common cause, characterized by amyloid plaques and tau tangles in the brain.
- Vascular Dementia: Caused by reduced blood flow to the brain, such as from strokes.
- Lewy Body Dementia (LBD): Involves abnormal protein deposits and often includes hallucinations and movement problems.
- Frontotemporal Dementia (FTD): Affects the frontal and temporal lobes, leading to significant changes in personality and behavior.
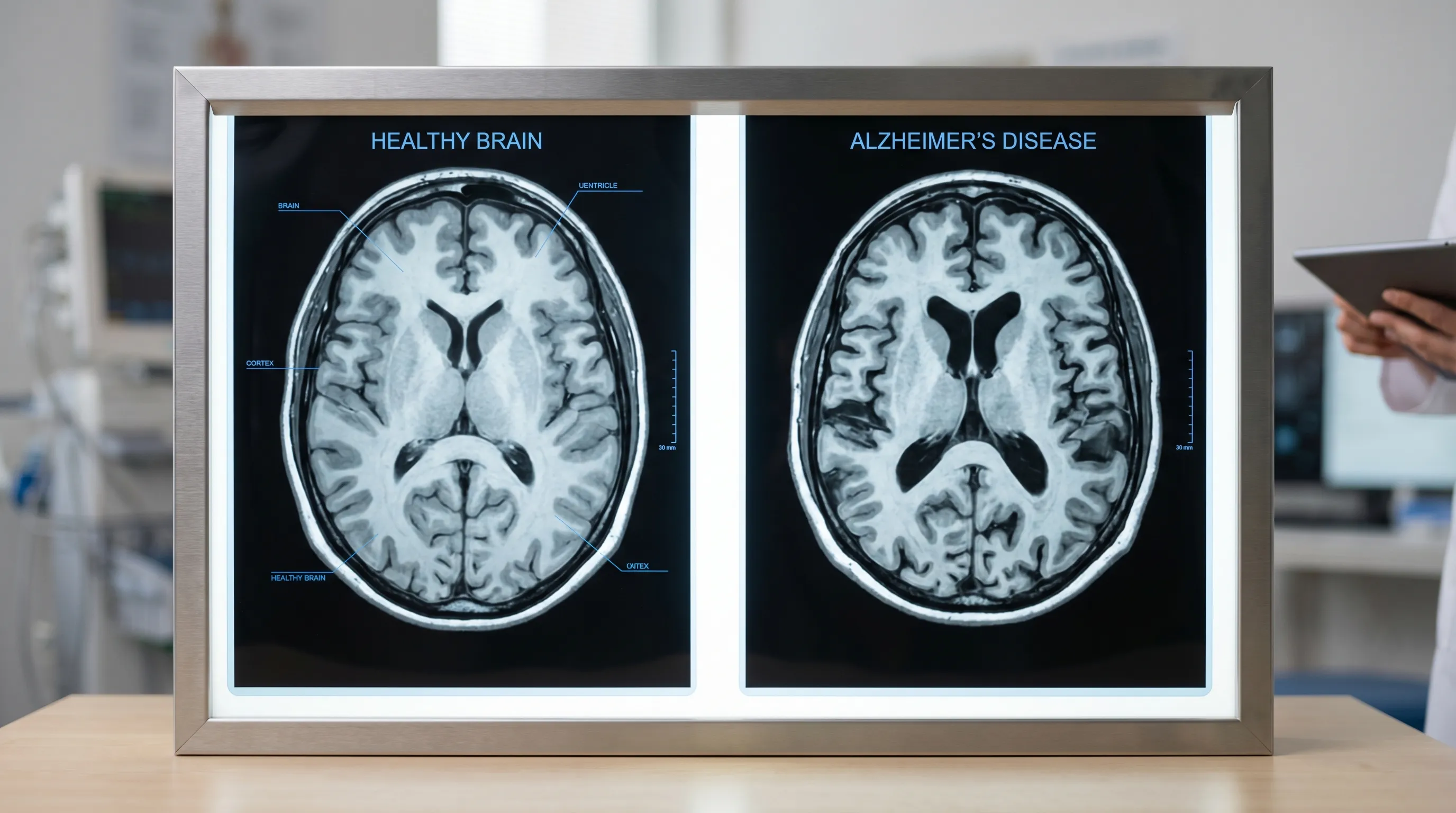 Image: Comparison of a healthy brain (left) and a brain with advanced Alzheimer’s disease (right). The widespread brain cell loss (atrophy) in Alzheimer's leads to global cognitive decline. Source: National Institute on Aging (NIA)
Image: Comparison of a healthy brain (left) and a brain with advanced Alzheimer’s disease (right). The widespread brain cell loss (atrophy) in Alzheimer's leads to global cognitive decline. Source: National Institute on Aging (NIA)
Diagnosis and Treatment: Diagnosis is complex and involves a medical assessment, cognitive and neurological exams, lab tests, and brain imaging. While there is no cure for most progressive dementias, treatments can help manage symptoms. Medications like cholinesterase inhibitors and memantine can temporarily improve cognitive function. Lifestyle changes, therapy, and strong caregiver support are crucial for maintaining quality of life.
The pathophysiology of dementia varies significantly by subtype, requiring precision diagnostics and tailored management. Alzheimer's disease accounts for 60-80% of cases and involves the pathological accumulation of extracellular beta-amyloid plaques and intracellular neurofibrillary tau tangles. These proteins disrupt neuronal communication, trigger chronic neuroinflammation, and ultimately lead to widespread synaptic failure and cortical atrophy. The disease typically progresses through predictable clinical stages: preclinical (asymptomatic but biologically active), mild cognitive impairment (MCI), mild dementia, moderate dementia, and severe dementia. Recent advances in biomarker testing now allow clinicians to detect amyloid and tau pathology through cerebrospinal fluid analysis, PET imaging, and increasingly, highly sensitive blood tests like p-tau217, enabling earlier and more accurate diagnosis long before functional decline occurs.
Vascular dementia, the second most common form, results from compromised cerebral blood flow due to large-vessel strokes, microvascular disease, or hypoperfusion. Its clinical presentation can be stepwise or gradual, depending on the vascular insult. Strict management of hypertension, diabetes, atrial fibrillation, and hyperlipidemia is paramount to halting further progression. Lewy Body Dementia is distinguished by alpha-synuclein aggregates and presents with a fluctuating cognitive profile, vivid visual hallucinations, REM sleep behavior disorder, and parkinsonian motor symptoms. Patients with LBD are highly sensitive to antipsychotic medications, requiring careful pharmacological navigation. Frontotemporal dementia predominantly strikes younger individuals (40s-60s) and manifests as profound behavioral disinhibition, apathy, or primary progressive aphasia, often preceding memory impairment by years.
Pharmacological management focuses on symptom modulation and slowing decline. Cholinesterase inhibitors (donepezil, rivastigmine, galantamine) work by increasing acetylcholine availability in synaptic clefts, temporarily enhancing attention, memory, and executive function. Memantine regulates glutamate activity to prevent excitotoxicity and is typically introduced in moderate to severe stages. Recently, disease-modifying therapies targeting amyloid pathology (e.g., lecanemab, donanemab) have received accelerated FDA approval, demonstrating modest but measurable slowing of cognitive decline in early-stage Alzheimer's patients, though they require careful monitoring for amyloid-related imaging abnormalities (ARIA), such as brain swelling or microhemorrhages.
Non-pharmacological interventions are equally critical. Cognitive stimulation therapy, reminiscence therapy, music therapy, and structured physical activity programs have demonstrated consistent benefits in behavioral and psychological symptom management. Environmental safety modifications—such as removing trip hazards, installing grab bars, using stove auto-shutoff devices, and implementing GPS trackers for wandering prevention—are essential for patient safety. As dementia advances, palliative care principles should be integrated early to address advance directives, nutritional support, and caregiver burden. Comprehensive dementia care requires a collaborative team including neurologists, geriatricians, occupational therapists, speech-language pathologists, social workers, and dedicated family caregivers.
Amnesia vs. Dementia: Key Differences
While both conditions affect memory, they are fundamentally different. Here’s a summary of the key distinctions.
| Aspect | Amnesia | Dementia |
|---|---|---|
| Scope of Symptoms | Primarily affects memory. Other cognitive functions are often intact. | Affects memory plus other cognitive functions like language, reasoning, and judgment. |
| Onset | Usually sudden, linked to a specific event (e.g., injury, trauma). | Typically gradual and progressive, worsening over months or years. |
| Progression | Often non-progressive. It can be stable, improve, or be temporary. | Progressive in most cases. Symptoms worsen over time. |
| Causes | Brain injury, stroke, infection, psychological trauma. | Neurodegenerative diseases (e.g., Alzheimer's), vascular issues, other chronic conditions. |
| Age of Onset | Can occur at any age. | Most common in older adults (65+), though early-onset forms exist. |
| Impact on Daily Life | Can be managed with coping strategies and memory aids; independence is often possible. | Leads to a growing need for assistance, eventually resulting in full dependence on caregivers. |
This comparative framework is invaluable for both clinical triage and family education. When patients or loved ones present with isolated memory deficits following a discrete incident like a fall or surgery, the clinical suspicion naturally points toward amnesic syndromes. Conversely, a slow, insidious decline across multiple cognitive domains, accompanied by personality shifts or executive dysfunction, strongly aligns with dementia pathologies. The table above underscores that prognosis and care trajectories diverge sharply: amnesia often requires targeted rehabilitation and compensatory strategy development, whereas dementia necessitates long-term care planning, progressive symptom management, and extensive psychosocial support networks. Recognizing these distinctions prevents misdiagnosis, reduces unnecessary anxiety, and ensures patients are routed to the appropriate specialty services promptly.
Overlapping Aspects and Connections
It's important to recognize that dementia includes memory loss as a core symptom. In this sense, a person with dementia experiences a form of amnesia as part of their broader condition. However, a person with pure amnesia does not have the other cognitive impairments seen in dementia.
Furthermore, some conditions can mimic dementia. For example, severe depression can cause "pseudodementia," where memory and concentration improve once the depression is treated. A thorough medical evaluation is essential to distinguish between these conditions.
Beyond pseudodementia, numerous reversible or treatable medical conditions can present with amnestic or dementia-like symptoms. Metabolic disturbances (e.g., hypothyroidism, vitamin B12 deficiency, electrolyte imbalances), medication side effects (particularly anticholinergics, benzodiazepines, and polypharmacy in older adults), sleep apnea, chronic pain, and autoimmune encephalitis can all masquerade as primary cognitive disorders. Mixed dementia, where Alzheimer’s pathology coexists with vascular brain injury, is exceptionally common and explains why many patients exhibit features of both gradual decline and stepwise deterioration. Additionally, chronic traumatic encephalopathy (CTE), associated with repetitive head impacts in athletes and military personnel, blurs the lines between acquired amnesia and progressive neurodegeneration.
Clinical differentiation hinges on comprehensive neuropsychological testing, which maps specific cognitive domains and identifies characteristic deficit patterns. For instance, amnesic patients typically score normally on executive function, language, and visuospatial tasks, whereas dementia patients show multi-domain impairment. Brain imaging further clarifies: focal lesions point to amnesia, while diffuse atrophy, white matter hyperintensities, or hypometabolism patterns indicate neurodegeneration or vascular disease. A meticulous history, often supplemented by collateral interviews from family members, remains the most powerful diagnostic tool. Clinicians must also screen for sensory deficits; untreated hearing or vision loss frequently exacerbates cognitive complaints by increasing mental effort and social isolation, creating a false impression of rapid decline. Addressing these underlying or mimicking factors is a cornerstone of geriatric neurology and can dramatically alter patient outcomes.
 Image: The health of our brain cells and their connections is crucial for memory. In dementia, these connections are progressively lost, while in amnesia, a specific area of the memory network may be damaged.
Image: The health of our brain cells and their connections is crucial for memory. In dementia, these connections are progressively lost, while in amnesia, a specific area of the memory network may be damaged.
When to Seek Professional Help
If you or a loved one are experiencing significant memory problems, whether sudden or gradual, it is crucial to consult a doctor. Early diagnosis can help identify reversible causes, allow for early intervention to manage symptoms, and provide time for future planning. A healthcare professional, such as a neurologist, can perform the necessary assessments to determine the underlying cause of the memory loss.
Certain red flags warrant immediate medical attention. Sudden confusion, disorientation, slurred speech, facial drooping, or weakness on one side of the body could indicate a stroke or acute neurological emergency requiring emergency department evaluation. Memory loss accompanied by high fever, severe headache, stiff neck, or recent head trauma also demands urgent assessment. For non-emergent but concerning symptoms, schedule a primary care visit if you notice: repeating the same questions within short intervals; getting lost in familiar neighborhoods; mismanaging medications or finances; noticeable personality or mood changes; difficulty following conversations or finding common words; or neglecting personal hygiene and safety.
To maximize the value of a clinical consultation, prepare thoroughly beforehand. Maintain a symptom journal documenting specific memory lapses, their frequency, triggers, and impact on daily routines. Bring a complete list of all prescription medications, over-the-counter drugs, and supplements, as interactions are a common culprit. Invite a close family member or friend who has observed the changes firsthand, as patients with cognitive impairment often lack insight into their deficits (anosognosia). Expect a comprehensive workup that includes a physical and neurological exam, standardized cognitive screening (such as the MoCA or MMSE), blood tests (CBC, metabolic panel, thyroid function, B12/folate, syphilis/HIV screening if indicated), and neuroimaging. Depending on initial findings, referral to a memory disorders clinic, neuropsychologist, or geriatric psychiatrist may follow. Early engagement with healthcare providers not only optimizes medical management but also opens doors to clinical trials, community resources, and vital legal/financial planning while decision-making capacity remains intact.
Prevention and Brain Health
While many causes of amnesia are not preventable (e.g., accidents), research suggests that you can reduce your risk of some types of dementia through a healthy lifestyle.
- Stay Physically Active: Regular exercise improves blood flow to the brain.
- Eat a Healthy Diet: Diets like the Mediterranean diet, rich in fruits, vegetables, and healthy fats, are linked to better brain health.
- Remain Mentally and Socially Engaged: Challenge your mind with puzzles, reading, learning new skills, and maintaining social connections.
- Manage Cardiovascular Health: Controlling blood pressure, cholesterol, and diabetes is vital for protecting your brain.
- Protect Your Head: Wear helmets and take precautions to prevent falls and head injuries.
The evidence supporting lifestyle-driven brain resilience has grown exponentially, largely driven by landmark studies like the FINGER (Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability), which demonstrated that multidomain lifestyle interventions can reduce cognitive decline by up to 25-30% in at-risk older adults. Physical activity, particularly aerobic exercise like brisk walking, swimming, or cycling, stimulates the release of brain-derived neurotrophic factor (BDNF), a protein that promotes neurogenesis, synaptic plasticity, and vascular health. The American Heart Association recommends at least 150 minutes of moderate-intensity aerobic activity weekly, supplemented with strength training twice weekly.
Dietary patterns profoundly influence neuroinflammation and oxidative stress. The MIND diet (Mediterranean-DASH Intervention for Neurodegenerative Delay), which emphasizes leafy greens, berries, nuts, whole grains, fish, and olive oil while limiting red meat, butter, cheese, pastries, and fried foods, has shown robust associations with slower cognitive aging and reduced Alzheimer’s pathology. Key nutrients like omega-3 fatty acids (DHA), polyphenols, and B vitamins support myelin integrity and reduce homocysteine levels, an independent risk factor for cognitive decline.
Cognitive and social engagement build "cognitive reserve," a buffer that allows the brain to compensate for pathology by utilizing alternative neural networks. Lifelong learning, mastering complex skills, volunteering, and maintaining deep social connections reduce chronic stress and cortisol levels, protecting hippocampal volume. Sleep is another non-negotiable pillar: during deep sleep, the glymphatic system clears metabolic waste products, including beta-amyloid, from the brain. Treating sleep apnea and prioritizing 7-9 hours of quality rest nightly is one of the most potent neuroprotective strategies available. Finally, aggressive management of cardiovascular risk factors—maintaining blood pressure below 130/80, optimizing glycemic control, quitting smoking, and managing stress through mindfulness or therapy—directly preserves cerebral vasculature. Brain health is not isolated; it is inextricably linked to systemic wellness, making preventive neurology a lifelong, proactive commitment.
Conclusion
Amnesia and dementia are two distinct conditions that both impact memory. Amnesia is a memory disorder, often with a sudden onset, where other cognitive functions remain intact. Dementia is a progressive syndrome involving the decline of multiple cognitive abilities that ultimately affects a person's ability to live independently.
Understanding these differences is the first step toward proper diagnosis, management, and support. With advancements in research and a growing emphasis on brain health, there is hope for better treatments and improved quality of life for individuals facing these challenges. The rapid evolution of biomarker technology, disease-modifying therapies, and precision neurology is transforming cognitive care from purely symptomatic management to proactive intervention. Whether navigating the sudden disruptions of amnesia or the gradual journey of dementia, patients, families, and clinicians are better equipped than ever to build compassionate, evidence-based care pathways. By demystifying these conditions and championing preventive brain health, we can foster a society that values cognitive resilience and supports those experiencing memory challenges with dignity and informed care.
Video Resources
- What is Dementia? (YouTube): An animated video from the Alzheimer's Society that clearly explains what dementia is and how it differs from normal aging.
- The Man with the 7 Second Memory (YouTube): A documentary clip on Clive Wearing, providing a powerful look into the reality of living with severe amnesia.
Additional Resources & References
- Mayo Clinic: Amnesia: Symptoms and causes
- Mayo Clinic: Dementia: Symptoms and causes
- Alzheimer’s Association: What Is Dementia?
- National Institute on Aging (NIA): Understanding Memory Loss
- World Health Organization (WHO): Dementia Fact Sheet
Frequently Asked Questions
Can amnesia turn into dementia over time?
No, amnesia does not transform into dementia. They have fundamentally different underlying mechanisms and clinical trajectories. Amnesia typically results from an acute, focal event such as trauma, stroke, hypoxia, or severe psychological stress, and its symptoms usually stabilize or improve with rehabilitation and time. Dementia, on the other hand, is a chronic, progressive neurodegenerative or vascular condition that gradually destroys brain cells across multiple regions. While both involve memory loss, having an amnesic syndrome does not increase your biological risk for developing Alzheimer's disease or other dementias later in life. If someone with pre-existing amnesia begins showing progressive decline in other cognitive domains, it warrants a separate clinical evaluation for a new, independent neurological condition.
Are there medications that cure or completely reverse amnesia or dementia?
Currently, there are no medications that provide a complete cure or reversal for most cases of organic amnesia or progressive dementia. Treatment strategies are symptom-focused and disease-modifying where applicable. For dementia, drugs like cholinesterase inhibitors and memantine can temporarily enhance neurotransmission and slow functional decline, while newer immunotherapies (e.g., lecanemab) modestly slow amyloid accumulation in early Alzheimer's disease but do not restore lost neurons. For amnesia, no pharmacological agents can regenerate scarred or necrotic brain tissue. Management relies heavily on addressing reversible contributors (e.g., vitamin deficiencies, medication side effects, metabolic issues), cognitive rehabilitation, and compensatory environmental strategies. Research into neuroplasticity enhancers, stem cell therapies, and targeted protein clearance is ongoing, but clinical cures remain a future horizon.
How do doctors definitively differentiate between amnesia and dementia in a clinical setting?
Differentiation relies on a comprehensive diagnostic protocol. Clinicians begin with a detailed patient and collateral history to establish onset patterns (sudden vs. gradual) and progression. Standardized neuropsychological testing is the gold standard: amnesia shows isolated deficits in episodic memory (both encoding and retrieval) with preserved executive function, language, and visuospatial skills. Dementia demonstrates broad-spectrum impairment across at least two domains (memory plus language, praxis, gnosia, or executive function). Neuroimaging (MRI or CT) reveals focal lesions in the hippocampus, thalamus, or basal forebrain in amnesia, whereas dementia shows diffuse cortical atrophy, specific lobar shrinkage (e.g., temporal/parietal in AD, frontal in FTD), or extensive white matter disease. Advanced biomarkers (CSF analysis, amyloid/tau PET scans) further confirm or exclude neurodegenerative pathology. Blood tests rule out reversible metabolic or infectious mimics, ensuring an accurate diagnosis.
What specific daily strategies help caregivers support someone with amnesia versus someone with dementia?
Caregiving approaches must align with the condition's nature. For amnesia, strategies focus on externalizing memory and building routines since intelligence and self-awareness remain intact. Caregivers should implement structured schedules, use visible calendars, pill organizers, labeled storage, and smartphone alarms. Teaching the patient to use memory notebooks or voice recorders empowers independence. Emotional support centers on validating frustration without treating the patient as incompetent. For dementia, care must adapt to progressive cognitive and functional decline, often requiring safety modifications and simplified communication. Strategies include reducing environmental clutter, using short, direct sentences, maintaining consistent routines, and managing behavioral symptoms non-pharmacologically first. As dementia advances, caregivers shift from enabling independence to ensuring safety, dignity, and comfort, frequently requiring respite care, professional home health aides, and eventually specialized memory care facilities. Joining condition-specific support groups is highly recommended for both caregiver types.
Is memory loss in younger adults (under 60) always a sign of dementia?
Absolutely not. Memory complaints in younger adults are far more likely to stem from stress, anxiety, depression, sleep deprivation, hormonal imbalances (e.g., thyroid dysfunction, perimenopause), medication side effects, or nutritional deficiencies (B12, iron, vitamin D) than from neurodegenerative dementia. While early-onset dementia (before age 65) does exist, it accounts for less than 10% of all dementia cases and is often linked to specific genetic mutations (e.g., APP, PSEN1, PSEN2, or MAPT genes). When younger adults experience persistent cognitive fog or memory lapses, a thorough medical workup should prioritize reversible lifestyle and metabolic factors first. Chronic stress elevates cortisol, which can temporarily impair hippocampal function, while untreated sleep apnea severely disrupts memory consolidation. Addressing these root causes typically restores cognitive function, underscoring why comprehensive evaluation is essential before assuming a progressive neurodegenerative diagnosis.
About the author
David Chen, DO, is a board-certified neurologist specializing in neuro-oncology and stroke recovery. He is the director of the Comprehensive Stroke Center at a New Jersey medical center and has published numerous articles on brain tumor treatment.