Feet Turn Purple When Sitting: Causes, Warning Signs, and Expert Guidance

Noticing that your feet turn purple when sitting can be unsettling, but understanding the underlying mechanisms behind this phenomenon can help separate harmless physiological responses from conditions that require medical intervention. Blood circulation in the lower extremities is a complex interplay of gravity, muscle contraction, vascular tone, and autonomic nervous regulation. When we remain seated for extended periods, venous blood naturally pools in the distal capillaries and venules of the feet, particularly if the legs are dependent. This accumulation of deoxygenated hemoglobin often manifests as a bluish or purplish hue, which typically resolves once movement resumes or posture changes. However, when this discoloration becomes persistent, painful, or asymmetrically distributed, it may signal an underlying vascular or systemic disorder. In this comprehensive guide, we will explore the physiological and pathological reasons behind foot discoloration, identify red flags that demand prompt clinical evaluation, outline evidence-based diagnostic protocols, and provide actionable lifestyle modifications to optimize lower extremity circulation. Whether you work at a desk, travel frequently, or manage chronic metabolic conditions, understanding why feet turn purple when sitting empowers you to take proactive steps toward long-term vascular wellness.
Understanding Why Feet Change Color When Sitting
To fully grasp why feet turn purple when sitting, it is essential to first understand the fundamental principles of peripheral circulation. The human cardiovascular system relies on a delicate balance between arterial delivery and venous return. While the heart pumps oxygen-rich blood downward through the arterial network, returning blood against gravity requires a sophisticated system of one-way venous valves, calf muscle contractions, and respiratory pressure changes. When you remain seated, several physiological shifts occur simultaneously that can alter the visible color of your skin.
The Physiology of Blood Circulation in the Lower Extremities
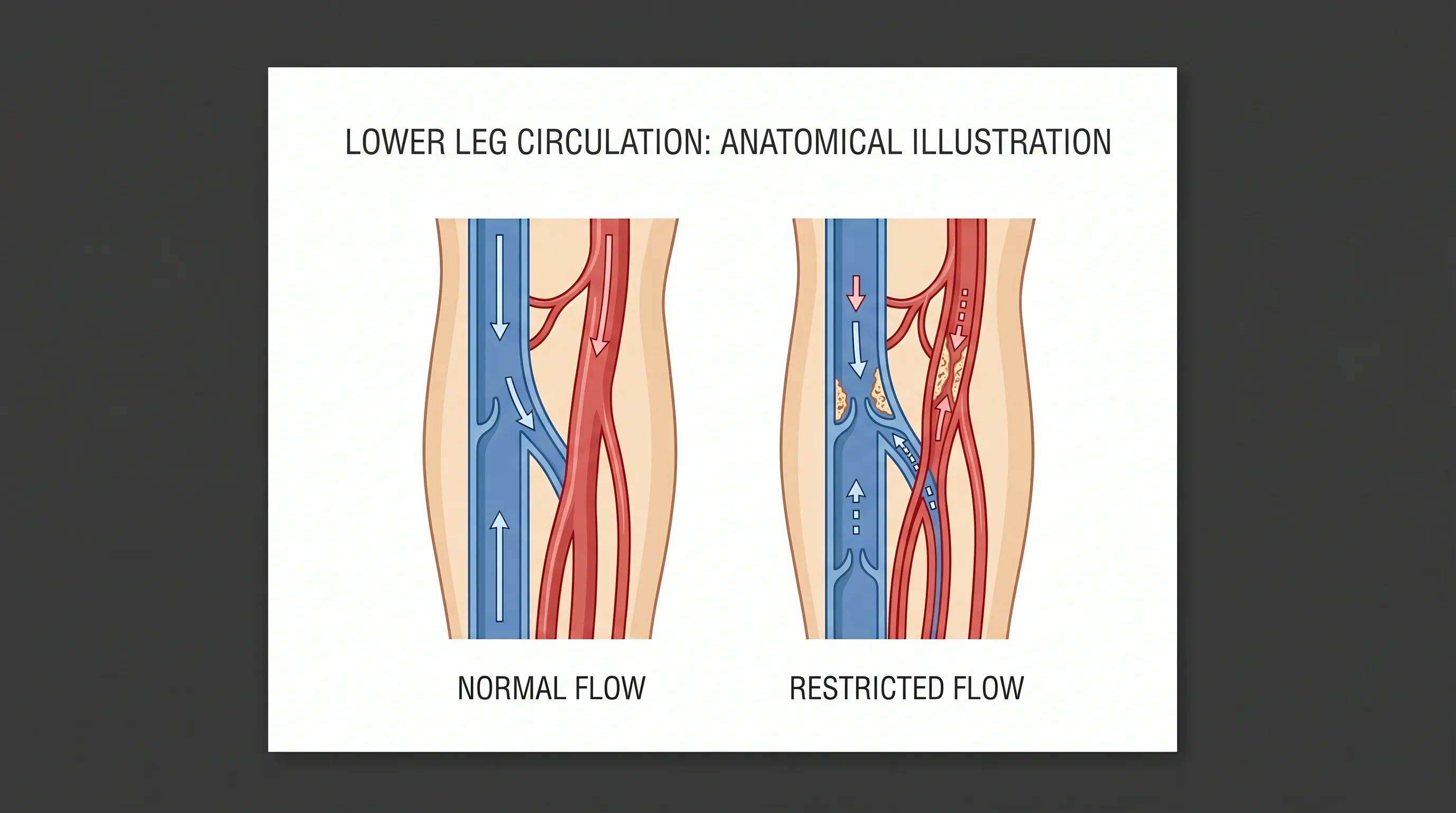
The arterial system delivers oxygenated blood from the heart through the femoral, popliteal, and tibial arteries down into a dense capillary network within the feet. As oxygen diffuses into the tissues, hemoglobin converts from oxyhemoglobin (bright red) to deoxyhemoglobin (dark red to purplish-blue). Under normal conditions, venous blood swiftly exits through the superficial and deep venous systems, preventing visible discoloration. However, when sitting for prolonged periods, hydrostatic pressure increases in the dependent limbs. This elevated pressure forces fluid into the interstitial space, causing mild edema, and slows venous outflow. The resulting stagnation allows deoxygenated blood to accumulate in superficial capillaries, which becomes visible through the thin skin of the dorsum of the foot. Research published by the National Institutes of Health indicates that venous pooling is a normal physiological response to immobility, but its clinical significance depends heavily on baseline vascular integrity, autonomic function, and ambient temperature.
How Gravity and Posture Affect Venous Return
Posture plays a critical role in determining circulatory efficiency. Sitting with knees bent at a ninety-degree angle compresses the popliteal vein and reduces the effectiveness of the soleal muscle pump. Additionally, crossing the legs or leaning forward excessively can mechanically obstruct venous pathways. Gravity exerts approximately 0.77 mmHg of pressure per centimeter of vertical distance from the heart. For an average adult, this translates to nearly 90 mmHg of hydrostatic pressure in the feet while seated upright. This substantial pressure gradient overwhelms venous valves over time, particularly if the valves are already weakened. Consequently, blood pools, and the characteristic purple or bluish tint emerges. Adjusting your chair height, using a footrest to alter the knee angle, and periodically flexing the ankles can dramatically reduce this gravitational burden. Ergonomic adjustments are among the most underutilized yet highly effective interventions for maintaining healthy circulation during sedentary activities.
Acrocyanosis and Benign Discoloration
Many individuals experience a harmless condition known as benign acrocyanosis, where the extremities exhibit persistent blue or purple discoloration without pain, swelling, or tissue damage. This condition is particularly common in women, adolescents, and people with naturally thin skin or lower basal body temperatures. Acrocyanosis occurs due to exaggerated peripheral vasoconstriction mediated by the sympathetic nervous system. When exposed to mild cold or prolonged sitting, arterioles in the skin constrict excessively, while deeper veins continue to pool blood slowly. The result is a visible purple hue that disappears rapidly upon warming or standing. Unlike pathological vascular disease, acrocyanosis does not lead to ulcers, gangrene, or progressive ischemia. If your feet turn purple when sitting in cool environments but quickly normalize after standing and warming up, and you experience no accompanying pain or skin changes, this is likely a benign physiological variant. Clinical resources from the Mayo Clinic note that monitoring for progression remains essential.
Common Medical Causes of Purple Feet While Seated
While transient discoloration can be entirely normal, persistent or worsening symptoms often point to underlying medical conditions. Vascular disorders, metabolic imbalances, and neurological factors can all compromise lower extremity perfusion. Recognizing these conditions early allows for targeted interventions that prevent irreversible tissue damage.
Peripheral Artery Disease (PAD)
Peripheral artery disease occurs when atherosclerotic plaques accumulate within the arteries supplying the legs and feet, progressively narrowing the lumen and restricting blood flow. Individuals with PAD often report that their feet turn purple when sitting, particularly when transitioning from standing to a seated position. The discoloration in PAD is frequently accompanied by cool skin temperature, diminished hair growth on the toes, shiny skin, and intermittent claudication during walking. When sitting, arterial inflow decreases due to already compromised vessel patency, while venous outflow continues relatively normally, creating a mismatch that highlights deoxygenated blood in superficial tissues. According to the American Heart Association, approximately 1 in 20 adults over 50 has PAD, with prevalence increasing significantly among smokers and individuals with diabetes. Diagnostic confirmation typically involves measuring the ankle-brachial index (ABI) and performing duplex ultrasonography to visualize plaque burden and blood flow velocities.
Chronic Venous Insufficiency (CVI)
In contrast to arterial disease, chronic venous insufficiency stems from malfunctioning venous valves that fail to prevent retrograde blood flow. Over time, this backward leakage causes chronic venous hypertension, leading to capillary dilation, hemosiderin deposition, and characteristic purple-brown pigmentation around the ankles and feet. When sitting, the hydrostatic column exerts continuous pressure on already weakened valves, exacerbating venous pooling and making the purple hue more pronounced. Patients with CVI frequently experience heavy legs, aching that worsens as the day progresses, varicose veins, and stasis dermatitis. If left untreated, CVI can progress to venous stasis ulcers, which are notoriously difficult to heal and carry a high recurrence rate. Clinical management focuses on reducing venous hypertension through compression therapy, weight optimization, and in severe cases, endovenous ablation or sclerotherapy.
Raynaud’s Phenomenon and Vasospastic Disorders
Raynaud’s phenomenon is characterized by episodic vasospasm of digital arteries in response to cold or emotional stress. During an episode, the toes and fingers undergo a classic triphasic color change: white (ischemia due to severe vasoconstriction), blue/purple (deoxygenation as blood stagnates), and red (reperfusion hyperemia). While traditionally affecting the fingers, Raynaud’s frequently involves the feet. Prolonged sitting, especially in air-conditioned environments, can trigger vasospastic responses that cause feet to turn purple even without extreme cold exposure. Primary Raynaud’s is typically benign, but secondary Raynaud’s associated with autoimmune conditions like systemic lupus erythematosus, scleroderma, or rheumatoid arthritis carries higher risks of digital ulceration and tissue necrosis. Thermographic studies and capillaroscopy are valuable tools for distinguishing primary from secondary forms.
Diabetes-Related Vascular Changes
Diabetes mellitus exerts profound effects on both microvascular and macrovascular circulation. Chronic hyperglycemia leads to glycation of vascular proteins, endothelial dysfunction, and accelerated atherosclerosis. Diabetic neuropathy further complicates circulation by impairing autonomic regulation of blood vessel diameter. Consequently, many individuals with diabetes notice that their feet turn purple when sitting due to impaired arteriolar dilation and sluggish venous return. The combination of poor perfusion and sensory neuropathy significantly elevates the risk of foot ulcers, infections, and delayed wound healing. Tight glycemic control, routine podiatric examinations, and strict foot care protocols are essential for mitigating these complications. Evidence consistently shows that multidisciplinary diabetes management reduces lower extremity amputation rates by up to 75% (CDC).
When to Seek Immediate Medical Attention
While occasional discoloration is often benign, certain presentations indicate urgent or emergent vascular compromise. Timely recognition of red flag symptoms can prevent irreversible tissue loss and systemic complications.
Red Flag Symptoms to Watch For
You should contact a healthcare provider promptly if foot discoloration is accompanied by severe or worsening pain, particularly pain that occurs at rest. Rest pain typically indicates critical limb ischemia, a stage of PAD where tissue oxygen demand cannot be met even during minimal activity. Other warning signs include unilateral swelling, which may suggest deep vein thrombosis (DVT), skin breakdown, open ulcers, or foul-smelling discharge. A sudden onset of cold, pale, or mottled extremities warrants emergency evaluation for acute arterial occlusion. Additionally, if discoloration fails to resolve after elevation, movement, or warming, or if it spreads proximally toward the calves, immediate clinical assessment is mandatory.
Differentiating Between Temporary and Chronic Discoloration
Temporary discoloration typically appears symmetrically, fades within minutes of standing or walking, and lacks accompanying symptoms like pain, numbness, or temperature asymmetry. Chronic discoloration, however, persists despite positional changes, may be localized or asymmetrical, and is frequently paired with skin texture changes such as thickening, scaling, or hair loss. Tracking symptom duration, triggers, and progression using a simple health journal can provide clinicians with valuable diagnostic clues. If you frequently observe that feet turn purple when sitting and the color remains for over an hour after resuming normal activity, scheduling a vascular assessment is strongly advised.
Diagnostic Approaches and Clinical Evaluation
Accurate diagnosis of lower extremity discoloration requires a systematic clinical approach combining patient history, physical examination, and targeted diagnostic testing.
Physical Examination and Patient History
Clinicians begin by obtaining a comprehensive history, including symptom onset, duration, occupational habits, smoking status, family history of vascular disease, and comorbid conditions like hypertension or diabetes. The physical examination focuses on comparing bilateral pulses (dorsalis pedis and posterior tibial), assessing capillary refill time (normally under 3 seconds), checking skin temperature with the back of the hand, and evaluating for edema, varicosities, or trophic changes. The Buerger’s test is a classic bedside maneuver where the clinician elevates the leg to 45 degrees and observes for pallor, then has the patient dangle the leg to assess rubor or cyanosis. This simple test provides immediate insight into arterial sufficiency and venous competence.
Non-Invasive Vascular Testing (ABI, Ultrasound)
Non-invasive modalities are the cornerstone of vascular diagnostics. The ankle-brachial index (ABI) compares systolic blood pressure at the ankle to that in the arm. Values between 0.9 and 1.3 are normal, while readings below 0.9 indicate arterial insufficiency. Values above 1.3 suggest medial calcification, common in diabetic patients, requiring alternative testing like toe-brachial index (TBI). Duplex ultrasonography visualizes blood flow velocity, valve function, and plaque morphology in real time. Magnetic resonance angiography (MRA) or computed tomography angiography (CTA) may be utilized for surgical planning if severe arterial disease is confirmed. These tests help clinicians pinpoint the exact level and severity of circulatory impairment when patients report that feet turn purple when sitting consistently.
Blood Work and Metabolic Panels
Laboratory investigations complement imaging and physical findings. A comprehensive metabolic panel, lipid profile, hemoglobin A1c, and fasting glucose provide insight into cardiovascular risk factors. Inflammatory markers like C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) can indicate vasculitis or autoimmune involvement. Coagulation panels are essential if hypercoagulable states or venous thrombosis are suspected. Thyroid function tests may be ordered, as hypothyroidism can impair peripheral circulation and mimic vascular insufficiency. Together, these results guide personalized treatment strategies.
Lifestyle Modifications and Home Care Strategies
Implementing evidence-based lifestyle changes can dramatically improve peripheral circulation and reduce discoloration episodes. These strategies are safe, cost-effective, and synergize well with medical treatments.
Proper Seating Posture and Ergonomic Adjustments
Your workstation setup directly impacts lower extremity hemodynamics. Avoid chairs with rigid edges that press against the posterior thighs. Use adjustable seating with lumbar support and ensure feet rest flat on the floor or a contoured footrest. Keep knees slightly below hip level to reduce venous compression. Avoid sitting with legs crossed, as this position increases popliteal pressure by up to 40%. Setting a timer to remind yourself to shift position every 30 to 45 minutes encourages muscle pump activation and prevents prolonged stagnation. Ergonomic assessments conducted by occupational therapists have demonstrated measurable improvements in venous return and symptom reduction among office workers.
Leg Elevation and Movement Breaks
Gravity-assisted drainage is highly effective for venous pooling. Elevating your legs above heart level for 15 to 20 minutes, two to three times daily, facilitates rapid venous and lymphatic return, reducing edema and purple discoloration. Incorporating micro-movements such as ankle pumps, toe curls, and calf raises while seated maintains continuous blood flow. Walking for just 5 minutes every hour dramatically improves endothelial nitric oxide production, promoting vasodilation and optimal perfusion. The World Health Organization emphasizes that reducing sedentary behavior and breaking up prolonged sitting periods are critical for maintaining systemic and peripheral vascular health. If your daily routine requires prolonged sitting, scheduling deliberate movement breaks should be non-negotiable.
Temperature Management and Footwear Choices
Cold exposure triggers sympathetic vasoconstriction, worsening discoloration. Maintaining ambient room temperature between 68–72°F (20–22°C) prevents peripheral chilling. Wear breathable, moisture-wicking socks made from merino wool or bamboo blends, avoiding tight elastic bands that restrict superficial venous drainage. Choose footwear with adequate toe box space and cushioned arch support to prevent mechanical compression. Avoid high heels and narrow shoes during extended seated periods, as they alter biomechanics and impede natural muscle pump function. Consistent temperature regulation and proper footwear significantly enhance baseline circulation.
Medical Interventions and Professional Treatments
When lifestyle measures prove insufficient, targeted medical interventions address underlying pathology and restore hemodynamic balance.
Pharmacological Options
Medication selection depends on the diagnosed etiology. For PAD, antiplatelet agents like aspirin or clopidogrel reduce cardiovascular events, while statins stabilize atherosclerotic plaque and improve endothelial function. Cilostazol, a phosphodiesterase inhibitor, specifically alleviates claudication symptoms and promotes peripheral vasodilation. In Raynaud’s phenomenon, calcium channel blockers such as nifedipine or amlodipine reduce vasospastic frequency and severity. Diabetic patients benefit from strict glycemic control agents alongside SGLT2 inhibitors or GLP-1 receptor agonists, which have demonstrated cardiovascular protective effects. Pharmacotherapy should always be supervised by a licensed healthcare provider to monitor efficacy and prevent adverse interactions.
Compression Therapy
Graduated compression stockings remain the gold standard for managing venous insufficiency and preventing dependent edema. These garments apply highest pressure at the ankle (typically 20–30 mmHg or 30–40 mmHg) with gradual reduction proximally, creating a physiological gradient that propels blood upward. Clinical trials confirm that consistent compression use reduces leg heaviness, decreases discoloration, and prevents ulcer recurrence by up to 60%. Proper fitting by a certified orthotist ensures optimal pressure distribution and patient comfort. Compression should be worn daily, removed only at night, and replaced every 3 to 6 months as elasticity diminishes. Guidelines from the Society for Vascular Surgery strongly recommend compression as a first-line conservative treatment for venous pathology.
When Surgery Becomes Necessary
Advanced vascular disease may require procedural intervention. Endovascular techniques like balloon angioplasty, stent placement, and atherectomy restore patency in occluded arteries with minimally invasive approaches, resulting in shorter recovery times. Venous procedures such as endovenous laser ablation (EVLA), radiofrequency ablation (RFA), and microphlebectomy remove incompetent saphenous veins, eliminating reflux and venous hypertension. Bypass surgery utilizing autologous saphenous or synthetic grafts remains the definitive treatment for extensive multi-level arterial occlusions. Surgical candidates undergo thorough risk stratification, including cardiac stress testing and renal function assessment, to optimize outcomes. Postoperative care emphasizes early ambulation, compression, and aggressive risk factor modification.
| Feature | Benign Postural Discoloration | Pathological Vascular Disease |
|---|---|---|
| Onset | Gradual, triggered by prolonged sitting or cool temps | May be acute or chronic, often progressive |
| Symmetry | Usually bilateral and symmetrical | Often unilateral or asymmetric |
| Pain Level | None or mild heaviness | Rest pain, cramping, burning, or sharp pain |
| Resolution | Rapid upon standing, walking, or warming | Persists despite elevation or temperature change |
| Skin Changes | Normal texture, hair, and temperature | Shiny skin, hair loss, ulcers, temperature asymmetry |
| Clinical Action | Lifestyle optimization, monitoring | Urgent evaluation, imaging, targeted therapy |

Frequently Asked Questions
Is it dangerous if my feet occasionally look slightly blue or purple while working at a desk?
Occasional mild discoloration is usually not dangerous, particularly if you sit for extended periods without moving. Gravity naturally pools blood in the lower extremities, and deoxygenated blood gives the skin a bluish-purple appearance. If the color fades quickly after standing or walking, and you experience no pain, numbness, or swelling, it is likely a normal physiological response. However, implementing regular movement breaks and ergonomic adjustments can prevent unnecessary venous pooling and maintain optimal circulation.
Can vitamin deficiencies cause foot discoloration?
Certain deficiencies can indirectly affect circulation. Vitamin B12 deficiency, for instance, may lead to peripheral neuropathy and impaired microvascular function. Severe iron-deficiency anemia reduces oxygen-carrying capacity, which can make skin appear pale or slightly bluish in extremities. However, isolated purple feet are rarely caused solely by nutritional gaps. A comprehensive evaluation including complete blood count, vitamin panels, and vascular testing ensures accurate diagnosis rather than relying on supplementation alone.
Does hydration impact circulation in the feet?
Adequate hydration is crucial for optimal blood viscosity and endothelial health. Dehydration increases hematocrit levels, making blood thicker and more resistant to flow through narrow peripheral vessels. This can exacerbate discoloration and delay venous return. Consuming approximately 2 to 3 liters of water daily, depending on body size, activity level, and climate, maintains ideal rheological properties for blood flow. Electrolyte balance, particularly sodium and potassium, further supports proper muscle contraction and vascular tone, directly influencing lower extremity perfusion.
Are there specific exercises that target foot and ankle circulation?
Yes, targeted exercises significantly enhance the calf and foot muscle pumps. Ankle circles, alphabet tracing with toes, heel raises, and seated marching activate venous valves and promote lymphatic drainage. Incorporating resistance band toe curls improves intrinsic foot muscle strength, which supports arch integrity and enhances pump efficiency. Studies in vascular rehabilitation journals demonstrate that 15 minutes of daily lower extremity exercises can improve ABI readings and reduce discoloration frequency within 6 to 8 weeks of consistent practice.
Should I avoid sitting completely if I notice my feet change color?
Complete avoidance of sitting is neither practical nor necessary. Instead, adopt a dynamic sitting strategy. Alternate between sitting, standing, and brief walking intervals throughout the day. Use sit-stand desks when possible, and ensure your seated posture does not compress popliteal or femoral vessels. The goal is to prevent static immobility, not eliminate sitting entirely. Properly managed, seated activities pose minimal risk when balanced with intentional movement and ergonomic support.
Conclusion
Observing that feet turn purple when sitting can range from a completely normal physiological response to a clinical indicator of underlying vascular compromise. Understanding the distinction between benign postural pooling and pathological conditions like peripheral artery disease, chronic venous insufficiency, or vasospastic disorders is essential for maintaining long-term lower extremity health. By recognizing red flag symptoms, pursuing timely diagnostic evaluation, and implementing evidence-based lifestyle modifications, individuals can significantly improve circulation, reduce discoloration episodes, and prevent progressive tissue damage. Whether through ergonomic seating adjustments, graduated compression therapy, structured exercise routines, or targeted medical interventions, proactive management empowers patients to take control of their vascular wellness. Always consult a qualified healthcare provider for persistent, painful, or asymmetrical discoloration, as early intervention yields the best clinical outcomes. Prioritizing foot circulation today ensures mobility, comfort, and overall health for years to come.
About the author
Marcus Thorne, MD, is a board-certified interventional cardiologist and a fellow of the American College of Cardiology. He serves as the Chief of Cardiology at a major metropolitan hospital in Chicago, specializing in minimally invasive cardiac procedures.