Multilevel Disc Desiccation: Causes, Symptoms & Evidence-Based Management

Receiving an MRI report that mentions "multilevel disc desiccation" can immediately trigger anxiety, especially if the medical terminology sounds unfamiliar or intimidating. However, understanding this finding requires separating radiological descriptors from clinical diagnoses, recognizing that the human spine undergoes predictable, often asymptomatic, structural changes as part of the natural aging process. Disc desiccation literally translates to the drying out of the intervertebral spaces that separate your vertebrae. When this dehydration occurs across two or more spinal segments simultaneously, radiologists classify it as a multilevel phenomenon. While the term is inherently descriptive of tissue water content rather than a definitive disease state, it frequently serves as the earliest imaging hallmark of degenerative spinal changes. The vast majority of individuals who receive this diagnosis are unaware they have it until an unrelated scan is ordered. When symptoms do arise, they are highly manageable through evidence-based conservative strategies. This comprehensive guide explores the underlying biomechanics, clinical implications, and scientifically backed management protocols to help you navigate multilevel disc desiccation with clarity and confidence.
Understanding the Anatomy and Physiology of Intervertebral Discs
The human spinal column is a sophisticated mechanical structure composed of thirty-three stacked vertebrae separated by twenty-four mobile intervertebral discs. These discs are not merely passive spacers; they function as dynamic, shock-absorbing hydraulic cushions that enable complex multi-planar movements while protecting the central nervous system. Each healthy disc comprises three distinct anatomical components working in precise biomechanical harmony.
The nucleus pulposus sits at the center of the disc. During early adulthood, this gelatinous core is approximately 80% water, bound tightly by highly hygroscopic molecules called proteoglycans, particularly aggrecan. These proteoglycans create a negative osmotic pressure that continuously draws water into the disc, maintaining internal hydrostatic pressure and turgor. This pressurized core acts like a fluid ball bearing, evenly distributing compressive forces across the vertebral endplates.
Surrounding the nucleus is the annulus fibrosus, a highly organized, multi-layered ring of type I and type II collagen fibers oriented in alternating diagonal directions (lamellae). This cross-ply architecture provides remarkable tensile strength, preventing the nucleus from bulging outward under load while containing torsional stresses during twisting motions.
Finally, the cartilaginous endplates sit superiorly and inferiorly, anchoring the disc to the adjacent vertebral bodies. These semi-permeable plates serve as the critical gateway for nutrient and waste exchange. Since mature intervertebral discs are entirely avascular, they lack direct blood supply. Instead, they rely on a diffusion-driven process fueled by spinal movement. Mechanical loading and unloading create a pumping effect, forcing synovial fluid through the endplates to nourish disc cells and flush metabolic byproducts. This physiological pumping mechanism explains why prolonged immobility is profoundly detrimental to disc health.
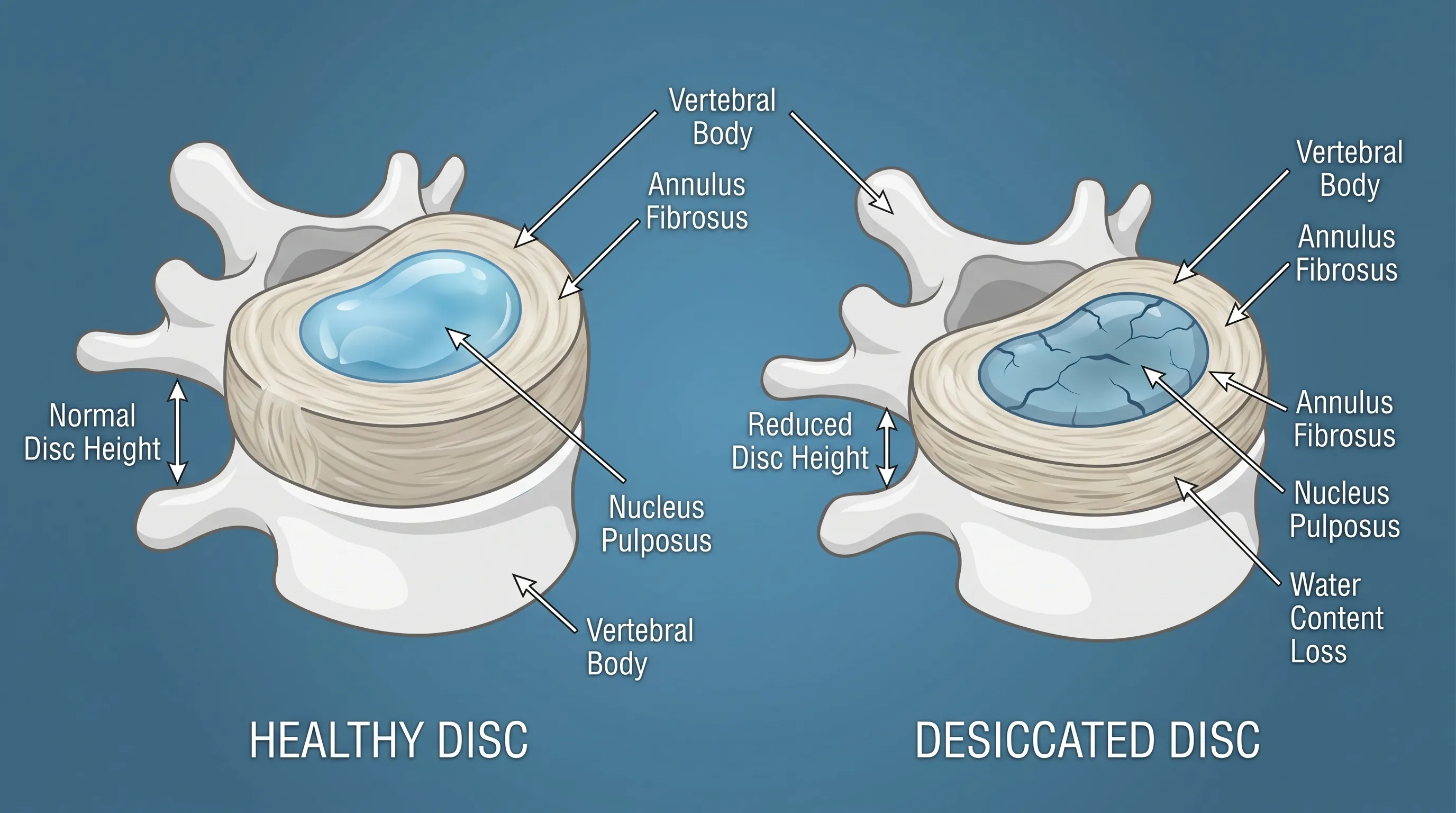
Understanding this delicate hydrodynamic system clarifies why fluid loss disrupts the entire spinal load-bearing architecture. When proteoglycans degrade, the disc loses its capacity to bind water, hydrostatic pressure drops, and the nucleus becomes fibrotic rather than gelatinous. Consequently, the annulus experiences abnormal shear forces, micro-tears develop, and spinal stability diminishes. Multilevel disc desiccation indicates that this biochemical dehydration has progressed across multiple segments, altering the kinetic chain of the entire spine.
What Is Multilevel Disc Desiccation?
The clinical definition of multilevel disc desiccation is straightforward yet frequently misunderstood by patients and non-specialized clinicians alike. In radiology, desiccation refers strictly to decreased water content within the disc matrix, visible on magnetic resonance imaging (MRI) as reduced signal intensity. When this finding is documented at two or more contiguous or non-contiguous spinal levels, the report specifies "multilevel" involvement. Common anatomical distributions include the lumbar spine (particularly L3-L4, L4-L5, and L5-S1) and the cervical spine (C4-C7), which bear the greatest mechanical loads and possess the highest degrees of mobility.
Clinical Definition vs. Degenerative Disc Disease
It is crucial to distinguish between a radiological observation and a clinical syndrome. Multilevel disc desiccation is essentially an MRI descriptor, not a standalone diagnosis. It represents the early to moderate structural manifestation of degenerative disc disease (DDD), which is the broader clinical condition encompassing pain, functional limitation, and neurological involvement. Many orthopedic specialists and neurosurgeons emphasize that imaging findings alone cannot dictate treatment plans. A patient with severe multilevel desiccation may experience zero pain, while another with minimal MRI changes may suffer debilitating symptoms due to central sensitization, muscular dysfunction, or facet joint arthropathy. The term DDD should only be applied when degenerative imaging findings correlate directly with reproducible clinical symptoms that impair daily function.
How MRI Findings Translate to Real-World Symptoms
When multilevel disc desiccation progresses to a point where it triggers symptoms, the clinical picture usually involves mechanical back or neck pain. As discs lose height, the vertebral bodies approximate, increasing compressive stress on the facet joints and surrounding ligamentous structures. The paraspinal musculature must work overtime to stabilize the compromised spinal segment, leading to fatigue, localized tenderness, and protective muscle spasms. If the height loss is significant enough to narrow the neural foramina (the openings where spinal nerves exit), radicular symptoms may develop. Understanding this progression demystifies the diagnostic process and shifts focus toward functional rehabilitation rather than chasing imaging abnormalities.
Pathophysiology and Primary Risk Factors
The cascade of events leading to fluid depletion within intervertebral spaces is multifactorial, involving genetic programming, mechanical stressors, biochemical degradation, and lifestyle choices. Modern spine research, including comprehensive twin studies and longitudinal epidemiological data, has fundamentally shifted our understanding of disc degeneration from a purely age-related inevitability to a modifiable physiological process.
Aging and Proteoglycan Depletion
The most significant predictor of disc desiccation is chronological age. Starting in the second decade of life, the nucleus pulposus undergoes gradual compositional changes. Vascularity that once permeated the juvenile disc completely regresses by early adulthood, leaving diffusion as the sole nutrient pathway. Over time, aggrecan molecules fracture into smaller fragments that wash out of the disc matrix. This proteoglycan depletion directly reduces the tissue's osmotic gradient, diminishing its water-binding capacity. By age 40, approximately 60% to 70% of adults demonstrate measurable disc desiccation on T2-weighted MRI, yet a substantial portion remains entirely asymptomatic. The rate of decline varies dramatically based on environmental and behavioral exposures.
Genetic Predisposition and Twin Studies
Heritability plays an unexpectedly dominant role in disc matrix resilience. Landmark research, such as the Twin Spine Study published in the Spine Journal, demonstrated that genetic factors account for 50% to 75% of the variance in lumbar disc degeneration. Specific polymorphisms in collagen type IX, vitamin D receptor genes, and matrix metalloproteinase promoters significantly influence how rapidly discs desiccate under normal physiological stress. Individuals with a strong family history of early-onset chronic back pain or spinal fusion surgeries often possess inherent vulnerabilities in disc matrix maintenance, making proactive lifestyle interventions even more critical.
Mechanical Stress, Posture, and Occupational Hazards
Biomechanical loading directly dictates disc nutrition and structural integrity. Repetitive axial loading, particularly when combined with flexion and torsion, generates shear forces that accelerate annular microtrauma. Occupations requiring heavy lifting, frequent bending, or prolonged vibration exposure (such as commercial driving or construction work) dramatically elevate desiccation risk. Poor postural habits, particularly sustained spinal flexion during prolonged sitting, increase intradiscal pressure to levels far exceeding standing or recumbent positions. This static loading compresses endplate vasculature, stifling the diffusion pump and creating a localized hypoxic environment that accelerates cellular apoptosis within the disc.
Lifestyle Choices: Smoking, Nutrition, and Sedentary Behavior
Among modifiable risk factors, tobacco use remains the most detrimental. Nicotine induces profound vasoconstriction of the vertebral endplate arteries, starving the disc of oxygen and nutrients required for proteoglycan synthesis. Carbon monoxide further reduces oxygen-carrying capacity in the bloodstream, compounding ischemic damage. Obesity introduces chronic, excessive axial loading; for every pound of excess body weight, approximately four pounds of additional mechanical pressure are transmitted to the lumbar spine. Conversely, sedentary behavior eliminates the dynamic movement necessary for disc nutrition, creating a paradoxical cycle where inactivity accelerates degenerative dehydration. Nutritional deficiencies, particularly low vitamin C, magnesium, and omega-3 fatty acids, impair collagen cross-linking and amplify inflammatory cascades that degrade disc matrix components.
Clinical Presentation and Symptom Progression
Recognizing the symptomatic patterns associated with multilevel disc desiccation empowers patients to seek appropriate care and differentiate mechanical back pain from systemic or neurological emergencies. While many individuals remain completely asymptomatic, those who experience clinical manifestations typically report a consistent constellation of findings.
Localized Axial Pain and Morning Stiffness
The hallmark symptom is dull, aching axial pain localized directly over the affected spinal region. Lumbar involvement typically presents as midline lower back discomfort that radiates subtly into the gluteal or posterior thigh regions, stopping above the knee. Cervical desiccation often causes persistent neck stiffness, occipital tension, and referred shoulder discomfort. Morning stiffness is particularly characteristic, as discs naturally rehydrate overnight during recumbency, temporarily expanding tissue volume. When transitioning to weight-bearing activities, the sudden load on rehydrated yet structurally compromised discs triggers inflammatory mediators and mechanoreceptor activation. Pain intensity typically worsens with prolonged sitting, forward bending, heavy lifting, or exposure to whole-body vibration, while supine positioning and gentle walking often provide immediate relief.
Radiculopathy and Nerve Compression
As multilevel disc desiccation progresses and disc height diminishes, the spinal foramina experience mechanical narrowing. This foraminal stenosis can impinge upon exiting nerve roots, generating radicular pain, paresthesia (pins and needles), numbness, or distal weakness. Lumbar radiculopathy (sciatica) follows specific dermatomal patterns: L4 nerve involvement typically causes medial leg pain and quadriceps weakness; L5 radiculopathy presents with lateral leg/foot discomfort and foot drop; S1 compression causes posterior calf pain and reduced Achilles reflex. Cervical radiculopathy follows similar principles, with C5-C7 nerve root impingement causing shoulder blade pain, arm tingling, and hand grip weakness. It is vital to note that radicular symptoms do not automatically indicate a herniated disc; foraminal collapse secondary to height loss from desiccation alone can produce identical neurological findings.
When to Seek Immediate Medical Attention
While multilevel disc desiccation rarely constitutes a medical emergency, certain red flags warrant urgent clinical evaluation. Progressive neurological deficits, including worsening muscle atrophy, inability to walk, or loss of fine motor coordination, require prompt imaging and specialist consultation. Bowel or bladder dysfunction, saddle anesthesia (numbness in the perineal region), or severe bilateral leg weakness indicate cauda equina syndrome, a rare but devastating condition requiring immediate surgical intervention. Additionally, unexplained weight loss, night pain that prevents sleep, fever, or a history of malignancy alongside back pain should trigger comprehensive diagnostic workup to rule out systemic pathology unrelated to disc degeneration.
Diagnostic Imaging and Grading Systems
Accurate diagnosis of multilevel disc desiccation relies heavily on advanced imaging modalities, though clinical correlation remains the gold standard for determining treatment necessity. Understanding how radiologists interpret spinal scans demystifies the diagnostic process and helps patients contextualize their reports accurately.
T2-Weighted MRI and the Dark Disc Sign
Magnetic resonance imaging is unequivocally the most sensitive and specific modality for evaluating disc hydration status. T2-weighted sequences specifically highlight water molecules within tissues, rendering hydrated structures bright white. A healthy intervertebral disc displays a hyperintense (bright) nucleus pulposus on T2 images, surrounded by a darker annulus. Disc desiccation manifests as decreased T2 signal intensity, commonly referred to as the "dark disc sign." Radiologists evaluate the severity of signal loss, disc height reduction, and bulging morphology across multiple levels. MRI also excels at visualizing soft tissue structures, allowing clinicians to assess nerve root compression, ligamentum flavum hypertrophy, and paraspinal muscle atrophy simultaneously.
Pfirrmann Grading Scale Explained
To standardize desiccation severity, radiologists utilize the Pfirrmann grading system, a validated five-tier classification widely adopted in orthopedic and neurosurgical literature. Grade I represents a healthy disc with homogeneous bright signal, well-defined structure, and normal height. Grade II shows slightly inhomogeneous signal with horizontal dark bands but preserved height. Grade III demonstrates inhomogeneous gray signal, indistinct nucleus-annulus distinction, and mild-to-moderate height loss. Grade IV reveals dark, inhomogeneous signal, collapsed structure, and significant height reduction. Grade V indicates complete desiccation, black signal, severe collapse, and often associated osteophyte formation. Multilevel disc desiccation typically spans Grades II through IV across multiple contiguous segments, providing clinicians with a quantifiable baseline for monitoring progression.

Complementary Imaging: X-Rays and CT Scans
While MRI dominates soft tissue assessment, conventional radiography and computed tomography serve complementary roles. Standing X-rays evaluate dynamic spinal alignment, disc space narrowing, endplate sclerosis, and osteophyte formation under weight-bearing conditions. They cannot visualize hydration but provide critical biomechanical context, especially when flexion-extension views assess segmental instability. CT scans excel at detailing bony anatomy, identifying facet joint arthrosis, calcified disc herniations, and precise foraminal dimensions. CT is rarely used to diagnose desiccation alone but proves invaluable when surgical planning requires detailed osseous mapping or when MRI contraindications exist.
| Imaging Modality | Primary Clinical Utility | Desiccation Detection Capability | Weight-Bearing Assessment | Radiation Exposure |
|---|---|---|---|---|
| MRI (T2-Weighted) | Gold standard for soft tissue, hydration, and neural compression | Excellent (Direct visualization of water content) | Limited (Typically supine) | None |
| Standing X-Ray | Spinal alignment, disc height, osteophytes, instability | Poor (Indirect inference from space narrowing) | Excellent | Low |
| CT Scan | Bony detail, foraminal calcification, surgical planning | Poor | Limited | Moderate to High |
Evidence-Based Treatment and Management Strategies
The cornerstone of managing multilevel disc desiccation is conservative, non-surgical rehabilitation. Over 90% of patients achieve significant symptom relief and functional restoration without invasive interventions. Treatment protocols emphasize active movement, biomechanical optimization, and long-term lifestyle modification rather than passive dependency on medications or procedures.
Conservative First-Line Therapies
Initial management focuses on pain modulation while preserving mobility. Short-term use of non-steroidal anti-inflammatory drugs (NSAIDs) or acetaminophen addresses acute inflammatory flares. Muscle relaxants may be prescribed temporarily for severe paraspinal spasms, though prolonged use is discouraged due to tolerance and sedation risks. If radicular symptoms dominate, neuromodulators such as gabapentin or pregabalin target neuropathic pain pathways. Activity modification plays a parallel role; patients are educated to avoid prolonged static postures, implement frequent movement breaks, and utilize proper biomechanics during daily tasks. The goal is not complete rest, but strategic movement optimization.
Physical Rehabilitation and Core Stabilization Protocols
Physical therapy represents the most potent disease-modifying intervention. Evidence strongly supports structured exercise programs focusing on motor control re-education, dynamic stabilization, and graded loading. Core stabilization exercises target the transverse abdominis, multifidus, pelvic floor, and diaphragm to create a coordinated muscular cylinder that unloads compromised discs. The McKenzie Method (Mechanical Diagnosis and Therapy) utilizes repeated spinal movements, typically extension, to centralize radiating pain and improve fluid dynamics. Flexion-intolerant patients often thrive on extension-biased routines, while those with stenosis or spondylolisthesis require flexion-dominant protocols. Therapists progressively advance patients through foundational exercises like bird-dogs, dead bugs, glute bridges, and modified side planks before introducing dynamic resistance training.
Pharmacological and Interventional Options
When conservative measures plateau, interventional pain management bridges the gap toward surgical evaluation. Epidural steroid injections deliver corticosteroids directly into the epidural space, reducing nerve root inflammation and breaking the pain-spasm cycle. Transforaminal approaches target specific irritated nerve roots, while interlaminar injections provide broader coverage. Facet joint injections or medial branch blocks address concurrent zygapophysial arthropathy, a common comorbidity with disc height loss. Radiofrequency ablation offers longer-term relief by thermally disrupting pain-transmitting nerve fibers. These procedures are strictly palliative, buying time for rehabilitative efforts to restore functional capacity.
Surgical Considerations and Realistic Expectations
Surgical intervention for multilevel disc desiccation alone is virtually nonexistent. Surgery is reserved for documented instability (spondylolisthesis), progressive neurological deficits, or intractable pain unresponsive to six or more months of aggressive conservative care. Options include microdiscectomy for localized herniation, posterior lumbar interbody fusion (PLIF) or transforaminal lumbar interbody fusion (TLIF) to restore disc height and achieve arthrodesis, and total disc replacement to preserve motion in select candidates. Patients must understand that surgery addresses mechanical failure or neural compression, not the underlying degenerative process. Postoperative rehabilitation remains identical in principle, emphasizing long-term movement integration and core resilience.
Prevention, Lifestyle Modifications, and Long-Term Spinal Health
Preventing the progression of multilevel disc desiccation requires integrating spine-sparing habits into daily routines. Unlike acute injuries, chronic disc degeneration responds profoundly to cumulative lifestyle choices. The following evidence-based strategies form the foundation of lifelong spinal resilience.
Daily Ergonomic Adjustments for Work and Home
Modern occupational environments frequently violate fundamental spinal biomechanics. Prolonged sitting in slouched postures places up to 275% greater compressive force on lumbar discs compared to standing neutral alignment. Correcting this requires intentional environmental design. Use chairs with adjustable lumbar support maintaining natural lordotic curvature. Position computer monitors at eye level to prevent forward head posture and cervical strain. Implement sit-stand workstations, alternating between seated and standing positions every 30 to 45 minutes to maintain dynamic nutrient diffusion. In vehicles, adjust seats to prevent hip flexion beyond 100 degrees, utilize lumbar rolls, and maintain knees slightly below hip level. When lifting, engage the hip hinge pattern, keeping loads close to the body center of gravity while avoiding combined flexion and rotation.
Exercise, Movement, and Mechanical Loading
Discs require cyclical mechanical stress to thrive. Complete avoidance of exercise paradoxically accelerates desiccation by eliminating the endplate pumping mechanism. Low-impact cardiovascular activities, including brisk walking, stationary cycling, elliptical training, and swimming, promote systemic circulation while maintaining spinal mobility without excessive joint impact. Aim for 150 minutes of moderate-intensity aerobic activity weekly. Incorporate daily flexibility routines targeting hip flexors, hamstrings, and thoracic spine to reduce compensatory lumbar strain. High-impact sports involving repetitive jumping, heavy Olympic lifting, or aggressive contact sports may exacerbate existing multilevel disc desiccation and require individualized risk-benefit analysis with sports medicine specialists.

Nutritional Support and Systemic Hydration
Optimal disc matrix maintenance depends on adequate systemic nutrition and hydration. Adult discs rely entirely on diffusion, meaning blood plasma composition directly influences cellular metabolism. Maintain daily water intake at approximately 30 to 35 milliliters per kilogram of body weight to support osmotic gradients. Discs naturally imbibe fluid during unloading phases, particularly overnight; systemic dehydration limits this rehydration capacity, exacerbating morning stiffness. Nutritionally, prioritize anti-inflammatory dietary patterns rich in omega-3 fatty acids (salmon, flaxseeds, walnuts), vitamin C (citrus, bell peppers, broccoli) for collagen synthesis, magnesium (leafy greens, almonds) for neuromuscular regulation, and high-quality protein for tissue repair. Limit refined carbohydrates, trans fats, and excessive sodium, which promote systemic inflammation and impair microvascular perfusion. Consider vitamin D supplementation if deficient, as adequate levels correlate with improved disc proteoglycan content in clinical studies.
Frequently Asked Questions
Is multilevel disc desiccation reversible?
Once proteoglycans and water content are depleted from the intervertebral disc matrix, the structural process cannot be fully reversed. However, clinical progression can be significantly halted, and remaining disc function optimized through targeted rehabilitation, posture correction, smoking cessation, and mechanical loading strategies. Treatment focuses on symptom resolution and functional preservation rather than histological regeneration.
Does multilevel disc desiccation always cause back pain?
No. Extensive epidemiological research demonstrates that disc desiccation is frequently asymptomatic, particularly in middle-aged populations. Pain arises only when dehydration leads to height loss, nerve compression, facet joint overload, or muscular fatigue. Imaging findings alone should never dictate treatment without clinical correlation.
What is the difference between disc desiccation and a herniated disc?
Desiccation refers to internal matrix dehydration and proteoglycan loss, visible as decreased MRI signal intensity. Herniation involves structural failure of the annulus fibrosus, allowing nucleus material to protrude into the spinal canal. While desiccation weakens disc integrity and increases herniation risk, they represent distinct pathological processes requiring different management approaches.
Can specific exercises help with multilevel disc desiccation?
Absolutely. Evidence-based core stabilization, controlled spinal extension, and graded loading exercises enhance nutrient diffusion, improve load distribution, and reduce compensatory muscle fatigue. Programs emphasizing transverse abdominis and multifidus activation are particularly effective. Consultation with a physical therapist ensures proper progression and avoids movements that exacerbate symptoms.
How does smoking affect multilevel disc desiccation?
Smoking causes severe vasoconstriction of the vertebral endplate arteries, drastically reducing oxygen and nutrient delivery to avascular discs. Carbon monoxide further impairs cellular metabolism. Chronic tobacco use accelerates proteoglycan degradation, increases inflammatory cytokine production, and doubles the risk of severe degenerative progression compared to non-smokers.
When is surgery considered for disc desiccation?
Surgery is exceptionally rare for desiccation alone. It is reserved for documented spinal instability, progressive neurological deficits, or intractable pain failing comprehensive conservative management. Procedures such as fusion or disc replacement address mechanical failure or neural compression, not the degenerative hydration process itself.
Key Takeaways
Multilevel disc desiccation is a common, often incidental MRI finding that reflects the natural biochemical aging of intervertebral discs. Understanding that imaging abnormalities do not equate to clinical disease empowers patients to approach management rationally. The majority of individuals achieve excellent outcomes through conservative strategies, including structured physical therapy, ergonomic optimization, smoking cessation, weight management, and targeted nutritional support. By prioritizing dynamic movement over prolonged static postures, maintaining systemic hydration, and engaging in evidence-based core rehabilitation, you can significantly slow degenerative progression and preserve lifelong spinal function. Always consult board-certified orthopedic or neurosurgical specialists for personalized evaluation, and remember that proactive lifestyle integration remains the most powerful tool for long-term spine health.

About the author
Dr. Flores is a board-certified diagnostic radiologist with a fellowship in neuroradiology. She works for a large teleradiology practice based in Phoenix, Arizona, where she interprets complex brain, spine, and head & neck imaging from hospitals across the country.