Can Stress Cause Vertigo? Understanding the Link and Finding Relief

Key points
- Spinning or whirling sensation (either subjective, feeling you are moving, or objective, feeling the room is moving)
- Loss of balance or unsteadiness, often worsening with head turns or positional changes
- Nausea or vomiting, driven by the close neural connection between the vestibular nuclei and the vomiting center in the medulla
- Abnormal rapid eye movements (nystagmus), which occur as the brain attempts to compensate for the false motion signals
Feeling dizzy or lightheaded during a stressful period is a common experience. You might feel like the room is spinning after an anxiety-provoking event, leaving you to wonder: can stress actually cause vertigo?
The short answer is yes, but with important medical nuance. While acute psychological stress does not directly create vestibular pathology in a completely healthy ear, it acts as a powerful physiological modulator that can trigger, worsen, or prolong vertigo episodes. The mind-body connection is particularly strong in the vestibular system, which is highly sensitive to changes in neurotransmitters, blood flow, and hormonal fluctuations. For individuals with an underlying predisposition or a pre-existing inner ear condition, stress can serve as the tipping point that transforms mild imbalance into disabling vertigo.
Vertigo is a specific type of dizziness where you feel that you or your surroundings are moving when they aren't. While it's typically linked to inner ear problems, stress and anxiety can produce a variety of physical symptoms, including dizziness and balance issues. Research shows that chronic stress can worsen existing inner ear (vestibular) disorders and may even trigger vertigo episodes in some people. Understanding the neurobiological pathways behind this phenomenon is essential for accurate diagnosis, effective treatment, and long-term symptom management.
This guide explores the connection between stress and vertigo, its causes, symptoms, diagnostic considerations, and evidence-based strategies for finding lasting relief. By bridging the gap between psychological stressors and vestibular physiology, we can develop a comprehensive approach to managing this complex condition.
What Is Vertigo?
Vertigo is the false sensation of movement. People often describe it as feeling like they are spinning or the world is whirling around them. It is a symptom of an underlying condition, not a disease itself. Vertigo stems from a disturbance in the body's balance system, which includes the inner ear and the parts of the brain that process spatial information. To fully grasp how stress interferes with equilibrium, it helps to understand the anatomy and physiology of the vestibular apparatus.
The human balance system relies on the seamless integration of three primary sensory inputs: the vestibular system (located in the inner ear), vision, and proprioception (sensory feedback from muscles and joints). The inner ear contains two main functional units: the semicircular canals, which detect rotational head movements, and the otolith organs (utricle and saccule), which sense linear acceleration and gravity relative to head position. These structures are filled with a specialized fluid called endolymph. When your head moves, the fluid shifts, bending microscopic hair cells that convert mechanical energy into electrical signals. These signals travel via the vestibulocochlear nerve to the brainstem, cerebellum, and vestibular cortex, where they are processed and matched against visual and proprioceptive data.
When this sensory integration process fails or receives conflicting signals, the brain misinterprets your position in space, resulting in the illusion of motion. Stress disrupts this delicate process through multiple pathways, including altered neurotransmitter release, changes in inner ear blood flow, and heightened sensory processing in the central nervous system. This explains why psychological tension often manifests as physical dizziness, even in the absence of structural ear damage.
Key signs of vertigo include:
- Spinning or whirling sensation (either subjective, feeling you are moving, or objective, feeling the room is moving)
- Loss of balance or unsteadiness, often worsening with head turns or positional changes
- Nausea or vomiting, driven by the close neural connection between the vestibular nuclei and the vomiting center in the medulla
- Abnormal rapid eye movements (nystagmus), which occur as the brain attempts to compensate for the false motion signals
It's important to distinguish vertigo from other types of dizziness, such as lightheadedness (feeling faint, often related to cardiovascular or respiratory issues) or disequilibrium (feeling off-balance without spinning, often linked to neuropathy or cerebellar dysfunction). While stress more commonly causes lightheadedness or a floating sensation, it can absolutely trigger or worsen true rotational vertigo, particularly through central nervous system sensitization and exacerbation of peripheral vestibular conditions.
What Causes Vertigo?
Vertigo is most often caused by a problem in the inner ear or the brain. Understanding these causes helps clarify how stress can play a role. Vestibular disorders are broadly categorized into peripheral (originating in the inner ear or vestibular nerve) and central (originating in the brainstem or cerebellum) etiologies. The majority of vertigo cases are peripheral, and these are the conditions most frequently influenced by psychological stress.
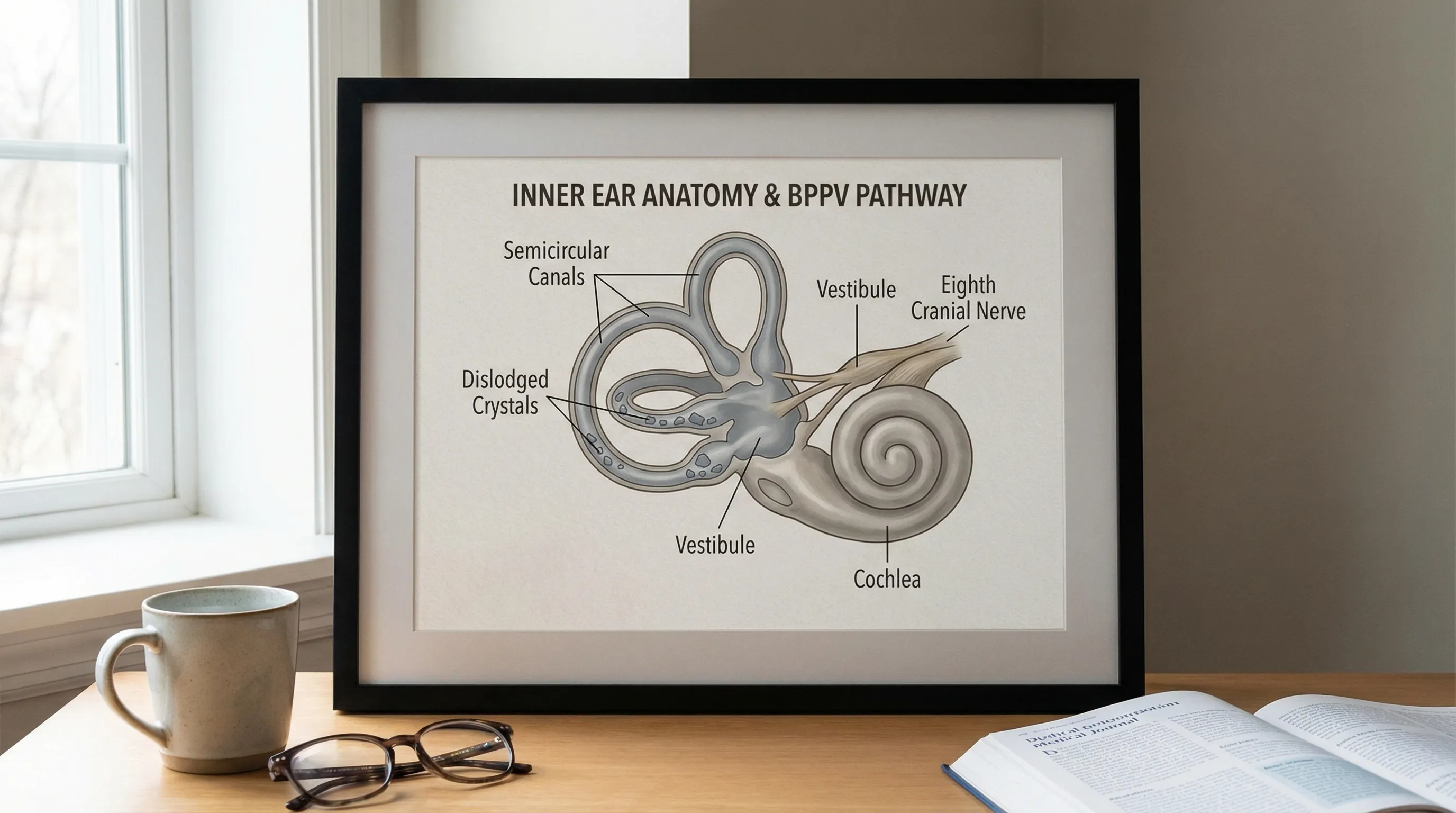
Benign Paroxysmal Positional Vertigo (BPPV)
BPPV is the most common cause of vertigo, accounting for roughly 20% to 30% of all clinical dizziness cases. It occurs when tiny calcium carbonate crystals (otoconia) in the utricle become dislodged and migrate into the semicircular canals, most commonly the posterior canal. When you move your head, these free-floating crystals shift the endolymph abnormally, sending false rotational signals to the brain. This causes brief but intense episodes of vertigo, typically lasting less than 60 seconds, triggered by specific head movements such as rolling over in bed, looking up, or bending forward.
While BPPV itself is a mechanical issue, stress significantly impacts patient experience and recovery. High cortisol and sympathetic arousal can amplify symptom perception, making brief mechanical episodes feel prolonged and terrifying. Additionally, stress-induced sleep disturbances and neck muscle tension can alter cervical proprioception, further confusing the brain's balance network. Some research also suggests that chronic stress and poor sleep quality may impair the natural clearance of dislodged crystals, indirectly contributing to BPPV recurrence.
Meniere’s Disease
Meniere's disease is an inner ear disorder characterized by episodic peripheral vertigo, sensorineural hearing loss, tinnitus, and aural fullness. The underlying pathology is believed to be endolymphatic hydrops—an abnormal accumulation of endolymphatic fluid within the membranous labyrinth. As fluid pressure builds, it distorts the delicate structures of the cochlea and vestibular organs, leading to spontaneous vertigo attacks that can last from 20 minutes to 12 hours. According to Johns Hopkins Medicine, emotional stress is a known trigger that can bring on these episodes.
The stress-Meniere's connection is well-documented. Psychological stress activates the hypothalamic-pituitary-adrenal (HPA) axis and sympathetic nervous system, which can alter inner ear blood flow and disrupt endolymphatic fluid homeostasis. Vasoconstriction from stress hormones may reduce microcirculation in the stria vascularis, impairing fluid absorption and exacerbating hydrops. Consequently, patients with Meniere's disease frequently report that high-pressure periods, work-related tension, or emotional trauma directly precede debilitating vertigo flare-ups.
Vestibular Neuritis and Labyrinthitis
These conditions involve acute inflammation of the inner ear or the vestibular nerve connecting it to the brain, typically following a viral infection. Vestibular neuritis affects only the balance nerve, causing severe vertigo, nausea, and imbalance without hearing changes. Labyrinthitis involves both the balance and hearing structures, resulting in similar vertigo symptoms accompanied by tinnitus and hearing loss. They can cause a sudden, intense vertigo that lasts for days, gradually improving as the brain compensates.
While an infection is the root cause, high levels of stress can profoundly impact recovery. Chronic stress suppresses immune function, potentially prolonging viral shedding or delaying tissue healing. More importantly, stress interferes with vestibular compensation—the neuroplastic process by which the brain recalibrates to asymmetric inner ear signals. Patients who maintain high anxiety levels during the acute phase often experience slower functional recovery, prolonged gait instability, and a higher risk of developing chronic postural symptoms. Stress management during the acute window is therefore a critical component of rehabilitation.
Vestibular Migraine
Vestibular migraines are the second most common cause of episodic vertigo. Unlike typical migraines that primarily feature headache, vestibular migraines present with dizziness, motion sensitivity, and balance disruption. Episodes can last minutes to days and may occur with or without head pain. The pathophysiology involves abnormal neuronal excitability, cortical spreading depression, and brainstem dysregulation affecting vestibular nuclei processing. Stress is a well-established trigger for migraines. For individuals prone to vestibular migraines, managing stress is a key part of preventing vertigo episodes, as noted by the American Migraine Foundation.
Stress alters serotonin and glutamate neurotransmission, both of which play pivotal roles in migraine pathogenesis. Elevated cortisol levels can lower the threshold for neuronal firing in the vestibular brainstem, making patients hyper-responsive to normal motion stimuli. This explains why many vestibular migraine sufferers experience "visual vertigo" or feel dizzy in visually complex environments (like grocery store aisles) during periods of psychological strain.
Other Causes
Vertigo can also be caused by a variety of other systemic, neurological, and pharmacological factors:
- Medication side effects: Ototoxic drugs (certain antibiotics, loop diuretics, high-dose aspirin) can damage inner ear hair cells. Antihypertensives, sedatives, and antidepressants can cause orthostatic dizziness or alter central vestibular processing.
- Sudden drops in blood pressure (hypotension): Orthostatic hypotension or vasovagal syncope can cause presyncopal dizziness, often exacerbated by stress-induced autonomic dysregulation.
- Dehydration or low blood sugar: Electrolyte imbalances and hypoglycemia disrupt neuronal function and cerebral perfusion, leading to lightheadedness and impaired balance control.
- Head injuries: Post-concussion syndrome frequently includes vertigo due to peripheral vestibular trauma, cervical spine disruption, or mild traumatic brain injury affecting central integration pathways.
- Neurological conditions: Stroke, transient ischemic attack (TIA), multiple sclerosis, or acoustic neuroma can cause central vertigo. These require urgent evaluation, especially when accompanied by focal neurological deficits.
How Stress Affects the Body and Balance
When you perceive a threat, your body initiates the "fight-or-flight" response, releasing stress hormones like adrenaline and cortisol. This evolutionary survival mechanism is designed for short-term physical emergencies, but chronic psychological stress keeps these pathways perpetually activated. The resulting neuroendocrine and autonomic shifts directly affect your sense of balance through multiple interconnected physiological routes.
The Fight-or-Flight Response and Dizziness
During the stress response, several things happen that can make you feel dizzy or trigger vertigo-like sensations:
- Rapid Breathing (Hyperventilation): Anxiety often leads to shallow, rapid chest breathing. This blows off excessive carbon dioxide, causing respiratory alkalosis. The resulting alkaline shift increases blood vessel constriction in the brain (cerebral vasoconstriction) and alters calcium binding, leading to lightheadedness, tingling in the extremities, and a profound sense of floating or detachment.
- Blood Pressure and Heart Rate Spikes: A surge of adrenaline and noradrenaline increases cardiac output and peripheral vascular resistance. While this ensures muscle readiness, it can temporarily disrupt the precise autoregulation required for stable cerebral and labyrinthine blood flow. The inner ear's labyrinthine artery has no collateral circulation, making it exceptionally vulnerable to microvascular fluctuations.
- Muscle Tension and Cervical Impact: Chronic stress causes sustained contraction in the trapezius, sternocleidomastoid, and suboccipital muscles. These muscles are densely packed with proprioceptors that constantly inform the brain about head and neck position. Abnormal cervical tension sends mismatched signals to the vestibular nuclei, contributing to cervicogenic dizziness or exacerbating existing balance disorders.
- Neurotransmitter Imbalance: Stress depletes serotonin and GABA while increasing glutamate and cortisol. Since serotonin and GABA act as inhibitory modulators in the vestibular brainstem, their depletion can lead to central vestibular hyperexcitability, making you feel unsteady even when your ears are functioning normally.
How Stress Can Trigger Underlying Conditions
For many people, stress acts as a trigger rather than a direct cause. If you have a pre-existing vestibular disorder, the physiological cascade of chronic anxiety can tip the scales and initiate an episode of vertigo or significantly lower your threshold for symptom onset.
- Meniere’s Disease: Stress-induced cortisol fluctuations and sympathetic tone can disrupt endolymphatic fluid resorption, directly triggering hydrops-related vertigo attacks. Many patients track their flare-ups alongside major life stressors or acute anxiety spikes.
- Vestibular Migraine: The migraine brain is inherently hyperexcitable. Stress lowers the activation threshold for cortical spreading depression and brainstem vestibular nuclei firing. For susceptible individuals, even moderate emotional tension can precipitate hours or days of motion sensitivity and spinning.
- BPPV: While stress doesn't physically dislodge otoconia, the heightened anxiety, sleep fragmentation, and muscle tension from chronic stress can make BPPV episodes feel more severe, increase fall risk due to delayed postural adjustments, and slow the brain's natural adaptation to residual imbalance.
The Anxiety-Vertigo Cycle
Vertigo can be a deeply disorienting and frightening experience, often leading to anticipatory anxiety about future episodes. This psychological burden fundamentally alters how the brain processes balance information, creating a self-perpetuating feedback loop known as the anxiety-vertigo cycle. When you constantly fear dizziness, your nervous system remains in a heightened state of alert. This leads to hypervigilance, where the brain amplifies normal, minor fluctuations in balance into perceived threats.
This maladaptive sensory processing is central to a condition called Persistent Postural-Perceptual Dizziness (PPPD), a functional vestibular disorder formally recognized by the Barany Society. PPPD develops when the brain fails to return to baseline sensory integration after an initial vertigo event. Chronic anxiety and fear-avoidance behaviors rewire the vestibular cortex to over-rely on visual cues and suppress efficient vestibular processing. Patients experience chronic non-spinning dizziness, rocking, or swaying that worsens in upright positions, complex environments, or during stress. Breaking this cycle requires targeted neurological rehabilitation alongside psychological intervention to recalibrate sensory weighting and reduce fear-driven autonomic arousal.
Symptoms of Stress-Related Vertigo
Recognizing the specific presentation of stress-related dizziness versus purely mechanical vestibular pathology can guide appropriate treatment. If stress is contributing to your vertigo or dizziness, you may notice distinct patterns in timing, associated symptoms, and symptom quality.
- A spinning, swaying, or floating feeling that closely correlates with periods of high psychological demand or anxiety. Symptoms may begin abruptly during a stressful confrontation or gradually build over days of sustained pressure.
- Dizziness accompanied by classic autonomic and psychological symptoms, such as a racing heart, palpitations, sweating, shallow breathing, chest tightness, or shortness of breath. These often point toward a panic-driven or anxiety-mediated vestibular response.
- A persistent background sensation of unsteadiness, "brain fog," or feeling disconnected from reality (derealization). Unlike acute vertigo that comes in sharp attacks, stress-related dizziness often presents as a continuous, low-grade haze that fluctuates in intensity.
- Tension headaches, jaw clenching, or severe neck/shoulder pain that coincides with balance disturbances. This somatic clustering strongly suggests a musculoskeletal or cervicogenic component driven by chronic stress.
- Worsening symptoms in visually demanding or socially stressful environments. Many patients report feeling significantly worse in busy supermarkets, scrolling on screens, navigating crowded spaces, or during public speaking. This visual and situational dependence is a hallmark of central sensitization and PPPD.
- An increase in vertigo episodes or prolonged recovery time if you have a known condition like Meniere’s disease, vestibular neuritis, or vestibular migraines. Stress doesn't just trigger attacks; it delays the brain's natural compensation mechanisms.
It is crucial to understand that stress does not produce "fake" symptoms. The dizziness, nausea, and imbalance are real physiological experiences. The difference lies in their origin: while BPPV stems from mechanical debris in the canal, stress-related vertigo stems from altered neural processing, autonomic dysregulation, and amplified sensory signaling. This distinction is vital for effective treatment, as mechanical maneuvers will not resolve neurophysiological dizziness, and vice versa.
How to Manage Stress-Related Vertigo
Managing stress-related dizziness requires a dual-track approach: downregulating the overactive stress response while actively rehabilitating the vestibular system and addressing any underlying ear pathology. A multidisciplinary strategy consistently yields the best outcomes.
1. Stress Management Techniques
Reducing your overall physiological and psychological stress load can significantly decrease the frequency, intensity, and duration of dizzy spells. The goal is to shift the autonomic nervous system from sympathetic dominance back toward parasympathetic balance.
- Diaphragmatic Breathing: Slow, deep belly breathing activates the vagus nerve, lowering heart rate and blood pressure while preventing hyperventilation-induced dizziness. The 4-7-8 technique (inhale for 4 seconds, hold for 7, exhale for 8) is highly effective. Aim for 5-10 cycles, twice daily or at the first sign of symptom onset.
- Progressive Muscle Relaxation (PMR): Systematically tensing and releasing muscle groups reduces chronic cervicogenic tension and decreases overall sympathetic tone. Focus particularly on the neck, jaw, and shoulder girdle, which heavily influence proprioceptive balance input.
- Mindfulness and Meditation: Daily mindfulness practice reduces amygdala hyperactivity and improves vestibular sensory processing. Apps like Headspace or Calm offer guided sessions specifically designed for anxiety and chronic dizziness. Regular practice has been shown to reduce PPPD severity and improve quality of life.
- Yoga and Tai Chi: These practices combine gentle movement, proprioceptive training, balance challenges, and breath regulation. They are clinically proven to improve vestibular compensation, reduce fall risk, and lower cortisol levels. Opt for gentle, grounded forms initially; avoid rapid inversions if acutely dizzy.
- Cognitive Behavioral Therapy (CBT): CBT is the gold-standard psychological intervention for chronic dizziness and anxiety. It helps you identify catastrophic thought patterns ("I'm going to faint," "I'm losing my mind"), develop coping statements, and gradually confront avoided situations. CBT-V (CBT for Vestibular disorders) specifically targets motion avoidance and fear conditioning.
2. Vestibular Rehabilitation and Home Exercises
If you have an underlying vestibular issue or chronic dizziness, a physical therapist can guide you through vestibular rehabilitation therapy (VRT). VRT is a customized exercise program designed to promote central nervous system compensation and sensory substitution. It typically involves three core components: habituation (repeated exposure to provocative movements to desensitize the system), adaptation (gaze stability exercises like VOR x1 and VOR x2 to retrain eye-head coordination), and balance training.
For BPPV-related vertigo, specific head movements called canalith repositioning maneuvers can provide rapid mechanical resolution. The Epley maneuver is most commonly used for posterior canal BPPV. A safer, more accessible home version for many patients is the Half-Somersault or Foster Maneuver, which achieves similar results with less neck strain.
Note: Always have your vertigo type diagnosed by a professional before attempting canalith repositioning at home, as performing the wrong maneuver can move crystals into a different canal and worsen symptoms. If your vertigo is stress-mediated or central, VRT focuses less on canal repositioning and more on gaze stability, dynamic balance, and gradual exposure to visual-motion triggers.
3. Lifestyle and Self-Care Adjustments
Sustainable daily habits build neurological resilience against both stress and vestibular dysfunction. The brain requires stable metabolic conditions to compensate for balance disturbances effectively.
- Optimize Hydration and Electrolytes: Chronic mild dehydration reduces cerebral perfusion and blood volume, exacerbating lightheadedness. Aim for 2-3 liters of water daily, and ensure adequate sodium, potassium, and magnesium intake, especially if you exercise or consume diuretics like caffeine.
- Eat Regular, Balanced Meals: Hypoglycemia causes brain energy deficits, triggering dizziness, shakiness, and anxiety. Prioritize protein-rich breakfasts, complex carbohydrates, and healthy fats to stabilize blood sugar. For Meniere's patients, a consistent low-sodium diet (<1500-2000 mg/day) is critical for fluid regulation.
- Get Consistent, Quality Sleep: The brain consolidates vestibular compensation and clears metabolic waste during deep sleep. Aim for 7-9 hours per night. Maintain a strict sleep schedule, limit blue light before bed, and create a cool, dark environment. Poor sleep dramatically lowers the threshold for vertigo and anxiety.
- Identify and Limit Aggravating Substances: Caffeine, alcohol, and nicotine are potent vestibular and autonomic disruptors. Caffeine can trigger migraines and increase anxiety; alcohol is directly ototoxic and alters endolymph density; nicotine causes microvascular constriction. Tapering these often yields noticeable symptom improvement.
- Maintain a Symptom Journal: Track your dizziness alongside stress levels, sleep quality, diet, menstrual cycles, and environmental triggers. Over 2-4 weeks, patterns will emerge that allow you to proactively adjust your routine rather than reactively treat flare-ups.
For more coping strategies, the Mayo Clinic offers helpful resources on vertigo and stress triggers on managing stress and anxiety with vestibular disorders. Integrating these evidence-based lifestyle modifications with medical care creates a robust foundation for long-term vestibular health.
When to See a Doctor
While some dizziness can be managed with home exercises and stress reduction, professional evaluation is essential to rule out serious underlying conditions and confirm an accurate diagnosis. Vertigo can occasionally signal life-threatening neurological or cardiovascular events. Self-management should never replace medical assessment when red flags are present or symptoms persist beyond a few days.
Seek medical attention if you experience:
- Severe or persistent vertigo that lasts continuously for hours to days without improvement, or significantly impairs walking, eating, or self-care.
- Vertigo accompanied by hearing loss, sudden tinnitus, or pressure in one ear. This strongly suggests peripheral pathology like Meniere's disease, sudden sensorineural hearing loss, or labyrinthitis, which may require prompt steroid treatment to preserve hearing.
- Dizziness with other neurological symptoms, such as double vision, facial droop, limb weakness or numbness, severe uncharacteristic headache, slurred speech, or profound coordination loss. Seek emergency care if these symptoms appear suddenly, as they may indicate stroke or TIA.
- Fainting, chest pain, irregular heartbeat, or shortness of breath alongside dizziness, which may point to cardiac arrhythmias, structural heart disease, or severe autonomic dysfunction.
- Vertigo that begins after a significant head injury, which requires imaging to rule out concussion, cervical spine damage, or perilymphatic fistula.
During your evaluation, a healthcare provider (typically a primary care physician, ENT, or neurologist) will perform a comprehensive physical and neurological exam. Diagnostic workup may include the Dix-Hallpike test or roll test for BPPV, audiometry to assess hearing, videonystagmography (VNG) or rotary chair testing to evaluate vestibular function, and blood work to check for anemia, thyroid dysfunction, or metabolic imbalances. If central pathology is suspected, an MRI of the brain may be ordered. Treatment is highly specific to the diagnosis, ranging from canalith repositioning and vestibular physical therapy to preventive migraine medications, diuretics for Meniere's, or targeted anxiety treatments. Early intervention dramatically improves prognosis and prevents chronic disability.
Frequently Asked Questions
Can stress alone cause true rotational vertigo?
Stress rarely causes true rotational vertigo in a completely healthy vestibular system. Instead, stress typically induces lightheadedness, a floating sensation, or unsteadiness through hyperventilation, blood pressure changes, and autonomic arousal. However, stress can absolutely trigger true spinning vertigo in individuals with an underlying vulnerability, such as a predisposition to vestibular migraines, undiagnosed mild Meniere's disease, or prior vestibular injury. Additionally, chronic stress can contribute to the development of PPPD, which creates persistent, real dizziness driven by maladaptive brain processing rather than peripheral ear damage.
How long does stress-induced vertigo typically last?
The duration varies significantly based on the underlying mechanism. Anxiety or panic-induced dizziness usually peaks within 10-20 minutes and resolves as the nervous system downregulates. If stress triggers a vestibular migraine, symptoms may last from several hours to several days. In cases where chronic stress contributes to PPPD or delays compensation after an ear infection, the sensation of dizziness can become persistent and fluctuate over weeks or months until targeted rehabilitation and stress management are implemented.
Does anxiety medication help with stress-related vertigo?
In many cases, yes. Medications like SSRIs (e.g., sertraline, escitalopram) or SNRIs (e.g., venlafaxine) are frequently prescribed for chronic vestibular dizziness and PPPD. They work by modulating serotonin and norepinephrine in the brainstem and vestibular nuclei, reducing neural hyperexcitability, improving sensory filtering, and breaking the fear-avoidance cycle. Benzodiazepines may be used short-term for severe acute attacks but are generally avoided for long-term use as they can actually delay central vestibular compensation and increase dependency risk. Always consult a physician to determine if medication is appropriate for your specific presentation.
How can I tell if my dizziness is from an inner ear infection or just stress?
Inner ear infections (vestibular neuritis/labyrinthitis) typically cause sudden, severe, continuous vertigo that lasts for days, is unrelenting regardless of position, and is accompanied by significant nausea, vomiting, and nystagmus. Stress-related dizziness, by contrast, tends to fluctuate with emotional state, worsens in busy visual environments or during posture changes without true rotation, and lacks the intense, acute onset of viral labyrinthitis. Furthermore, labyrinthitis does not improve significantly with relaxation alone, whereas stress-mediated symptoms often lessen noticeably when breathing is controlled and anxiety is managed. A clinical examination and vestibular testing are the most reliable ways to differentiate the two.
Can dietary changes really help reduce stress-related vertigo?
Yes, diet plays a substantial role in vestibular stability. Blood sugar fluctuations from irregular meals or high-sugar diets can mimic or worsen dizziness. Caffeine and alcohol are known to disrupt sleep architecture, increase anxiety, and alter inner ear fluid dynamics. For individuals with vestibular migraines or Meniere's disease, specific dietary triggers like aged cheeses, processed meats, high sodium intake, and artificial sweeteners (like MSG or aspartame) can directly provoke vertigo. Adopting a consistent, anti-inflammatory, whole-food diet with adequate hydration stabilizes both the autonomic nervous system and vestibular physiology, creating a stronger foundation for stress resilience.
Conclusion
The connection between psychological stress and vertigo is both complex and clinically significant. While stress rarely generates structural damage in a healthy ear, it profoundly influences the neuroendocrine, vascular, and sensory pathways that govern human balance. By triggering autonomic arousal, altering neurotransmitter balance, and lowering the threshold for conditions like vestibular migraines, Meniere's disease, and PPPD, chronic tension can transform mild imbalance into debilitating vertigo.
Recognizing that your symptoms are real, physiologically grounded, and treatable is the first step toward recovery. Effective management requires moving beyond quick fixes and embracing a comprehensive, evidence-based approach. This includes targeted vestibular rehabilitation to retrain the brain's balance processing, deliberate stress-reduction practices to calm the nervous system, and strategic lifestyle adjustments that support neurological and metabolic stability. Working with a multidisciplinary team of healthcare providers ensures that underlying conditions are properly diagnosed while psychological factors are addressed with compassion and clinical expertise. With the right combination of medical guidance, physical therapy, and stress management, most individuals can break the anxiety-vertigo cycle, regain their equilibrium, and return to a confident, active life.
About the author
David Chen, DO, is a board-certified neurologist specializing in neuro-oncology and stroke recovery. He is the director of the Comprehensive Stroke Center at a New Jersey medical center and has published numerous articles on brain tumor treatment.