Can a Hernia Cause Constipation? The Complete Medical Guide
Understanding whether digestive discomfort stems from everyday lifestyle factors or an underlying anatomical issue is crucial for long-term wellness. Many individuals experience infrequent bowel movements and abdominal pressure without realizing the root cause may be structural rather than purely dietary. The medical community has extensively studied gastrointestinal motility and abdominal wall integrity, consistently revealing a significant intersection between these two systems (Mayo Clinic). When evaluating persistent bowel irregularities alongside noticeable abdominal bulges or groin discomfort, the question naturally arises: can a hernia cause constipation? The answer is definitively yes, and the physiological mechanisms behind this connection are both well-documented and clinically significant. This relationship operates in a bidirectional manner, meaning chronic straining during bowel movements can actually precipitate hernia formation, while an existing hernia can simultaneously restrict intestinal transit. Navigating this complex interplay requires a thorough understanding of abdominal anatomy, early symptom recognition, and evidence-based management strategies. By exploring how tissue protrusions impact digestive flow, examining the specific types of hernias most likely to trigger bowel complications, and reviewing both conservative and surgical interventions, you will gain the knowledge necessary to protect your gastrointestinal health and seek appropriate care when needed.
Understanding the Connection Between Hernias and Constipation
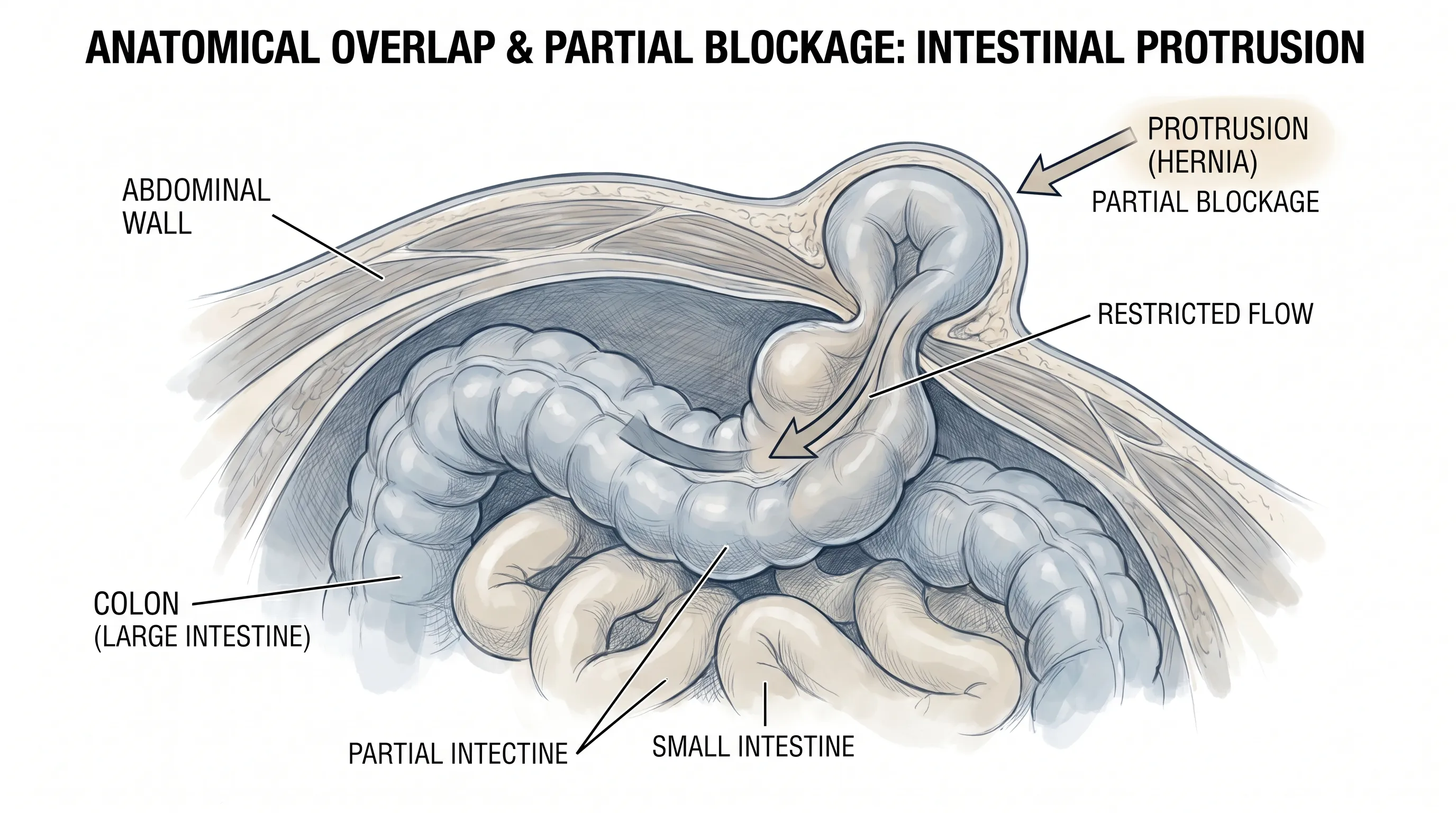
The human abdominal cavity is a highly pressurized environment that houses critical organs of the digestive, urinary, and reproductive systems. This pressure must be dynamically managed by the coordinated function of the diaphragm, pelvic floor, and layered abdominal musculature. When this structural integrity is compromised, the consequences often manifest in gastrointestinal dysfunction (NIH). Medical literature consistently demonstrates that can a hernia cause constipation depends largely on the anatomical position of the hernia, the volume of protruding tissue, and whether the bowel segment is partially compressed or fully entrapped. The most direct pathway involves mechanical interference. When a segment of the small or large intestine slips through a weakened fascial defect, it creates a physical narrowing within the gastrointestinal lumen. This narrowing slows the natural peristaltic waves that propel digested material toward the rectum, resulting in delayed transit time, increased water absorption by the colon, and ultimately, hardened stool.
Beyond simple mechanical restriction, neurovascular factors play a substantial role. Herniated bowel segments often experience subtle compression of the mesenteric blood supply and localized nerve endings. This microvascular compromise can dampen the intrinsic electrical pacing of the enteric nervous system, which governs coordinated muscle contractions in the digestive tract. When peristalsis becomes sluggish or uncoordinated, fecal matter accumulates, leading to bloating, discomfort, and reduced stool frequency. Furthermore, the psychological and behavioral adaptations patients develop in response to hernia-related pain frequently contribute to bowel irregularities. Individuals who experience sharp groin discomfort or abdominal pulling sensations may instinctively avoid straining during defecation to prevent pain exacerbation. This voluntary suppression of the Valsalva maneuver disrupts the natural defecation reflex, creating a secondary, functional layer of constipation that compounds the structural blockage.
The Anatomy of Abdominal Pressure
To comprehend how tissue displacement translates into digestive stagnation, one must examine the biomechanics of intra-abdominal pressure. Every time you cough, sneeze, lift a heavy object, or push during a bowel movement, pressure spikes within the abdominal cavity. In a healthy individual, the transversus abdominis, internal and external obliques, and rectus abdominis muscles contract synergistically to contain this force. However, congenital weaknesses, surgical scar tissue, chronic coughing, pregnancy, and age-related connective tissue degradation can create vulnerable zones, as recognized by the Cleveland Clinic. When intra-abdominal pressure repeatedly overwhelms these weak points, tissue herniation occurs. The resulting protrusion does not exist in isolation; it often drags adjacent bowel loops along with it. As the intestine bends or folds into the hernial sac, its diameter narrows. Even a partial reduction in luminal diameter can dramatically increase resistance to stool passage, following Poiseuille’s law, which states that flow resistance is inversely proportional to the fourth power of the radius. Consequently, even mild tissue entrapment can significantly slow colonic transit.
How Hernias Physically Impact Bowel Function
The physical impact of a hernia on bowel function extends beyond simple blockage. Entrapped intestinal segments frequently develop localized edema due to impaired venous drainage. Swelling further reduces the internal space available for stool movement, compounding the obstruction. Additionally, chronic mechanical irritation from the hernia sac can trigger inflammatory responses within the bowel wall, altering mucosal secretions and disrupting the optimal balance of digestive enzymes and bile acids. This inflammatory cascade can lead to dysmotility syndromes that mimic irritable bowel syndrome (IBS), making accurate diagnosis essential. Research from peer-reviewed journals, including studies published in Arquivos Brasileiros de Cirurgia Digestiva, highlights the statistically significant correlation between chronic constipation and inguinal hernia presence, reinforcing that the gastrointestinal tract and abdominal wall share a deeply interconnected physiological relationship (Mayo Clinic). When evaluating whether can a hernia cause constipation in your specific situation, clinical imaging and physical examination remain the gold standards for determining the extent of anatomical disruption.
Types of Hernias That Commonly Trigger Constipation
Not all abdominal wall defects carry the same risk profile for gastrointestinal complications. The anatomical location, size of the fascial defect, and likelihood of bowel involvement determine how severely digestive function will be impacted. Clinicians categorize hernias based on their precise anatomical origin, and certain types are notoriously more prone to causing bowel obstruction and chronic constipation, as detailed by the Cleveland Clinic. Understanding these distinctions is vital for recognizing symptom patterns and seeking timely intervention.
Inguinal Hernias and Digestive Disruption
Inguinal hernias represent the most prevalent form of abdominal wall defect, accounting for the vast majority of cases diagnosed in clinical practice. These hernias occur in the groin region, where the lower abdominal muscles naturally converge near the inguinal canal. Because this area experiences constant mechanical stress during walking, bending, and lifting, it is highly susceptible to weakening over time. When small bowel loops or segments of the sigmoid colon migrate into the inguinal canal, they can become temporarily or permanently lodged. This entrapment frequently manifests as constipation, accompanied by a noticeable bulge that may extend into the scrotum in males or the labia in females. The curved pathway of the inguinal canal creates an anatomical bottleneck, making it particularly difficult for bulky stool to navigate past the herniated segment. Clinical trials and epidemiological data consistently show that individuals with chronic constipation are at significantly elevated risk for inguinal hernia development, while those with existing inguinal defects frequently report worsened bowel habits.
Ventral and Umbilical Hernias
Ventral hernias arise anywhere along the anterior abdominal wall, often at sites of previous surgical incisions (incisional hernias) or natural midline weaknesses. Umbilical hernias specifically occur at the navel, where the fetal umbilical cord once connected to the placenta. Both types frequently involve loops of the small intestine or transverse colon. Because these hernias are positioned directly along the central digestive pathway, they can cause noticeable changes in stool caliber. Patients often report passing unusually thin or pencil-like stools, a classic sign of partial colonic obstruction. The proximity of ventral and umbilical defects to the peritoneal cavity also means that increased intra-abdominal pressure directly pushes bowel content against the fascial gap, creating a persistent feeling of incomplete evacuation. Over time, the repeated straining associated with this incomplete emptying exacerbates both the constipation and the hernia defect itself, establishing a self-perpetuating cycle that rarely resolves without medical intervention.
Femoral Hernias: The High-Risk Category
Although less common than inguinal variants, femoral hernias carry the highest risk for severe gastrointestinal complications. They develop just below the inguinal ligament, where the femoral vessels pass through the pelvic floor into the upper thigh. The femoral canal is naturally narrow and rigid, bordered by tough ligaments and bone. When bowel tissue enters this confined space, it is highly susceptible to incarceration. Medical literature indicates that up to thirty percent of femoral hernias become incarcerated, meaning the protruding tissue cannot be manually reduced. This high rate of entrapment makes femoral hernias particularly dangerous for digestive health. Constipation in these cases is rarely a mild, temporary symptom; instead, it often signals an impending complete bowel obstruction. Patients with femoral hernias frequently experience rapid-onset constipation accompanied by severe groin or upper thigh pain, requiring urgent surgical evaluation to prevent bowel ischemia and tissue necrosis.
| Hernia Type | Common Location | Bowel Segments Involved | Constipation Risk | Key Clinical Notes |
|---|---|---|---|---|
| Inguinal | Groin/Inguinal canal | Small intestine, sigmoid colon | High | Most prevalent type; often causes intermittent blockage and groin discomfort during straining |
| Ventral/Incisional | Midline or surgical scars | Small intestine, transverse colon | Moderate to High | Often associated with thin stools and persistent abdominal pressure |
| Umbilical | Navel region | Small intestine, colon | Moderate | Frequently exacerbated by obesity, pregnancy, or chronic coughing |
| Femoral | Below inguinal ligament | Small bowel, occasionally colon | Very High | Narrow canal leads to 30% incarceration rate; requires urgent evaluation |
The Bidirectional Relationship: A Vicious Cycle
The physiological interplay between hernias and bowel irregularities is not a one-way street. Clinical researchers have extensively documented how chronic constipation acts as both a consequence and a catalyst for abdominal wall compromise. This bidirectional relationship creates a self-reinforcing cycle that progressively worsens both conditions if left unmanaged. Straining during bowel movements generates intense, localized pressure within the abdominal cavity. According to the National Institutes of Health (NIH), repetitive straining places enormous mechanical stress on fascial layers and connective tissue, significantly increasing the likelihood of abdominal wall defects. Over months or years, this repetitive micro-trauma degrades collagen integrity, stretches muscle fibers, and enlarges natural anatomical openings. Eventually, the tissue fails to contain intra-abdominal contents, resulting in hernia formation. Once the hernia develops, it alters gastrointestinal motility, which in turn produces harder stools and further straining, accelerating the hernia’s growth and increasing the risk of complications.
Straining as a Catalyst for Hernia Development
Defecation requires coordinated relaxation of the pelvic floor and controlled increase in intra-abdominal pressure to expel stool. However, when stool is hard, dry, or impacted, individuals instinctively engage in prolonged Valsalva maneuvers to generate sufficient force. These maneuvers dramatically elevate central venous pressure and compress abdominal organs against the anterior wall. Studies registered on ClinicalTrials.gov, including trial NCT02749682, explicitly identify chronic constipation alongside heavy lifting and chronic coughing as primary facilitators of hernia formation (CDC). The sudden spikes in abdominal pressure overwhelm weakened connective tissue, particularly in individuals with inherent collagen disorders, aging fascia, or prior surgical scars. Preventing hernia development, therefore, heavily relies on maintaining bowel regularity through dietary fiber, hydration, and appropriate physical activity.
Clinical Evidence Linking the Two Conditions
Peer-reviewed research consistently validates the clinical observations linking digestive dysfunction and abdominal wall defects. A notable 2025 case-control study published in PMC (PMC12571447) demonstrated statistically significant associations between constipation severity and inguinal hernia presence across adult populations. Researchers utilized standardized constipation scoring systems alongside thorough clinical examinations, finding that patients with chronic constipation were disproportionately likely to present with occult or symptomatic hernias (Mayo Clinic). Another prospective case-control investigation evaluating nutritional status and constipation scores in inguinal hernia patients revealed that lower dietary fiber intake and higher constipation scores strongly correlated with larger hernia defects and longer symptom duration. These findings underscore that addressing bowel health is not merely symptomatic management but a fundamental component of hernia prevention and long-term abdominal wall preservation. When patients ask whether can a hernia cause constipation or if constipation causes a hernia, the evidence confirms that both scenarios occur simultaneously in clinical practice.
Recognizing Warning Signs and When to Seek Emergency Care
Distinguishing between manageable gastrointestinal discomfort and a potentially life-threatening abdominal emergency requires vigilant symptom monitoring. While mild constipation alongside a reducible hernia bulge may be managed conservatively under medical supervision, certain red flags demand immediate emergency intervention, as outlined by the Cleveland Clinic. A hernia with constipation can rapidly progress to a complete bowel obstruction or tissue strangulation, both of which carry severe morbidity and mortality risks if untreated. Early recognition of these warning signs can prevent irreversible bowel damage and sepsis.
Partial vs. Complete Bowel Obstruction
Partial bowel obstruction occurs when the herniated intestine is compressed but still permits limited passage of gas and stool. Symptoms include intermittent cramping, bloating, reduced stool frequency, and a sensation of incomplete evacuation. Patients may still pass gas or small, hard stools, and the hernia bulge might reduce spontaneously when lying flat. Complete bowel obstruction, however, represents total luminal blockage. Gas and stool cannot pass in either direction, leading to rapid abdominal distension, severe colicky pain, persistent nausea, and bilious vomiting. The inability to pass flatus is a hallmark clinical indicator that requires urgent imaging and surgical consultation.
Red Flags of a Strangulated Hernia
Strangulation occurs when the blood supply to the trapped intestinal segment is completely compromised. Without adequate perfusion, bowel tissue begins to die, releasing toxins into the peritoneal cavity and bloodstream. Warning signs include a hernia bulge that becomes intensely tender, firm, and discolored (red, purple, or dark). The pain shifts from intermittent cramping to constant, severe agony that worsens with light touch. Systemic symptoms emerge rapidly, including fever, tachycardia, hypotension, and altered mental status. Nausea and vomiting become persistent, and the abdomen may grow rigid due to peritoneal inflammation. Strangulated hernias are true surgical emergencies. Delayed intervention drastically increases the risk of bowel resection, sepsis, and multi-organ failure. If you experience these symptoms, do not wait for a scheduled appointment; seek emergency medical care immediately.
Medical Management and Treatment Options
Addressing constipation in the context of a hernia requires a tiered therapeutic approach that balances symptom relief with anatomical correction. Conservative management focuses on improving bowel motility and reducing intra-abdominal pressure, while surgical intervention aims to permanently restore abdominal wall integrity. The choice of treatment depends on hernia size, symptom severity, patient comorbidities, and the risk of obstruction (Mayo Clinic).
Non-Surgical Relief for Constipation
For patients with small, reducible hernias and mild-to-moderate constipation, non-surgical strategies often provide meaningful symptom improvement. Dietary fiber remains the first-line intervention, with soluble fibers like psyllium and oat bran increasing stool bulk and moisture, while insoluble fibers accelerate transit time through mechanical stimulation. Hydration is equally critical; fiber without adequate water intake can actually worsen constipation by creating dense, difficult-to-pass masses. Over-the-counter laxatives and stool softeners are frequently incorporated into management plans. Osmotic agents such as polyethylene glycol or magnesium hydroxide draw water into the colon, softening stool and stimulating peristalsis. Stimulant laxatives like bisacodyl or senna may be used short-term to trigger bowel contractions but should not be relied upon long-term due to potential colonic inertia. Prescription medications, including lubiprostone, linaclotide, plecanatide, and prucalopride, target specific intestinal receptors to enhance fluid secretion and colonic motility. These agents are particularly beneficial for patients with chronic idiopathic constipation coexisting with hernias. Additionally, pelvic floor physical therapy and biofeedback training can retrain defecation mechanics, reducing straining and lowering abdominal pressure.
Definitive Surgical Intervention
When conservative measures fail to relieve symptoms, or when hernias exhibit signs of incarceration or significant size progression, surgical repair becomes the definitive treatment. Modern hernia surgery focuses on tension-free reconstruction using synthetic or biologic mesh, which reinforces the weakened fascial layer and minimizes recurrence rates. Open surgical repair involves a direct incision over the defect, allowing precise anatomical dissection and secure mesh placement. Laparoscopic and robotic-assisted techniques offer minimally invasive alternatives, utilizing small incisions, high-definition magnification, and enhanced instrument articulation to reduce post-operative pain and accelerate recovery (Cleveland Clinic). During the procedure, the surgeon carefully reduces the herniated bowel, assesses tissue viability, and repositions any compromised segments before reinforcing the abdominal wall. Post-operative bowel management is critical, as anesthesia and pain medications temporarily slow gastrointestinal motility. Surgeons routinely prescribe stool softeners, recommend early ambulation, and encourage a gradual reintroduction of high-fiber foods to prevent post-surgical constipation. Most patients experience significant improvement in bowel regularity once the mechanical obstruction is resolved, though long-term dietary and lifestyle modifications remain essential for sustained digestive health.

Lifestyle Modifications and Preventive Strategies
Long-term management of hernia-related constipation extends far beyond clinical interventions. Sustainable lifestyle adjustments form the foundation of digestive wellness and abdominal wall preservation. Implementing evidence-based habits can dramatically reduce recurrence risk, minimize discomfort, and promote optimal gastrointestinal function. The integration of nutrition, physical activity, stress management, and ergonomic awareness creates a comprehensive defense against both constipation and hernia progression.
Dietary Adjustments for Bowel Regularity
Nutrition plays the most direct role in regulating bowel motility. A diet rich in whole grains, legumes, fruits, and vegetables provides the necessary fiber matrix to maintain soft, bulky stools, aligning with CDC nutritional guidelines. Soluble fiber from foods like apples, citrus fruits, carrots, and barley forms a gel-like substance in the colon, slowing digestion and promoting nutrient absorption while keeping stools hydrated. Insoluble fiber from wheat bran, nuts, seeds, and leafy greens adds structural bulk, stimulating intestinal muscles and accelerating transit. Patients should gradually increase fiber intake to twenty to thirty grams daily to prevent bloating and gas, which can temporarily increase intra-abdominal pressure. Adequate fluid consumption, typically two to three liters of water daily, ensures fiber functions optimally. Probiotic-rich foods like yogurt, kefir, sauerkraut, and kimchi support a healthy gut microbiome, which influences colonic motility and stool consistency. Limiting processed foods, excessive dairy, refined sugars, and high-fat meals reduces inflammation and prevents sluggish digestion.
Safe Physical Activity and Core Support
Exercise significantly influences both bowel function and abdominal wall strength. Low-impact aerobic activities such as walking, swimming, and stationary cycling stimulate peristalsis through rhythmic abdominal muscle engagement and enhanced blood flow. Strength training should focus on balanced core conditioning that strengthens the transversus abdominis and pelvic floor without generating dangerous intra-abdominal pressure spikes. Exercises like planks, diaphragmatic breathing drills, and controlled Pilates movements build deep muscular support that protects fascial layers. Patients with hernias should avoid heavy compound lifts, maximal Valsalva maneuvers, and high-impact activities until cleared by a surgeon. Proper lifting mechanics—bending at the knees, keeping objects close to the body, and exhaling during exertion—dramatically reduce abdominal stress. Stress management techniques, including meditation, yoga, and consistent sleep schedules, lower cortisol levels, which indirectly regulates gut motility and prevents tension-related digestive stagnation.
Frequently Asked Questions
Can a hernia cause constipation directly, or is it just a symptom of something else?
Yes, a hernia can cause constipation directly through mechanical interference. When intestinal tissue protrudes through a weakened abdominal wall, it creates a physical narrowing that slows stool transit. This structural restriction, combined with localized inflammation and altered nerve signaling, frequently results in infrequent bowel movements, hardened stool, and difficulty passing waste. Additionally, pain from the hernia often causes patients to avoid straining, which further delays evacuation (NIH).
What are the immediate signs that a hernia is causing a complete bowel obstruction?
A complete bowel obstruction presents with severe, cramping abdominal pain, absolute inability to pass gas or stool, persistent vomiting (often containing bile), rapid abdominal swelling, and a rigid, tender abdomen. The hernia bulge may become firm, intensely painful, and discolored. These symptoms indicate total luminal blockage and require immediate emergency medical evaluation to prevent bowel ischemia and life-threatening complications (Mayo Clinic).
Can constipation alone lead to the development of a hernia?
Absolutely. Chronic constipation forces prolonged straining during bowel movements, which dramatically elevates intra-abdominal pressure. Repeated pressure spikes place mechanical stress on the abdominal wall, gradually stretching and weakening connective tissue and muscle fibers. Over time, this degradation can create fascial defects that allow abdominal contents to protrude, directly causing hernia formation (Cleveland Clinic). Managing bowel regularity is a proven preventive strategy.
Is surgical hernia repair required to resolve constipation caused by a hernia?
While dietary modifications, laxatives, and stool softeners can provide temporary symptomatic relief, they do not correct the underlying anatomical defect. If constipation is directly caused by mechanical bowel compression from a hernia, surgical repair is typically necessary to permanently eliminate the obstruction. Once the intestine is repositioned and the abdominal wall reinforced, normal digestive transit usually resumes (NIH).
How long does constipation last after hernia surgery?
Post-operative constipation is common and typically lasts three to seven days. It is primarily caused by anesthesia, opioid pain medications, reduced physical activity, and dietary changes during recovery. Surgeons recommend proactive bowel management, including stool softeners, osmotic laxatives, hydration, and gentle walking. Most patients return to normal bowel habits within the first two weeks after surgery (Mayo Clinic).
Conclusion
Navigating the intersection of abdominal wall integrity and digestive function requires a nuanced understanding of how structural defects impact gastrointestinal motility. The evidence clearly demonstrates that can a hernia cause constipation is answered with a definitive yes, as protruding intestinal tissue frequently creates mechanical blockages, alters nerve signaling, and triggers behavioral changes that collectively slow bowel transit. This relationship operates bidirectionally, with chronic straining serving as both a consequence of hernia-related discomfort and a primary catalyst for tissue weakening. Recognizing early warning signs, distinguishing between manageable symptoms and emergency complications, and pursuing appropriate medical evaluation are essential steps in preventing severe outcomes like bowel obstruction or strangulation. Whether through conservative dietary adjustments, targeted medication regimens, or definitive surgical repair, effective management prioritizes restoring normal abdominal pressure dynamics and optimizing colonic transit. By integrating clinical insights, peer-reviewed research, and practical lifestyle modifications, individuals can take proactive control of their digestive health. If you experience persistent bowel irregularities alongside noticeable abdominal or groin bulges, consult a qualified healthcare provider to develop a personalized, evidence-based treatment plan. Prioritizing bowel regularity, practicing safe lifting mechanics, and maintaining core strength will not only alleviate current symptoms but also safeguard your abdominal wall against future complications.

About the author
Fatima Al-Jamil, MD, MPH, is board-certified in gastroenterology and hepatology. She is an Assistant Professor of Medicine at a university in Michigan, with a clinical focus on inflammatory bowel disease (IBD) and motility disorders.