Do Cavities Hurt? Understanding Tooth Pain, Progression, and Evidence-Based Prevention

Tooth decay remains one of the most pervasive chronic conditions worldwide, affecting individuals across every demographic and age group. Yet, despite its ubiquity, a surprising number of people delay professional care because they operate under the misconception that dental problems must always be accompanied by noticeable discomfort. This leads to a critical question that surfaces in dental clinics and online health searches alike: do cavities hurt? The medical reality is nuanced, deeply tied to the biological architecture of the tooth, and directly proportional to how far decay has penetrated the dental structure. Understanding the precise timeline of cavity formation, recognizing the subtle early warning signs, and implementing evidence-based preventive protocols can mean the difference between a simple, painless intervention and a complex, costly restorative procedure. The following comprehensive guide explores the physiological mechanisms behind tooth decay, clarifies exactly when and why pain occurs, and provides actionable, clinically validated strategies to protect your smile and preserve long-term oral health.
The Short Answer to Do Cavities Hurt?
When evaluating whether do cavities hurt in the earliest phases, the clinical consensus from leading dental authorities is clear: early cavities often produce zero symptoms. According to the Mayo Clinic, "When a cavity is just beginning, you may not have any symptoms at all." This painless window can last for months or even years, which is why routine dental examinations remain the gold standard for early detection. Pain typically emerges only after the protective outer layer of enamel has been sufficiently compromised, allowing decay to advance into the softer, nerve-sensitive dentin or the innermost pulp chamber.
The progression of dental discomfort follows a predictable biological trajectory. Initial mineral loss causes no physical sensation because enamel contains zero nerve endings. As decay breaches this hard outer shell, microscopic exposure of the underlying dentin triggers transient sensitivity, particularly in response to thermal changes or sugary foods. Once bacteria and acidic byproducts infiltrate the pulp, significant pain develops. The pulp houses dense concentrations of nerves and blood vessels within a rigid, unyielding chamber. As infection triggers inflammation, swelling occurs with nowhere to expand, generating intense internal pressure that compresses nerves and radiates outward as severe toothache. In advanced, untreated cases, pain may extend beyond the tooth itself, affecting surrounding bone, adjacent teeth, and even causing facial swelling or systemic symptoms. The short answer, therefore, is that while early-stage cavities rarely hurt, progressing and advanced decay absolutely does, and the intensity of pain correlates directly with the depth of tissue destruction.
Understanding the Anatomy of a Tooth and How Decay Begins
To fully comprehend the answer to do cavities hurt, it is essential to understand the microscopic and macroscopic architecture of human teeth and the exact biological mechanisms that drive caries formation. Teeth are composed of multiple distinct layers, each with varying levels of hardness, porosity, and nerve density. The National Institute of Dental and Craniofacial Research (NIDCR/NIH) describes tooth decay as a continuous "tug-of-war" between destructive acid production and the mouth's natural remineralization processes.
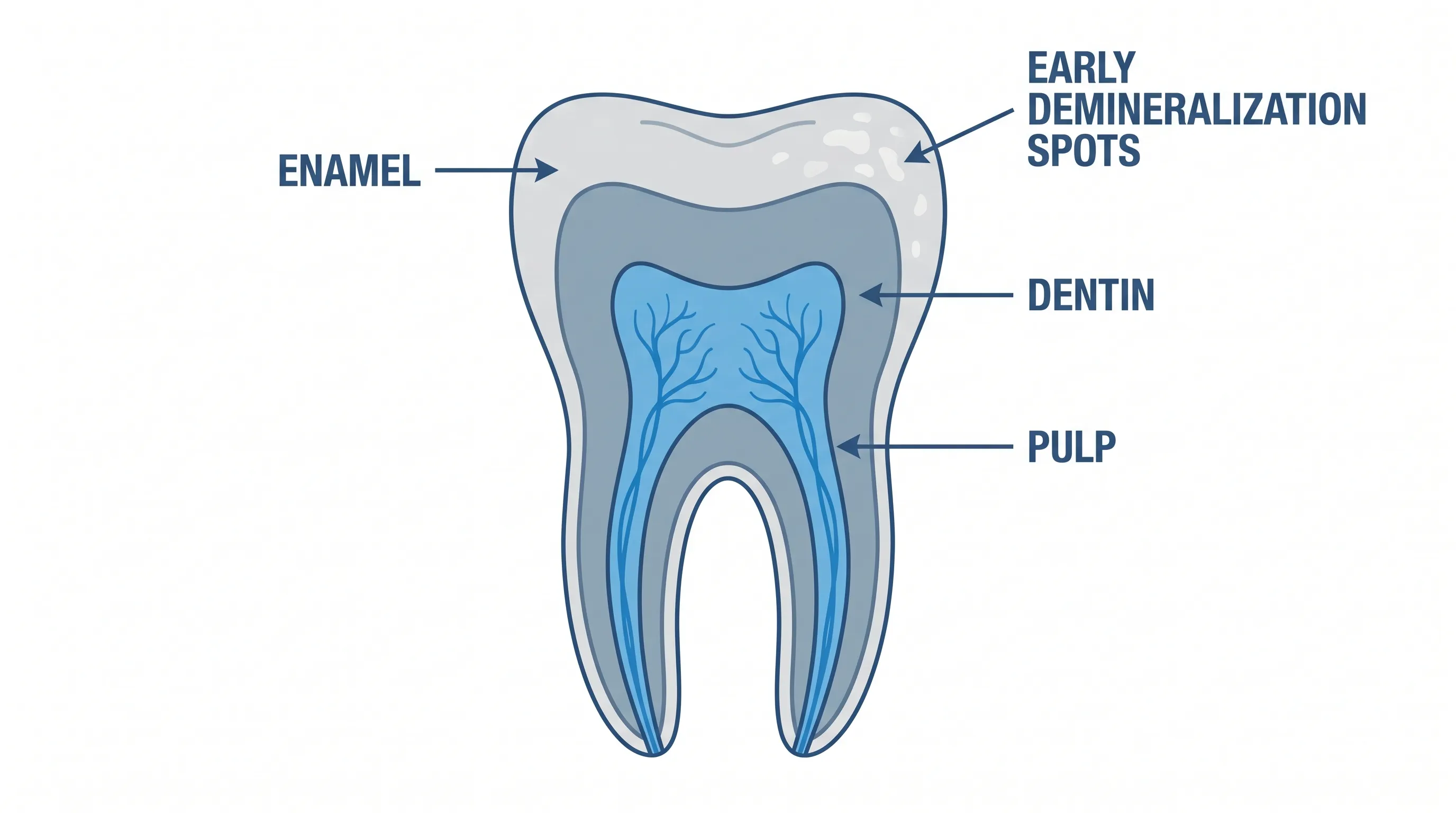
The Three Critical Layers: Enamel, Dentin, and Pulp
The outermost layer of a tooth is enamel, the hardest substance in the human body. Despite its remarkable durability, enamel is entirely acellular and avascular, meaning it lacks blood flow and nerve tissue. This biological design explains why surface-level erosion and early demineralization remain completely painless. Beneath the enamel lies dentin, a calcified tissue that is significantly softer and more porous than enamel. Dentin contains microscopic channels called tubules that extend directly to the pulp. The innermost layer, the pulp, contains a highly vascularized and innervated network of connective tissue, blood vessels, and sensory nerves. When decay reaches the pulp, pain becomes severe and persistent.
The Bacterial Tug-of-War Explained by the NIH
According to authoritative research from the NIDCR/NIH, tooth decay is fundamentally an infection driven by specific strains of oral bacteria, primarily Streptococcus mutans and Lactobacillus species. These microorganisms colonize the teeth by forming plaque, a clear, sticky biofilm that adheres to tooth surfaces. When you consume carbohydrates, sugars, or fermentable starches, plaque bacteria metabolize these substrates and secrete organic acids as metabolic byproducts. These acids rapidly lower the local pH around the tooth surface, initiating demineralization by dissolving calcium and phosphate crystals out of the enamel. The body's natural defense relies on saliva, which buffers acids, supplies minerals for repair, and washes away food debris. When acid attacks consistently outpace saliva's remineralization capacity, the protective balance tips in favor of destruction, initiating the cavity cascade.
The Pain Progression: How Cavities Evolve From Silent to Severe
The timeline of cavity-related discomfort is highly structured, progressing through four clinically defined stages. Understanding these stages clarifies exactly when and why pain emerges, reinforcing why the question of do cavities hurt must be evaluated in the context of disease progression rather than as a static yes-or-no scenario.
Stage 1: Demineralization and White Spots (No Pain)
The initial phase involves the leaching of essential minerals from the enamel matrix. Clinically, this appears as chalky white spots on the tooth surface. Because enamel remains intact and nerve-free, patients experience absolutely no pain. At this stage, the process is entirely reversible. Consistent fluoride exposure, reduced sugar frequency, and optimized oral hygiene can halt demineralization and stimulate remineralization, effectively preventing a permanent cavity from forming.
Stage 2: Enamel Breach and Early Dentin Exposure
As acid erosion continues, the enamel structure weakens and eventually collapses, creating a physical defect or early cavity. Once the decay penetrates into the dentin layer, patients typically begin experiencing intermittent sensitivity. The exposed dentinal tubules allow thermal, chemical, and tactile stimuli to reach the pulp more rapidly. This stage answers the core question: do cavities hurt at this phase? Yes, but usually as a brief, sharp sensitivity rather than constant throbbing. The discomfort often resolves quickly once the triggering substance is removed.
Stage 3: Pulp Inflammation and Nerve Compression
When decay advances deep into the pulp chamber, the inflammatory response escalates dramatically. Bacterial toxins invade the pulp tissue, causing vasodilation and increased blood flow. Because the pulp is encased in rigid dentin and enamel, the resulting edema generates intense hydrostatic pressure. This pressure compresses sensory nerve endings, producing severe, lingering pain that may wake patients at night, worsen when lying down, or occur spontaneously without external triggers. Pain at this stage typically indicates irreversible pulpitis, requiring immediate professional intervention.
Stage 4: Abscess Formation and Referred Pain
If pulp necrosis occurs without treatment, bacterial infection exits through the apex of the tooth root into the surrounding alveolar bone and periodontal ligament. This triggers the formation of a periapical abscess, characterized by intense, constant, pulsating pain that often radiates to the jaw, ear, or temples. Swelling, pus formation, and bone destruction may occur. At this advanced stage, pain may temporarily diminish as the nerve completely dies, but the underlying infection continues to spread, posing serious systemic risks. This progression underscores why waiting for pain before seeking care is a clinically dangerous strategy.
Recognizing the Warning Signs Before Pain Starts
Since early decay is frequently asymptomatic, relying solely on pain as an indicator of dental disease leaves patients vulnerable to advanced damage. Proactive recognition of subtle warning signs can facilitate timely intervention before cavities become painful. Common early indicators include persistent plaque accumulation, visible white or brown discolorations, mild sensitivity that resolves quickly, food trapping in specific areas, and a rough texture detectable with the tongue or dental explorer. The NHS emphasizes that "tooth decay may not cause any symptoms at first," making routine visual and radiographic examination essential.
Patients should also monitor lifestyle factors that accelerate decay risk. Frequent grazing, chronic dry mouth, high-stress diets rich in refined carbohydrates, and inconsistent brushing/flossing routines significantly increase the likelihood of silent enamel breakdown. Regular dental visits allow practitioners to use diagnostic technologies like bitewing radiographs, laser fluorescence devices, and transillumination to detect interproximal and occlusal decay long before it causes symptoms. Early intervention at this stage typically requires only fluoride application or minimally invasive sealants, preserving natural tooth structure and preventing future discomfort.
Why Early Cavities Often Fly Under the Radar
The biological silence of early cavities stems directly from human dental evolution. Enamel's lack of innervation was advantageous for ancestral diets but becomes a liability in modern environments where refined sugars are continuously available. The brain receives zero nociceptive signals from enamel demineralization, creating a false sense of dental health even as mineral loss progresses. Additionally, the oral cavity naturally adapts to gradual changes. Minor structural defects are quickly covered by plaque or food debris, masking visual and tactile cues. This adaptive silence explains why do cavities hurt only after substantial tissue compromise has already occurred. By the time pain emerges, the disease has progressed from a reversible mineral imbalance to irreversible structural destruction. Understanding this biological blind spot is critical for shifting patient behavior from reactive pain management to proactive preventive maintenance.
Evidence-Based Prevention Strategies to Stop Decay
Preventing cavities requires a multifaceted approach that addresses bacterial load, dietary frequency, enamel resilience, and mechanical plaque removal. Authoritative guidelines from the Mayo Clinic, NHS, and NIDCR provide a robust, clinically validated framework for cavity prevention.
Daily Oral Hygiene Protocols
Mechanical disruption of dental plaque remains the cornerstone of cavity prevention. Brushing teeth at least twice daily with a soft-bristled brush and fluoride toothpaste effectively removes surface biofilm. The NHS specifically advises to "spit after brushing, do not rinse," as immediate rinsing washes away concentrated fluoride that needs time to integrate into the enamel matrix. Daily interdental cleaning using floss, interdental brushes, or water flossers targets the proximal surfaces where approximately forty percent of all cavities originate, as standard brushing cannot adequately penetrate these narrow spaces.
Dietary Adjustments and Sugar Timing
Dietary modification focuses not just on sugar reduction, but on controlling the frequency of acid attacks. Every time fermentable carbohydrates are consumed, plaque bacteria produce acid that remains active for twenty to thirty minutes. Continuous snacking or sipping sugary or acidic beverages creates a near-constant acidic environment that prevents enamel recovery. Consolidating carbohydrate consumption into distinct meal periods, choosing whole foods over processed snacks, drinking water instead of sweetened beverages, and chewing xylitol-containing gum after meals can significantly reduce cariogenic exposure.
The Role of Fluoride and Sealants
Fluoride functions as the most potent anti-caries agent available. As noted by the NIDCR, fluoride prevents mineral loss, replaces lost minerals during early demineralization, and inhibits bacterial acid production. Drinking fluoridated water, which serves approximately sixty-three percent of the U.S. population according to public health data, provides continuous low-dose protection. Professional fluoride varnishes and prescription-strength toothpaste offer additional defense for high-risk patients. Dental sealants applied to the deep pits and fissures of molars create a physical barrier that blocks food and bacteria from settling into vulnerable grooves, dramatically reducing occlusal cavity formation in both children and adults.

Professional Treatment Options Based on Cavity Depth
When preventive measures are insufficient and decay has already initiated structural damage, professional dental intervention becomes necessary. Treatment selection depends entirely on the depth of the lesion, symptom severity, and remaining tooth structure integrity. The following table outlines the standard treatment pathways corresponding to decay progression:
| Decay Stage | Tissue Involved | Symptoms | Standard Treatment |
|---|---|---|---|
| Initial Demineralization | Enamel Surface | None / Mild White Spots | High-concentration fluoride varnish, prescription toothpaste, dietary counseling |
| Early Cavity | Enamel to Dentin Junction | Intermittent sensitivity to sweet/cold | Composite resin filling, glass ionomer, or minimally invasive restoration |
| Moderate to Deep Decay | Dentin Pulp Proximity | Lingering sensitivity, sharp pain on biting | Indirect pulp capping, full composite or ceramic filling, possible onlay |
| Pulp Involvement | Pulp Chamber / Canals | Spontaneous throbbing pain, night pain, heat sensitivity | Root canal therapy, post/core restoration, crown placement |
| Severe Structural Loss | Pulp Necrosis / Root Abscess | Swelling, constant pain, pus, bone loss | Extraction, bone grafting, implant or bridge rehabilitation |
Reversing Early Lesions with Fluoride Therapy
When decay has not yet cavitated the enamel surface, professional fluoride treatments can arrest the disease process. Dental varnishes containing 22,600 ppm fluoride adhere to the tooth, releasing ions that integrate into the hydroxyapatite crystal lattice, forming fluorapatite. This modified crystal structure is significantly more resistant to acid dissolution than natural enamel. Combined with optimized home care, early lesions can remineralize and regain surface hardness without requiring drilling or restoration.
Fillings and Restorative Dentistry
Once the enamel architecture collapses, bacteria gain permanent access to deeper tooth structures. At this point, mechanical removal of decayed tissue is mandatory to eliminate the infection reservoir. Dentists use high-speed burs, hand instruments, or air abrasion to remove compromised dentin, sterilize the cavity preparation, and restore function using biocompatible materials. Modern composite resins bond directly to tooth structure, preserving healthy enamel and providing excellent aesthetic integration with natural dentition.
Root Canals and Extractions for Advanced Decay
When infection reaches the pulp, root canal therapy (endodontic treatment) becomes the standard of care. This procedure involves accessing the pulp chamber, completely removing necrotic or inflamed tissue, disinfecting the intricate root canal system with antimicrobial irrigants, and hermetically sealing the space with gutta-percha. The treated tooth is then restored with a crown to withstand functional forces and prevent fracture. If decay has destroyed too much structure for successful restoration, or if periodontal support is severely compromised, extraction may be recommended. Modern prosthetic options including implants, bridges, and removable appliances ensure functional and aesthetic rehabilitation following tooth loss.
When to Schedule an Emergency Dental Visit
Timing professional care correctly is crucial for preventing irreversible damage and managing severe pain. The Mayo Clinic advises: "You may not be aware that a cavity is forming. That's why it's important to have regular dental checkups and cleanings, even when your mouth feels fine. But if you have a toothache or mouth pain, see your dentist as soon as possible." Immediate consultation is warranted if you experience spontaneous tooth pain that lasts longer than a few hours, pain that worsens when lying down, facial swelling, gum tenderness or pus discharge, fever accompanying dental discomfort, or visible dark holes in your teeth. Delaying treatment at these stages increases the risk of pulp necrosis, abscess formation, systemic infection, and more complex restorative requirements. The NHS similarly recommends seeking prompt dental evaluation for suspected decay and maintaining routine checkups every twelve months for minors and every two years for adults, though high-risk patients typically benefit from six-month intervals.
Frequently Asked Questions
Do all cavities hurt immediately?
No. Early-stage cavities typically cause no pain or noticeable symptoms. Tooth enamel lacks nerve endings, so initial demineralization remains painless. Pain usually begins only after decay penetrates the enamel and reaches the dentin or pulp layers.
What does a cavity pain feel like as it worsens?
As decay progresses, patients typically experience mild sensitivity to temperature or sweetness first. If untreated, this escalates to sharp, persistent toothaches, pain when biting down, and eventually throbbing, constant pain that may disrupt sleep and radiate to the jaw or head.
Can early cavities be reversed without fillings?
Yes. In the initial demineralization phase (white spot lesions), fluoride treatments, improved oral hygiene, and dietary modifications can remineralize enamel and halt decay before a physical cavity forms. Once the enamel structure collapses into a true cavity, restorative dentistry is required.
Why does a cavity hurt when I eat or drink something cold?
When enamel thins or a cavity breaches the surface, microscopic tubules in the underlying dentin become exposed to temperature changes and sweet/acidic stimuli. These tubules connect directly to the tooth's nerve center, causing rapid, sharp sensitivity.
At what stage should I see a dentist for tooth pain?
You should see a dentist immediately upon experiencing persistent toothache, sensitivity lasting longer than a few seconds, or visible holes in your teeth. However, because early decay is often painless, routine checkups every six to twelve months are essential for early detection before symptoms appear.
Can a cavity stop hurting on its own?
Temporary pain relief can occur if the inflamed pulp tissue becomes necrotic (dies), eliminating nerve signals. However, this does not mean the infection has resolved. Without professional treatment, bacteria continue to destroy the tooth structure and can spread to surrounding bone and tissue, leading to severe complications.
Conclusion
The question of do cavities hurt ultimately depends on the stage of disease progression and the anatomical layers involved. While early demineralization remains completely asymptomatic due to the nerve-free nature of tooth enamel, advancing decay triggers a cascade of inflammation, nerve compression, and bacterial infection that produces significant pain. From mild sensitivity during the initial dentin breach to severe, spontaneous toothaches once the pulp becomes compromised, cavity-related discomfort serves as a biological alarm signaling advanced tissue destruction. Waiting for pain to develop before seeking professional care is a reactive strategy that frequently leads to complex treatments, higher costs, and compromised tooth structure. By implementing consistent oral hygiene routines, optimizing dietary habits, utilizing fluoride and professional sealants, and attending routine dental examinations, individuals can effectively interrupt the caries process long before it becomes painful. Preventive dentistry remains the most reliable method to preserve natural teeth, maintain oral comfort, and ensure long-term systemic health. Prioritizing proactive care over pain-driven intervention is the definitive pathway to a resilient, pain-free smile.

About the author
Benjamin Carter, MD, is a board-certified otolaryngologist specializing in head and neck surgery, with an expertise in treating throat cancer. He is an associate professor and the residency program director at a medical school in North Carolina.