Tattoo Itchy: Causes, Medical Research, and Safe Relief Strategies

When the needle pierces the epidermis and deposits pigment into the dermis, your body immediately recognizes the process as controlled trauma. This initiates a complex cascade of cellular repair, immune activation, and tissue remodeling. While the vibrant artwork itself is permanent, the physiological aftermath is temporary yet highly dynamic. One of the most universally reported sensations during this recovery window is pruritus, commonly described as a persistent tattoo itchy feeling. Understanding whether this sensation represents a routine healing milestone or a warning sign of a deeper dermatological issue requires a nuanced approach. Research consistently demonstrates that more than 70% of tattooed individuals experience some degree of tattoo-associated skin complications, with itching, erythema, and localized inflammation topping the list of immediate post-tattooing complaints (Source: Iranian Journal of Public Health). Navigating this phase safely demands a balance of proper aftercare, clinical awareness, and patience. Whether you are healing a freshly inked masterpiece or dealing with sudden irritation in an older design, knowing the biological mechanisms behind the discomfort, the potential triggers, and the medically backed interventions available will empower you to protect both your skin’s integrity and the longevity of your body art.
Understanding the Biological Basis of Tattoo Healing and Pruritus
The Physiology of Epidermal and Dermal Repair
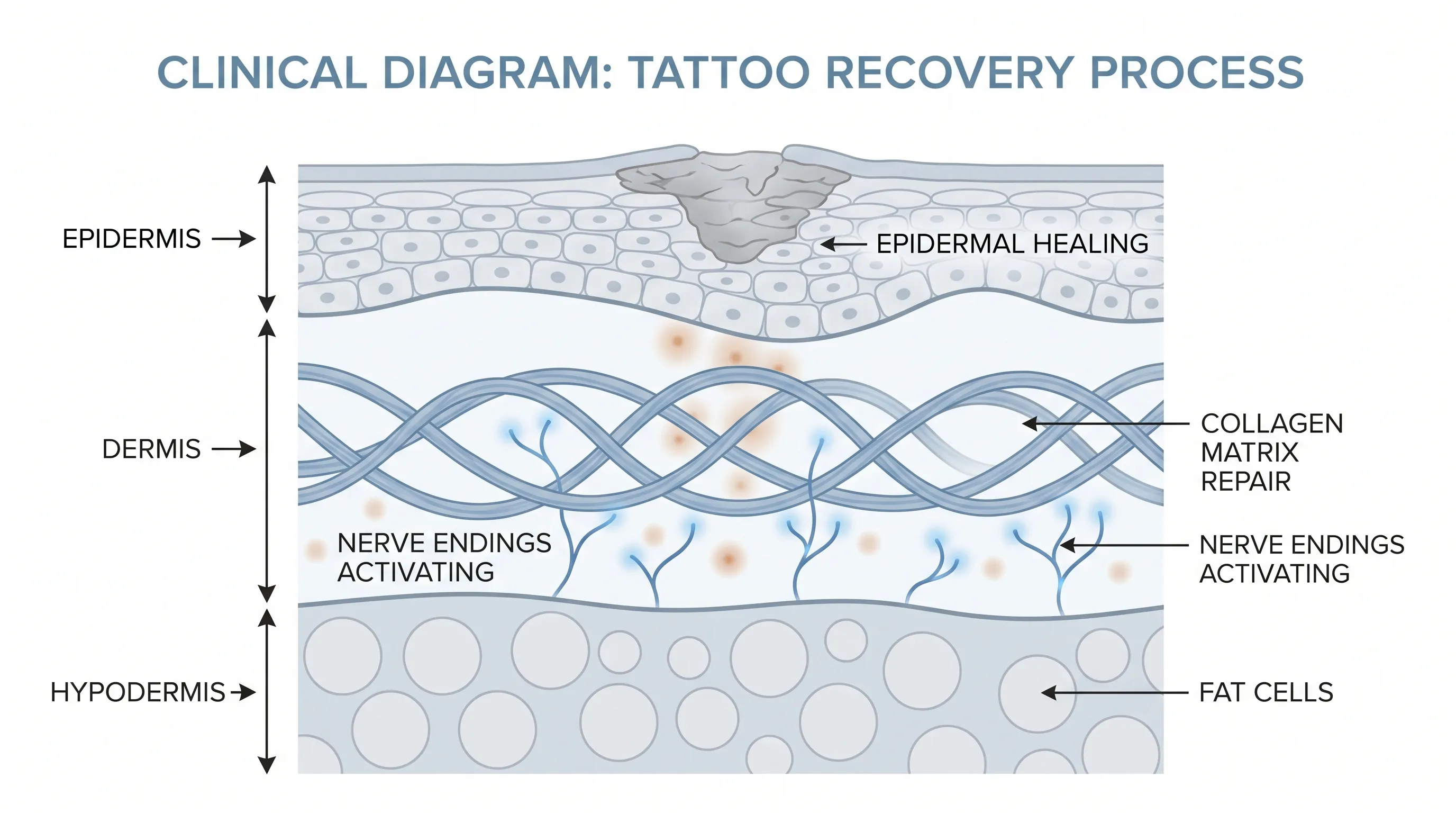
Tattooing fundamentally disrupts the skin’s structural architecture. As sterile needles repeatedly puncture the skin at a rapid frequency, they bypass the protective barrier of the stratum corneum, traverse the epidermis, and deposit pigment particles directly into the upper dermis. This microtrauma triggers an acute inflammatory response. Blood vessels dilate to increase blood flow to the area, delivering oxygen, white blood cells, and plasma proteins essential for tissue repair. As the skin begins to knit back together, fibroblasts produce collagen, and keratinocytes migrate to close the microscopic wounds. During this proliferative phase, the release of histamine and other inflammatory cytokines directly stimulates cutaneous nerve endings, resulting in the characteristic tattoo itchy sensation. This neurochemical signaling is a standard component of wound healing, indicating that the nervous system and immune cells are actively communicating to rebuild the compromised barrier. The sensation typically peaks between days three and seven, coinciding with the formation of thin scabs and the onset of epidermal shedding.
Nerve Regeneration and Cutaneous Sensitivity
The skin is densely populated with sensory receptors, including mechanoreceptors, thermoreceptors, and pruriceptors, which specifically detect itch. The physical trauma of tattooing can temporarily damage superficial nerve fibers, leading to aberrant signaling as they regenerate. This neurogenic itch is often mistaken for surface dryness, when in reality, it originates from the nerve’s attempt to restore baseline function. Additionally, the stratum corneum temporarily loses its ability to retain moisture efficiently during the healing window. Trans-epidermal water loss increases, causing the newly forming skin to become tight, flaky, and hypersensitive. When the skin contracts during scab formation and peeling, the mechanical tension further aggravates the pruriceptors. Recognizing that a tattoo itchy episode is frequently a sign of active cellular turnover, rather than a pathological condition, helps individuals avoid the common but dangerous temptation to scratch, which can disrupt the delicate matrix of healing collagen and pigment placement.
Key Medical Causes of a Tattoo Itchy Sensation
Allergic Contact Dermatitis to Tattoo Pigments
While the skin’s natural healing process accounts for most early-stage discomfort, allergic reactions represent the second most prevalent cause of persistent irritation. The American Academy of Dermatology identifies red ink as the most frequent culprit in allergic tattoo reactions, though all colors carry potential risks (Source: AAD). These reactions are typically classified as delayed-type hypersensitivity (Type IV), mediated by T-lymphocytes that recognize specific chemical components within the pigment as foreign antigens. Red pigments historically contained mercury sulfide (cinnabar), though modern formulations rely heavily on organic compounds, aluminum derivatives, iron oxides, and various azo dyes. Even with regulatory improvements, these compounds can degrade into sensitizing chemicals over time. Symptoms of an allergic reaction include intense, localized itching, raised papules, scaling, and occasionally weeping vesicles confined strictly to the inked lines. Importantly, allergic responses can manifest immediately or remain dormant for months to years before presenting. Some individuals only experience sensitization following systemic shifts, such as initiating antiretroviral therapy for HIV or undergoing orthopedic surgeries, which alter baseline immune tolerance and trigger previously dormant reactions to embedded pigments.
Bacterial Infections and Contamination Pathways
When the protective epidermal barrier is compromised, the underlying dermis becomes highly susceptible to microbial colonization. Non-sterile equipment, improperly diluted inks, unhygienic studio environments, or inadequate home aftercare can introduce opportunistic pathogens like Staphylococcus aureus, Streptococcus pyogenes, or Mycobacterium species into the wound bed. Unlike normal healing itch, infection-related pruritus is almost always accompanied by escalating erythema, warmth, purulent discharge, and throbbing pain that extends beyond the tattoo borders. As the bacterial load increases, the immune system releases higher concentrations of prostaglandins and leukotrienes, which intensify nerve stimulation. In severe cases, cellulitis or systemic toxicity may develop, marked by fever, chills, and lymphadenopathy. Differentiating infection-driven itching from routine healing is critical, as bacterial proliferation can permanently distort tattoo artwork through tissue necrosis and scarring. Prompt clinical intervention with targeted antibiotic therapy is non-negotiable when infectious signs appear.
Pre-Existing Dermatological Conditions and Koebner Phenomenon
Individuals with chronic inflammatory skin disorders face elevated risks when undergoing body modification. Conditions such as eczema, psoriasis, seborrheic dermatitis, and lichen planus can exhibit the Koebner phenomenon, wherein new skin lesions form along lines of trauma, including tattoo needle tracks. The mechanical injury and subsequent inflammatory cascade can reactivate dormant autoimmune pathways, leading to localized flares that mimic standard tattoo healing but persist indefinitely if unmanaged. Lichenoid tattoo reactions present as intensely itchy, flat-topped, violaceous papules that histologically resemble classic lichen planus. Granulomatous reactions, while less common, involve the formation of organized immune cell clusters around pigment particles, resulting in firm, raised nodules and chronic pruritus. These conditions require dermatological management rather than standard aftercare, as topical steroids or immunomodulators may be necessary to suppress the aberrant immune response without compromising tattoo integrity.
Photoallergic and Phototoxic Reactions
Certain tattoo pigments exhibit photosensitivity, meaning they undergo chemical changes when exposed to ultraviolet radiation. Compounds such as cadmium yellow, certain red azo dyes, and titanium dioxide can absorb UV light and transition into reactive states that generate free radicals. This photoactivation triggers localized inflammatory responses in the skin, resulting in a tattoo itchy sensation accompanied by acute swelling, erythema, and occasionally blistering. The reaction typically occurs within hours of significant sun exposure and remains confined to areas where the specific pigment resides. Chronic photoallergic sensitivity can lead to persistent low-grade inflammation and accelerated pigment fading. Mitigation strategies involve strict photoprotection, including broad-spectrum sunscreen application and covering fresh or sensitive tattoos with UPF-rated clothing during prolonged outdoor activities.
Toxicological Insights and Immune System Implications
Heavy Metals, Nanoparticles, and Chemical Contaminants
Recent analytical studies have shed critical light on the chemical composition of commercial tattoo inks, revealing concerning concentrations of potentially toxic substances. Research published in the Iranian Journal of Public Health demonstrated that many widely used inks contain heavy metals—including chromium, nickel, cobalt, and arsenic—at levels significantly exceeding international safety thresholds. Chromium concentrations ranged dramatically across tested batches, frequently surpassing the recommended limit of 5 parts per million. Similarly, nickel, a potent allergen, was detected at clinically relevant thresholds that explain the high prevalence of delayed hypersensitivity reactions. Beyond metals, polycyclic aromatic hydrocarbons (PAHs) represent a major toxicological concern. Benzo(a)pyrene, a potent PAH and recognized human carcinogen, was identified in black tattoo inks at concentrations up to 200 times higher than the Council of Europe’s recommended safety limit (Source: NIH PMC). These lipophilic compounds can penetrate cellular membranes, bind to DNA, and potentially initiate mutagenic processes over prolonged exposure periods.
Carbon black nanoparticles, the primary pigment in standard black ink, are classified as a Group 2B potential carcinogen due to their ability to induce oxidative stress and cellular inflammation. Meanwhile, titanium dioxide, commonly used to lighten colors or create white highlights, has demonstrated genotoxic potential in vivo, raising questions about long-term dermal safety. The presence of these compounds underscores the importance of regulatory oversight and the necessity for consumers to inquire about pigment sourcing and manufacturer transparency before undergoing procedures. For a comprehensive overview of ink risks, consult peer-reviewed literature like this ScienceDirect publication.
Macrophage Uptake and Long-Term Immune Dynamics
Once pigment particles are deposited in the dermis, they are not merely inert decorations suspended in tissue. The immune system actively responds to their presence. Dermal macrophages and dendritic cells phagocytize foreign particles in an attempt to clear them, but due to their size and chemical stability, the pigments resist lysosomal degradation. Consequently, the immune cells retain the pigment indefinitely, effectively acting as biological reservoirs that stabilize the tattoo. When macrophages eventually undergo apoptosis, they release their captured pigment, only for newly recruited macrophages to re-ingest it. This cyclical process maintains the tattoo’s visibility but establishes a state of chronic, low-grade immune activation. Emerging research suggests that this persistent antigenic load can subtly modulate local immune function, potentially influencing how the skin responds to subsequent stimuli. The Epidemiological Tattoo Assessment Tool provides frameworks for tracking these long-term dermatological interactions.

Evidence-Based Relief Strategies and Clinical Management
Safe Aftercare Protocols for Fresh Ink
Managing a tattoo itchy episode during the initial healing window requires a disciplined, hygiene-focused approach. The foundational principle is to support the skin’s natural barrier restoration while minimizing external irritants. Gently cleanse the area twice daily using lukewarm water and a mild, fragrance-free antibacterial soap. Avoid scrubbing, which disrupts the fragile epidermal matrix. After patting the skin completely dry with a clean paper towel, apply a thin layer of artist-recommended ointment or a petroleum-based barrier for the first three to five days. This occlusive layer prevents excessive moisture loss and reduces friction against clothing. Once the initial weeping phase subsides and thin scabs begin to form, transition to a fragrance-free, hypoallergenic moisturizer. Products containing ceramides, panthenol, or squalane effectively replenish lipid barriers without suffocating the healing tissue. Applying moisturizer multiple times daily prevents the tightness that exacerbates itching. Cool compresses applied intermittently provide immediate neurosensory relief by constricting superficial blood vessels and temporarily numbing hyperactive nerve endings. Crucially, individuals must resist scratching. If the urge becomes overwhelming, gently tap or slap the surrounding skin, which provides counter-stimulation without damaging the healing matrix. Additional visual guidance is available in this educational YouTube resource.
Managing Chronic Itch in Healed and Older Tattoos
When a tattoo itchy sensation emerges months or years after completion, the etiology shifts away from acute wound healing toward allergic, dermatological, or environmental triggers. For mild, intermittent irritation, maintaining optimal skin hydration remains paramount. Use thick, occlusive creams during colder months when ambient humidity drops, and incorporate gentle chemical exfoliants like lactic acid to remove dead keratinocytes that trap heat and irritate pruriceptors. Over-the-counter oral antihistamines, particularly non-sedating second-generation formulations like cetirizine or loratadine, can systemically reduce histamine-mediated itch without the risks associated with topical application on compromised barriers. Avoid applying topical hydrocortisone or antibiotic ointments to old tattoos without medical supervision, as prolonged steroid use can cause cutaneous atrophy, while antibiotics may disrupt the local microbiome and promote resistant strains. For individuals experiencing severe, refractory pruritus, recent clinical literature highlights a breakthrough therapeutic avenue. A 2024 NIH case series documented the successful resolution of chronic tattoo-related pruritus using topical Janus kinase (JAK) inhibitors, specifically ruxolitinib (Source: NIH PMC). By interrupting intracellular inflammatory signaling pathways, JAK inhibitors target the root cytokine activity driving the itch response, offering a promising, targeted intervention for patients unresponsive to conventional therapies.
Recognizing Clinical Warning Signs and When to Escalate Care
Differentiating Normal Pruritus from Pathological Complications
Knowing when a tattoo itchy sensation crosses the threshold from physiological recovery to pathological complication is essential for preventing permanent damage. Normal healing itch typically remains localized, fluctuates in intensity, gradually diminishes over ten to fourteen days, and responds well to moisturization and cool therapy. It is rarely accompanied by systemic symptoms. Conversely, infection, severe allergy, or immune-mediated dermatitis present distinct clinical patterns. Spreading erythema that extends beyond the tattooed lines, particularly when warm to the touch, strongly suggests cellulitis. Red streaks radiating from the site indicate lymphangitis, a medical emergency requiring immediate antibiotic administration. Persistent, worsening pain that disrupts sleep, foul-smelling purulent drainage, or the development of pustules and yellow crusts signal bacterial proliferation that standard home care cannot resolve.
Allergic and Autoimmune Reaction Indicators
Allergic contact dermatitis often presents with well-demarcated, raised, scaly plaques that strictly follow the lines of specific pigments. If the entire tattoo becomes uniformly inflamed and intensely itchy, accompanied by widespread swelling or hives, a systemic hypersensitivity reaction may be underway. Individuals with pre-existing autoimmune skin conditions should monitor closely for Koebnerization, where psoriatic or eczematous lesions develop exclusively over traumatized skin. Chronic granulomatous reactions manifest as firm, indurated nodules that may persist for years and require biopsy for definitive diagnosis. Photoallergic reactions are temporally linked to sun exposure and resolve with strict photoprotection, but recurrent episodes necessitate pigment-specific testing and possible laser removal consultation.
Establishing Clear Dermatological Thresholds
Seeking professional medical evaluation is warranted under several clear circumstances. If the tattoo itchy episode persists beyond two weeks without clinical improvement, or if symptoms worsen despite appropriate moisturization and hygiene, schedule a dermatology appointment. Immediate urgent care is required for signs of systemic infection: fever exceeding 100.4°F, chills, nausea, dizziness, or rapidly expanding redness. Severe allergic reactions presenting with facial swelling, respiratory difficulty, or diffuse urticaria constitute anaphylaxis and demand emergency intervention. Additionally, individuals who develop sudden, intense itching, elevation, or inflammation in previously stable, older tattoos should undergo evaluation for late-onset hypersensitivity or systemic triggers. Dermatologists may employ patch testing, skin biopsies, or prescribe targeted immunomodulators to manage complex cases effectively.
Preventative Measures and Long-Term Tattoo Health Optimization
Pre-Procedure Preparation and Artist Selection
Prevention begins long before the first needle punctures the skin. Selecting a licensed, reputable tattoo studio operating under strict health department regulations is the foundational step. Verify that artists use single-use, pre-sterilized needle cartridges and maintain barrier techniques. Reputable professionals will gladly discuss their ink suppliers, safety data sheets, and studio sanitation protocols. Prospective clients should undergo thorough skin preparation, including adequate hydration, balanced nutrition, and avoidance of blood-thinning substances like alcohol or high-dose NSAIDs for at least forty-eight hours prior to the appointment. Individuals with active skin infections, recent sunburns, or unmanaged eczema/psoriasis in the target area should postpone procedures until optimal skin barrier function is restored. Discussing pigment composition with the artist can also help mitigate risks, particularly for those with known nickel or heavy metal sensitivities.
Long-Term Maintenance and Environmental Protection
Once fully healed, tattoo longevity and skin health depend on consistent protective habits. Daily application of broad-spectrum sunscreen (SPF 30 or higher) prevents UV-induced degradation of pigment and reduces photoallergic risks. Moisturizing remains a lifelong necessity, as tattoos age within the same skin that experiences natural collagen decline and lipid loss over decades. Wearing loose, breathable clothing over large tattooed areas minimizes friction and heat buildup, which can exacerbate sensitivity. Individuals prone to dry skin should avoid hot, prolonged showers and harsh alkaline cleansers that strip essential lipids. Regular self-examination of tattooed skin helps identify early changes in texture, color, or sensation. Prompt attention to minor irritations prevents escalation into chronic dermatological issues. Integrating these practices into a comprehensive skincare routine ensures that body art remains vibrant while preserving the underlying tissue’s physiological balance.
| Complication Type | Primary Symptoms | Typical Onset | Recommended Management |
|---|---|---|---|
| Normal Healing | Mild to moderate itch, light peeling, slight redness | Days 3–14 | Moisturize, cool compress, avoid scratching |
| Allergic Dermatitis | Intense localized itch, raised papules, scaling confined to pigment | Weeks to years post-tattoo | Antihistamines, topical steroids (Rx), JAK inhibitors |
| Bacterial Infection | Spreading redness, warmth, pus, escalating pain, fever | Days 1–7 | Clinical evaluation, targeted antibiotics |
| Photoallergic Reaction | Itching, swelling, blistering after sun exposure | Immediate to 48 hrs post-UV | Strict sun protection, cool compress, topical antipruritics |
| Koebner Phenomenon | Psoriatic/eczematous plaques over tattoo lines | Weeks to months | Dermatologist care, immunomodulators, trigger avoidance |
Frequently Asked Questions
Is it normal for a tattoo to be itchy during the first week?
Yes, a tattoo itchy sensation is a completely normal physiological response during the initial seven to fourteen days of healing. As the epidermis regenerates and superficial nerve endings repair, histamine release and tissue contraction naturally trigger pruritus. This indicates active cellular turnover rather than a complication, provided there are no signs of infection such as spreading redness, pus, or severe pain.
Why does an old tattoo suddenly feel itchy and raised?
Sudden pruritus and elevation in a fully healed tattoo often signal a delayed allergic reaction, environmental trigger, or immune system shift. Changes in weather, seasonal allergies, hormonal fluctuations, or initiation of new medications can lower the immune threshold, causing the body to suddenly react to previously tolerated pigment particles. Photoallergic responses from sun exposure and localized dermatological flares also contribute to late-onset irritation.
What is the safest way to relieve a tattoo itchy feeling without damaging the ink?
The most effective and safe approach involves maintaining consistent hydration with fragrance-free, hypoallergenic moisturizers and applying intermittent cool compresses. If the urge to scratch becomes overwhelming, gently tapping or pressing a clean cloth against the area provides counter-stimulation. Avoid hot water, harsh soaps, and over-the-counter topical anesthetics unless explicitly approved by a dermatologist, as these can compromise the healing barrier or alter pigment retention.
Can allergic reactions to tattoo ink develop years after getting inked?
Absolutely. Allergic contact dermatitis is a delayed-type hypersensitivity reaction that can remain clinically silent for months or years before manifesting. Systemic immune alterations, such as starting new prescription medications, experiencing significant hormonal changes, or developing unrelated autoimmune conditions, can trigger a previously dormant sensitivity to specific metal salts or organic compounds embedded in the dermis. Red and yellow pigments are historically the most common culprits.
Are there medical treatments available for severe, chronic tattoo itch?
Yes, recent dermatological advances have expanded the therapeutic arsenal for refractory tattoo pruritus. While traditional management relies on oral antihistamines and topical corticosteroids, emerging research highlights the efficacy of topical Janus kinase (JAK) inhibitors like ruxolitinib. These targeted immunomodulators disrupt the specific cytokine pathways driving chronic itch, offering significant relief for patients who have not responded to conventional therapies. A board-certified dermatologist can evaluate suitability and prescribe appropriate regimens.
Conclusion
Navigating the complex interplay between body art and cutaneous physiology requires vigilance, education, and adherence to evidence-based care. While a tattoo itchy sensation is overwhelmingly a routine component of the epidermal repair process, distinguishing physiological pruritus from allergic, infectious, or autoimmune complications is essential for preserving both skin health and artistic integrity. The evolving toxicological landscape surrounding commercial pigments underscores the importance of selecting regulated products and understanding potential long-term immune interactions. By implementing disciplined aftercare protocols, maintaining optimal skin barrier function, and seeking timely clinical evaluation when red flags emerge, individuals can safely navigate the healing journey and enjoy their tattoos for a lifetime. Advances in targeted dermatological therapies, including JAK inhibitors, continue to refine the management of chronic tattoo-related complications, reflecting a growing commitment to patient-centered, science-driven skin care. Whether you are healing your first piece or managing irritation in older ink, prioritizing medical accuracy over anecdotal advice ensures optimal outcomes and lasting confidence in your body art journey.

About the author
Elena Vance, MD, is a double board-certified dermatologist and pediatric dermatologist. She is an assistant professor of dermatology at a leading medical university in California and is renowned for her research in autoimmune skin disorders.