Sun Cream and Eczema: The Complete Dermatologist-Approved Guide

Stepping outside during the warmer months should feel liberating, yet for individuals navigating chronic atopic dermatitis, summer often introduces a complex layer of anxiety and careful planning. The intersection of ultraviolet radiation, elevated temperatures, perspiration, and compromised skin barriers creates a perfect storm that can rapidly destabilize even well-managed dermatological routines. Navigating sun cream and eczema requires more than simply selecting a high SPF bottle off the pharmacy shelf; it demands a scientifically grounded approach to ingredient evaluation, barrier repair protocols, and strategic environmental management. Research consistently demonstrates that while sun exposure offers undeniable benefits for mood regulation and endogenous vitamin D synthesis, unshielded UV radiation can trigger oxidative stress, degrade collagen, and provoke inflammatory cascades that directly exacerbate eczematous lesions as detailed by the National Institutes of Health. By understanding the biochemical interactions between photoprotective agents and atopic skin, patients and caregivers can construct resilient, dermatologist-backed defense systems that minimize flare triggers while maximizing outdoor safety and comfort. This comprehensive guide explores the clinical evidence behind sun protection formulations, outlines precise application methodologies tailored to sensitive skin, and provides actionable strategies for integrating photoprotection into long-term eczema management plans.
Understanding the Link Between Sun Cream and Eczema
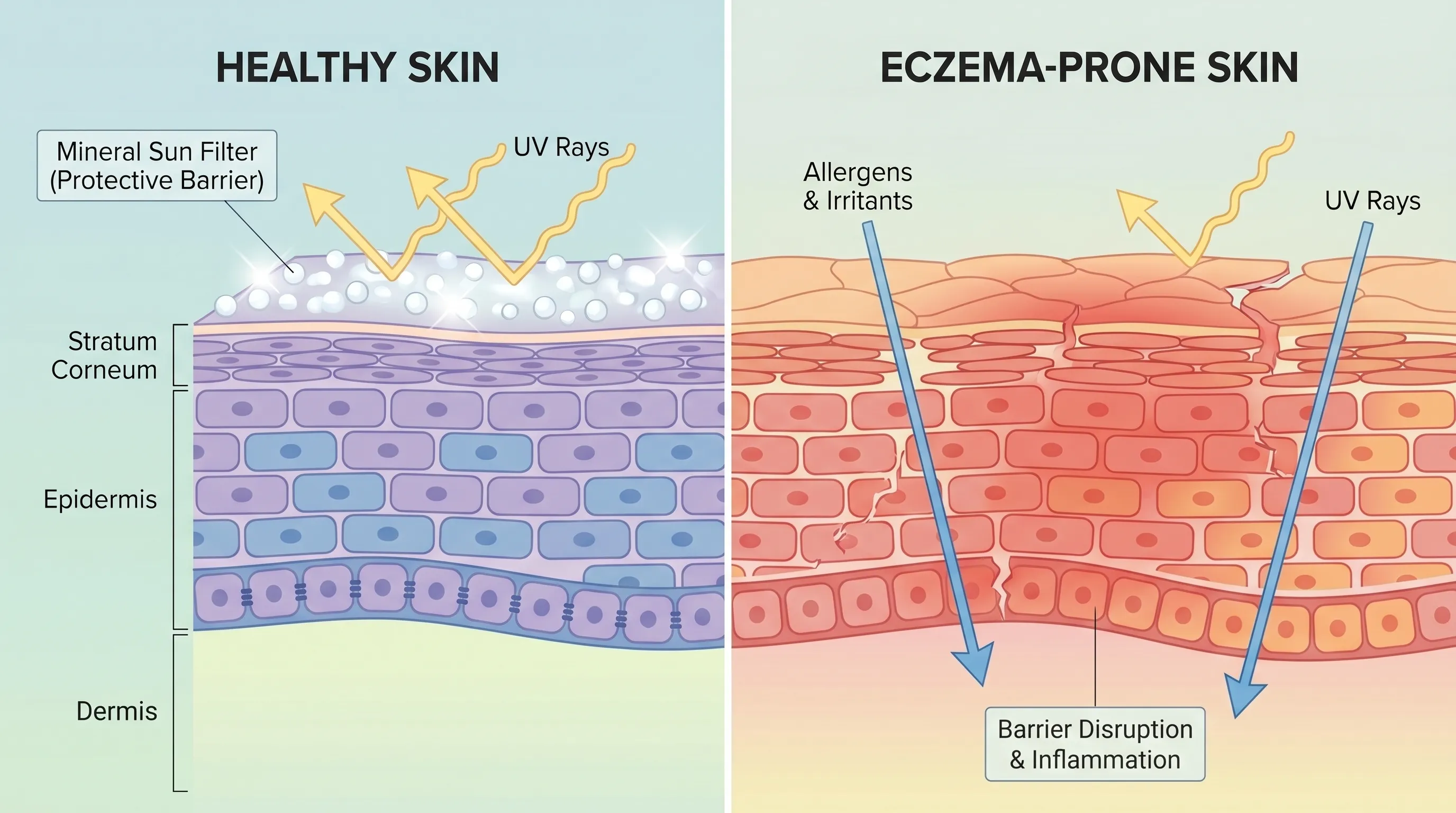
Atopic dermatitis is fundamentally a multifactorial inflammatory condition characterized by filaggrin gene mutations, impaired stratum corneum integrity, dysregulated immune responses, and altered cutaneous microbiome composition. The skin barrier in eczema-prone individuals exhibits decreased ceramide levels, elevated transepidermal water loss, and heightened susceptibility to environmental aggressors. When ultraviolet light strikes compromised epidermal tissue, it penetrates deeper layers more readily than in healthy skin, generating reactive oxygen species that amplify inflammatory pathways. This heightened reactivity explains why many patients experience severe worsening of lesions following unmediated sun exposure, despite anecdotal reports that moderate sunlight occasionally provides temporary symptom relief for certain subtypes of dermatitis.
How UV Radiation Impacts Eczema-Prone Skin
Ultraviolet radiation is categorized into UVA and UVB wavelengths, each interacting with cutaneous tissue through distinct mechanisms. UVB rays, responsible for acute erythema and direct DNA damage, penetrate the epidermis and stimulate keratinocytes to release pro-inflammatory cytokines such as interleukin-1 alpha, tumor necrosis factor-alpha, and interferon-gamma. These mediators accelerate T-cell recruitment and mast cell degranulation, directly correlating with the intense pruritus and erythema characteristic of acute eczema flares. UVA rays, conversely, penetrate the reticular dermis, inducing indirect oxidative damage through free radical generation and accelerating matrix metalloproteinase activity that degrades structural proteins. For individuals already managing chronic barrier dysfunction, this cumulative photoaging and inflammatory burden significantly impairs wound healing and increases susceptibility to secondary bacterial colonization, particularly Staphylococcus aureus.
Clinical dermatology literature consistently emphasizes that while narrowband UVB therapy under strict medical supervision demonstrates therapeutic efficacy for certain psoriatic and atopic conditions, ambient solar exposure lacks controlled dosing and often delivers unpredictable UV ratios. Mayo Clinic dermatology experts note that unregulated solar exposure frequently triggers photoaggravated eczema, a distinct clinical phenomenon where UV light acts as a direct catalyst for lesion expansion and refractory pruritus. Understanding these pathophysiological mechanisms underscores why strategic, consistent use of sun cream and eczema-compatible formulations is not merely cosmetic, but fundamentally therapeutic in preventing disease exacerbation.
The Double-Edged Sword of Sun Exposure and Skin Barrier Function
While excessive UV exposure unequivocally damages compromised skin, complete avoidance of sunlight introduces its own complications. Endogenous vitamin D synthesis occurs primarily through UVB-mediated conversion of 7-dehydrocholesterol in the epidermis. Vitamin D receptors are extensively expressed in keratinocytes and immune cells, playing crucial roles in cathelicidin antimicrobial peptide production and regulatory T-cell differentiation. Research from the National Institutes of Health indicates that suboptimal vitamin D levels correlate with increased eczema severity scores and heightened susceptibility to cutaneous infections. This creates a clinical balancing act: patients require adequate photoprotection to prevent UV-induced barrier breakdown while maintaining sufficient vitamin D status to support innate immunity and epidermal homeostasis.
Heat and perspiration further complicate this dynamic. Elevated ambient temperatures increase peripheral vasodilation and sweat gland activity. Eczematous skin contains elevated sodium chloride concentrations in sweat due to impaired ion channel function. When this hypertonic sweat evaporates across fissured epidermal surfaces, it creates localized osmotic stress that triggers intense stinging, erythema, and neurogenic pruritus via TRPV1 receptor activation. Sun protection strategies must therefore address not only UV filtration but also thermoregulation and moisture management. Integrating sun cream and eczema care requires selecting formulations that do not occlude sweat ducts excessively, avoiding heavy petrolatum bases during peak heat, and prioritizing breathable, mineral-based filters that sit on the skin surface without disrupting transepidermal water balance.
Choosing the Right Sun Protection for Sensitive Skin
The cosmetic and pharmaceutical industries offer thousands of sun protection products, yet the vast majority are formulated with general population skin in mind rather than the unique requirements of atopic dermatitis. Navigating this saturated marketplace demands critical ingredient literacy, understanding of regulatory labeling standards, and awareness of evidence-based dermatological recommendations. The National Eczema Association and the Skin Cancer Foundation both maintain rigorous evaluation criteria for products claiming compatibility with sensitive and dermatitis-prone skin. Their seal programs evaluate formulations for fragrance absence, allergen minimization, non-comedogenic properties, and clinical safety data.
Physical vs. Chemical Sunscreens: What’s Best?
Sun protection filters are categorized into physical (inorganic/mineral) and chemical (organic) classes, each utilizing fundamentally different photoprotective mechanisms. Physical filters, primarily zinc oxide and titanium dioxide, function by reflecting, scattering, and absorbing ultraviolet radiation. These compounds remain largely on the skin surface, creating a tangible photoprotective barrier without penetrating viable epidermal layers. This localized action profile makes physical sunscreens inherently less likely to provoke allergic contact dermatitis, making them the gold standard recommendation for sun cream and eczema management by board-certified dermatologists worldwide.
Chemical sunscreens operate through photochemical absorption, converting UV energy into negligible amounts of heat that subsequently dissipate from the skin. Common active ingredients include avobenzone, octinoxate, homosalate, octisalate, octocrylene, and oxybenzone. While modern chemical filters offer elegant cosmetic elegance, lightweight textures, and water-resistant formulations, their mechanism requires molecular absorption into the stratum corneum. For compromised skin barriers, this increased penetration potential raises the likelihood of stinging, burning sensations, and delayed-type hypersensitivity reactions. Additionally, certain chemical filters like oxybenzone demonstrate estrogenic activity in vitro and have been implicated in environmental coral reef damage, prompting many health and environmental agencies to recommend mineral alternatives for daily use.
Key Ingredients to Embrace and Avoid
When evaluating sun protection products, the active UV filters represent only a fraction of the formulation. Inactive ingredients frequently serve as the primary culprits in contact dermatitis reactions among eczema patients. Dermatologists recommend prioritizing formulations that contain barrier-supportive adjuncts alongside photoprotective agents. Ceramides, particularly ceramide NP, AP, and EOP, directly replenish depleted lipid matrices in atopic skin. Colloidal oatmeal provides beta-glucan and avenanthramides that demonstrate documented anti-inflammatory and antipruritic properties. Niacinamide enhances stratum corneum cohesion, increases epidermal lipid synthesis, and modulates inflammatory cytokine production. Glycerin and hyaluronic acid attract and retain moisture without occluding pores or triggering folliculitis.
Conversely, several ingredient categories should be systematically avoided when managing sun cream and eczema interactions. Fragrance, whether labeled as parfum, essential oils, or botanical extracts, remains the number one cause of allergic contact dermatitis in dermatological literature. Alcohol denatured, commonly used as a quick-drying solvent, severely degrades the lipid barrier and induces immediate transepidermal water loss. Preservatives such as methylisothiazolinone, formaldehyde releasers, and parabens demonstrate high sensitization potential. Botanical additives like citrus extracts, tea tree oil, and lavender, while marketed as natural healing agents, contain highly volatile terpenes that rapidly oxidize upon UV exposure, generating potent contact allergens. Always prioritize products with abbreviated, recognizable ingredient lists and verified dermatological testing.
Decoding Labels: SPF, Broad-Spectrum, and Fragrance-Free Claims
Regulatory terminology surrounding sun protection often generates consumer confusion. SPF (Sun Protection Factor) exclusively measures protection against UVB radiation and does not indicate UVA coverage. An SPF 30 product blocks approximately 97% of UVB rays, while SPF 50 blocks roughly 98%. The marginal difference beyond SPF 30 rarely justifies increased exposure to potentially irritating higher concentrations of UV filters. Broad-spectrum designation, regulated by the FDA and international standards, confirms that the product has passed critical wavelength testing demonstrating proportional UVA protection relative to SPF. Without broad-spectrum certification, products leave skin vulnerable to deeper dermal damage, photoaging, and photoaggravated inflammatory conditions.
Fragrance-free labeling carries specific regulatory weight, indicating the complete absence of masking fragrances and aromatic compounds. Hypoallergenic and dermatologist-tested terms, however, lack standardized clinical definitions and do not guarantee safety for atopic dermatitis patients. Always verify that products display independent seal certifications and review independent clinical trial data when available. The table below provides a comparative framework for selecting appropriate formulations.
| Feature | Physical/Mineral Sun Creams | Chemical/Organic Sun Creams |
|---|---|---|
| Active Mechanism | Reflects and scatters UV radiation | Absorbs UV radiation and converts to heat |
| Common Active Ingredients | Zinc oxide, titanium dioxide | Avobenzone, octinoxate, homosalate, oxybenzone |
| Skin Penetration Depth | Remains primarily on stratum corneum | Absorbs into viable epidermis |
| Irritation Potential | Low to moderate (if free of additives) | Moderate to high in compromised barriers |
| Cosmetic Texture | Can leave white cast, thicker consistency | Lightweight, transparent, easily absorbed |
| Water Resistance | Generally good with proper formulation | Excellent in modern polymer-stabilized systems |
| Ideal Use Case | Daily sensitive skin, post-procedure, active eczema | Athletic activities, water sports, non-reactive skin |
| Recommendation for Atopic Dermatitis | Strongly preferred by dermatologists | Use cautiously, patch test extensively first |
Step-by-Step Application Guide for Eczema Management
Proper application technique fundamentally determines whether sun protection acts as a therapeutic shield or an unintended irritant. Many patients inadvertently compromise their skin barriers through aggressive rubbing, improper layering sequences, or inadequate product amounts. Clinical studies demonstrate that the average consumer applies only 50 to 75 percent of the recommended sun protection dosage, drastically reducing stated SPF efficacy and leaving skin vulnerable to subclinical UV damage that accumulates over time. For eczema-prone individuals, precision in application methodology directly correlates with reduced flare frequency and improved barrier resilience.
Timing Your Application for Maximum Protection
Sun protection products require adequate time to bind with the epidermal surface and achieve uniform photostability. Mineral formulations typically achieve optimal distribution within 15 to 20 minutes of application. This waiting period allows volatile solvents to evaporate, particle suspensions to settle into skin crevices, and protective matrices to stabilize. Applying sun cream immediately before stepping into direct sunlight frequently results in uneven coverage, increased product migration, and higher likelihood of ocular irritation or follicular plugging.
Environmental conditions significantly influence timing effectiveness. High humidity slows evaporation rates, potentially extending the required stabilization period to 25 minutes. Wind and heat accelerate solvent evaporation, which can cause premature drying and patchy film formation. Dermatologists recommend applying sun cream in a cool, shaded environment before dressing or heading outdoors. For extended outdoor activities, plan a secondary application window 30 minutes after initial exposure to address any areas compromised by friction, sweat, or uneven settling.
Layering Sun Cream Over Moisturizers and Medications
The sequential application of dermatological products requires careful orchestration to prevent product antagonism, reduced therapeutic penetration, and barrier disruption. The established clinical protocol prioritizes prescription medications as the foundational layer. Topical corticosteroids, calcineurin inhibitors like pimecrolimus or tacrolimus, and Janus kinase inhibitors must contact clean, dry epidermal surfaces to achieve optimal receptor binding and anti-inflammatory efficacy. Applying occlusive products beneath prescription treatments creates a physical barrier that significantly reduces medication bioavailability and compromises treatment outcomes.
After medication absorption, apply your daily moisturizer. Ceramide-rich creams, ointments, or lotions replenish intercellular lipids, seal in hydration, and provide a smooth substrate for subsequent products. Allow 10 to 15 minutes for complete absorption before proceeding to photoprotection. When applying sun cream and eczema-safe formulations, use gentle patting and pressing motions rather than vigorous circular rubbing. This technique minimizes mechanical friction, reduces shear stress on fragile epidermal surfaces, and ensures uniform particle distribution without disturbing underlying therapeutic layers. Always apply the recommended density of 2 milligrams per square centimeter, which roughly translates to a nickel-sized amount for the face and two ounces for full-body coverage.
Reapplication Without Triggering a Flare
Consistent reapplication every two hours, or immediately following swimming, heavy perspiration, or towel drying, remains essential for sustained photoprotection. However, frequent reapplication across compromised skin barriers introduces cumulative product exposure and mechanical friction that can provoke contact irritation. Dermatologists recommend strategic reapplication protocols tailored to atopic dermatitis management. During active flares, minimize sun exposure during peak UV hours (10 AM to 4 PM) and rely primarily on physical barriers like UPF clothing, wide-brimmed hats, and portable shade structures.
When reapplication is necessary, use gentle patting techniques with clean fingertips or soft silicone applicators rather than rubbing with towels or abrasive fabrics. Powder-based mineral sunscreens containing micronized zinc oxide offer excellent reapplication alternatives for the face and neck, providing effective UV filtration without the occlusive weight or friction associated with liquid formulations. Always carry fragrance-free, individually packaged sun sticks for targeted reapplication on localized eczema patches, avoiding direct contact with open fissures or actively weeping lesions. The integration of sun cream and eczema care demands a flexible, responsive approach that adapts to daily symptom fluctuations and environmental variables.
Pediatric Considerations: Sun Cream and Eczema in Children
Pediatric atopic dermatitis affects approximately 20 percent of children worldwide, with peak onset occurring before age five. The pediatric epidermis is anatomically thinner, demonstrates reduced stratum corneum cohesion, and possesses developing enzymatic systems that metabolize topically applied compounds differently than adult skin. These physiological differences necessitate age-specific photoprotection protocols, careful product selection, and vigilant monitoring for early signs of adverse reactions. Parents and caregivers managing childhood eczema require specialized guidance to navigate the unique intersection of developmental dermatology and sun safety.
Age-Appropriate Sun Protection Strategies
The American Academy of Pediatrics and pediatric dermatology societies universally recommend complete avoidance of direct sunlight and sun cream application for infants younger than six months. CDC sun safety guidelines emphasize that the infantile epidermal barrier lacks sufficient lipid maturity to prevent systemic absorption of topical agents, and renal and hepatic metabolic pathways remain underdeveloped for processing chemical UV filters. For this age group, photoprotection relies exclusively on environmental modifications: dense shade structures, UPF 50+ clothing, wide-brimmed sun hats, and avoidance of peak solar intensity periods.
For children over six months with managed eczema, mineral-based sun protection becomes appropriate. Zinc oxide and titanium dioxide formulations demonstrate negligible systemic absorption, making them the safest active ingredients for developing skin barriers. Parents should select products specifically labeled for pediatric use, verified by independent dermatological safety programs, and formulated without parabens, phthalates, artificial fragrances, or essential oils. Application should focus exclusively on exposed areas not covered by sun-protective clothing. During school and daycare settings, establish clear communication with caregivers regarding the child's photoprotection routine, reapplication schedule, and early signs of heat rash or product-induced irritation.
Recognizing Early Signs of Contact Dermatitis from Sun Products
Distinguishing between an eczema exacerbation, heat-induced miliaria, and allergic contact dermatitis presents a common diagnostic challenge for parents and pediatricians. Contact dermatitis typically manifests within 24 to 72 hours of product application, presenting as well-demarcated erythema, pruritic vesicles, or edematous plaques localized precisely to application sites. Unlike generalized eczema flares, which often follow flexural distribution patterns, contact reactions remain confined to areas where the specific product made direct epidermal contact.
Immediate discontinuation of the suspected product constitutes the primary intervention. Gently cleanse the affected area with lukewarm water and a non-soap, pH-balanced cleanser. Apply a bland, fragrance-free barrier ointment to support recovery. If symptoms persist beyond 72 hours, involve a pediatric dermatologist to perform standardized patch testing, which identifies specific offending allergens within complex cosmetic formulations. Early recognition prevents chronic barrier disruption, reduces systemic corticosteroid requirements, and empowers caregivers to curate safer product portfolios for long-term management of sun cream and eczema compatibility in childhood.
Beyond Sun Cream: Holistic Sun Safety for Eczema
While topical photoprotection forms a critical component of atopic dermatitis management, relying exclusively on sun cream creates unnecessary vulnerability when environmental, behavioral, and nutritional factors are neglected. Comprehensive sun safety integrates physical barriers, thermoregulation strategies, microbiome support, and systemic anti-inflammatory nutrition. This multidimensional approach reduces the cumulative burden on compromised skin barriers while enhancing overall dermatological resilience during high-UV seasons.
Clothing, Shade, and Environmental Controls
UPF (Ultraviolet Protection Factor) rated textiles offer superior, consistent photoprotection without requiring reapplication or chemical exposure. UPF 50+ clothing blocks over 98 percent of UVA and UVB radiation, maintaining efficacy regardless of sweat or washing cycles. Prioritize tightly woven cotton, bamboo, or merino wool blends that balance breathability with coverage. Avoid loose-knit synthetics that allow significant UV penetration despite opaque appearance. Wide-brimmed hats with neck flaps, UV-filtering sunglasses, and lightweight long-sleeve sun shirts dramatically reduce exposed surface areas requiring topical application.
Environmental controls significantly influence symptom severity. Seek dense tree canopies, UV-blocking umbrellas, and architectural shade during outdoor activities. Utilize smart home devices and weather applications that track real-time UV index readings. When the UV index exceeds 6, prioritize indoor activities during midday hours or relocate exposure to early morning and late afternoon windows when solar angles are lower and UV intensity decreases. Install UV-filtering window films for home and vehicle use, protecting occupants from UVA penetration during commutes and indoor activities. Combining strategic shade-seeking with physical barriers minimizes reliance on topical formulations while maintaining robust photoprotection.
Hydration and Diet: Supporting Skin from the Inside
Systemic hydration directly influences epidermal turgor, transepidermal water loss, and thermoregulation efficiency. Individuals with atopic dermatitis should maintain consistent fluid intake throughout the day, prioritizing electrolyte-balanced beverages during periods of heat exposure or physical activity. Chronic dehydration thickens blood viscosity, reduces cutaneous microcirculation, and impairs nutrient delivery to regenerating epidermal cells.
Nutritional strategies complement external photoprotection by modulating systemic inflammation and oxidative stress. Cleveland Clinic specialists note that omega-3 fatty acids, particularly EPA and DHA from wild-caught salmon, sardines, and algal supplements, demonstrate proven efficacy in reducing prostaglandin-mediated inflammation and supporting lipid barrier integrity. Antioxidant-rich foods containing vitamins C, E, and selenium neutralize UV-induced free radicals before they reach compromised epidermal tissue. Fermented foods and prebiotic fiber support gut-skin axis communication, promoting regulatory T-cell differentiation and reducing atopic hypersensitivity responses. Polyphenol-rich green tea extracts and curcumin demonstrate clinical potential in reducing photoaggravated dermatitis severity when integrated into balanced dietary patterns. Always consult healthcare providers before initiating high-dose supplementation, particularly when managing concurrent immunomodulatory therapies.

Frequently Asked Questions
Is it safe to use regular sunscreen if I have atopic dermatitis?
While many individuals tolerate standard sunscreens, those with atopic dermatitis often experience contact irritation or allergic reactions due to chemical UV filters, fragrances, and alcohol. Dermatologists strongly recommend transitioning to mineral-based, fragrance-free formulations that carry a seal of acceptance from recognized dermatological organizations. Always perform a patch test before full-body application to verify individual tolerance.
Should I apply eczema medication before or after sun cream?
The established dermatological protocol prioritizes topical medications first. Apply prescription corticosteroids or calcineurin inhibitors to clean, dry skin. Wait 15 to 20 minutes for full absorption. Follow with your daily moisturizer to restore the lipid barrier. After another 10-minute absorption window, apply sun cream as the final protective layer. This layering sequence prevents product dilution and ensures optimal therapeutic penetration.
Can mineral sunscreens cause flare-ups in eczema-prone skin?
Pure mineral formulations containing only zinc oxide and titanium dioxide are generally the least reactive option for eczema-prone individuals. However, flare-ups can still occur if the product contains secondary irritants like botanical extracts, essential oils, alcohol denat, or certain preservatives. Always verify that the inactive ingredient list is simplified and specifically formulated for compromised skin barriers.
How often should children with eczema reapply sun protection?
Children should reapply mineral-based sun protection every two hours during continuous outdoor exposure, and immediately after swimming, excessive sweating, or towel drying. For toddlers and young children with active eczema patches, consider combining physical barriers like UPF clothing, wide-brimmed hats, and strategic shade breaks with gentle sun cream application only on exposed areas to minimize cumulative product exposure.
What SPF level is recommended for managing sun cream and eczema together?
Global health guidance from the World Health Organization recommends broad-spectrum SPF 30 or higher for daily use, regardless of eczema status. Higher SPF values offer marginal incremental protection beyond SPF 50 but may increase the concentration of active ingredients, potentially raising irritation risk for highly sensitive skin. Focus on broad-spectrum UVA/UVB coverage, gentle formulation, and consistent reapplication rather than chasing extremely high SPF numbers.
Conclusion
Successfully navigating sun cream and eczema management requires moving beyond trial-and-error product experimentation toward a structured, evidence-based approach. By understanding how UV radiation interacts with compromised epidermal barriers, recognizing the distinct mechanisms of physical versus chemical UV filters, and implementing precise layering and application protocols, patients can maintain robust photoprotection without triggering inflammatory exacerbations. Pediatric populations demand age-specific safeguards, vigilant monitoring for contact reactions, and strategic reliance on physical barriers alongside gentle topical formulations. Comprehensive sun safety extends far beyond a single product selection; it integrates UPF clothing, environmental controls, systemic hydration, and anti-inflammatory nutrition into a cohesive daily practice.
The intersection of photoprotection and atopic dermatitis management continues to evolve as dermatological research advances formulation science and barrier repair therapeutics. Patients who prioritize mineral-based, fragrance-free sun creams, adhere to consistent reapplication schedules, and partner closely with board-certified dermatologists experience significantly reduced flare frequencies, improved quality of life, and sustained skin resilience throughout high-UV seasons. Always verify product certifications, perform individualized patch testing, and adjust routines based on seasonal environmental changes. With informed product selection, disciplined application techniques, and holistic lifestyle integration, sun protection becomes a powerful ally in long-term eczema management rather than an unavoidable trigger.
For ongoing clinical guidance, review resources provided by the American Academy of Dermatology (https://www.aad.org/public/diseases/a-z/atopic-dermatitis) and the National Eczema Association (https://nationaleczema.org/). Consult your dermatologist before modifying prescription regimens or introducing new photoprotective products, particularly when managing pediatric eczema or concurrent immunosuppressive therapies.

About the author
Elena Vance, MD, is a double board-certified dermatologist and pediatric dermatologist. She is an assistant professor of dermatology at a leading medical university in California and is renowned for her research in autoimmune skin disorders.