What Type of Lens Does Medicare Cover for Cataract Surgery?

Key points
- Blurry or foggy vision that may resemble looking through a dirty window
- Faded or yellowed colors, making it difficult to distinguish between shades like navy and black
- Increased glare and halos around lights, especially at night or when driving in rain
- Difficulty seeing in low light or adapting quickly to changes in lighting conditions
- Frequent changes in your glasses prescription that no longer provide satisfactory clarity
- Double vision in one eye or needing brighter light to read and perform close-up tasks
Cataracts are a common, age-related eye condition that can cloud your vision and interfere with daily life. For the millions of Americans on Medicare who need cataract surgery, a key question arises: "What type of lens does Medicare cover for cataract surgery?"
Cataract surgery involves replacing the eye's cloudy natural lens with a clear, artificial intraocular lens (IOL). With several types of IOLs available—each offering different visual benefits—understanding Medicare’s coverage is crucial for making informed health and financial decisions. This guide breaks down what you need to know about the lenses Medicare covers, including clinical considerations, insurance logistics, and long-term visual outcomes. According to the National Eye Institute (NIH), cataracts are a leading cause of vision loss worldwide, yet cataract surgery remains one of the safest and most frequently performed procedures in modern ophthalmology.
What Is a Cataract?
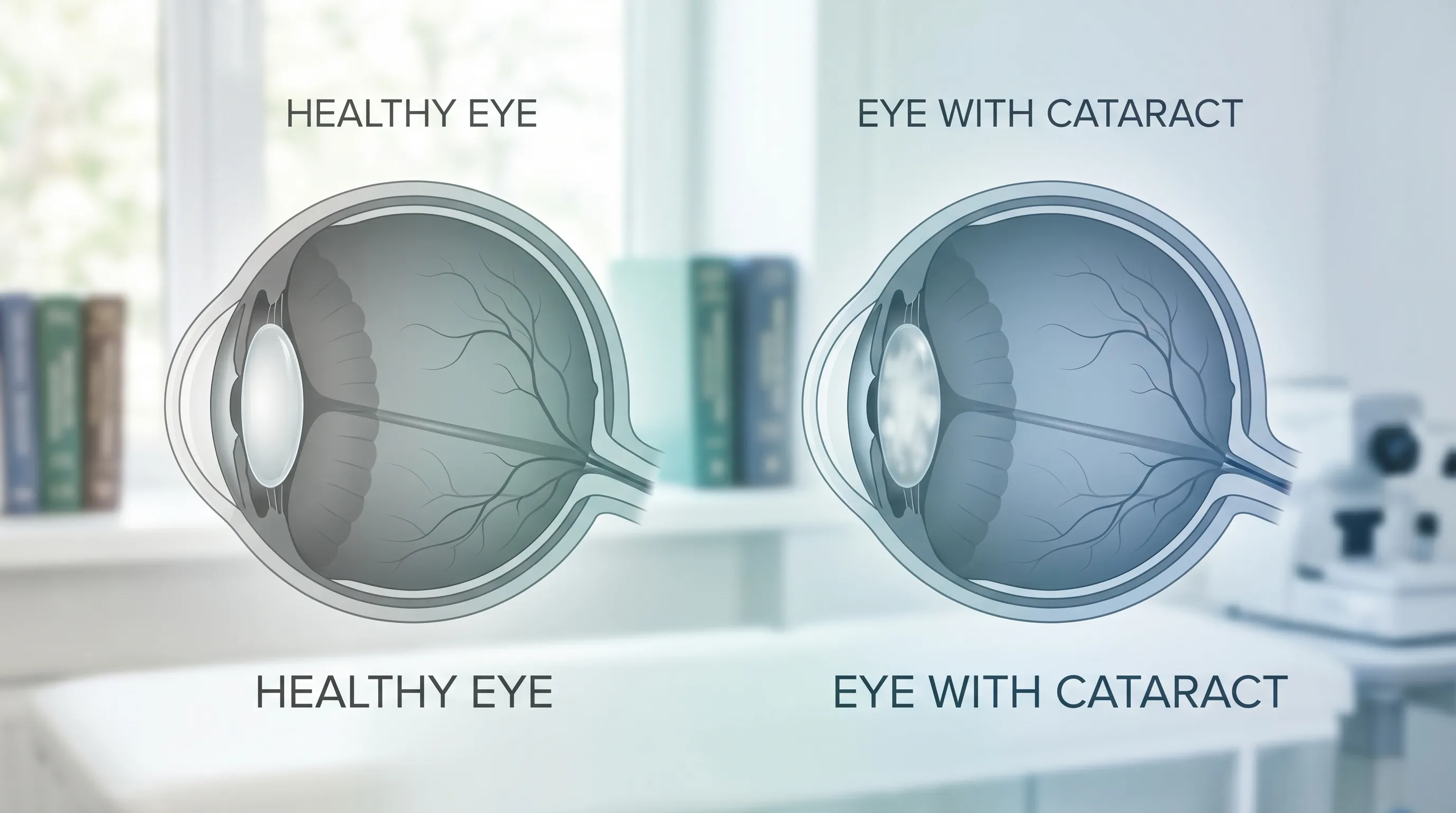
A cataract is a clouding of the eye’s natural lens, which lies behind the iris and pupil. This lens works much like a camera lens, focusing light onto the retina to produce clear, sharp images. As a cataract develops, the lens proteins clump together, becoming opaque and scattering light before it can properly reach the retina. This process typically occurs gradually over months or years, though certain medical conditions can accelerate lens deterioration. The progression of cataracts leads to symptoms such as:
- Blurry or foggy vision that may resemble looking through a dirty window
- Faded or yellowed colors, making it difficult to distinguish between shades like navy and black
- Increased glare and halos around lights, especially at night or when driving in rain
- Difficulty seeing in low light or adapting quickly to changes in lighting conditions
- Frequent changes in your glasses prescription that no longer provide satisfactory clarity
- Double vision in one eye or needing brighter light to read and perform close-up tasks
Cataract development is influenced by multiple risk factors, including prolonged ultraviolet (UV) light exposure, smoking, diabetes mellitus, prolonged corticosteroid use, previous ocular trauma, obesity, hypertension, and genetic predisposition. The CDC emphasizes that managing systemic health conditions, wearing UV-protective sunglasses, and maintaining a nutrient-rich diet with antioxidants can support overall ocular health, though they cannot reverse existing lens clouding.
When these symptoms significantly impair your ability to perform daily activities like reading, recognizing faces, working on a computer, or driving, your ophthalmologist will likely recommend cataract surgery. Surgery is considered medically necessary when visual impairment impacts functional independence or quality of life. The decision to proceed is highly individualized, as some cataracts mature slowly enough that patients can delay surgery safely for months or years under regular monitoring.
How Does Cataract Surgery Work?
Cataract surgery is a safe, highly effective, and common outpatient procedure performed by board-certified ophthalmologists. During the surgery, the surgeon makes a micro-incision (typically 2–3 millimeters) in the cornea. Through this opening, an ultrasonic handpiece is inserted to break up the cloudy natural lens using a technique called phacoemulsification. The liquefied lens fragments are gently suctioned out, leaving the clear posterior capsule intact to serve as a natural support structure for the replacement lens.
Next, the surgeon inserts a new, artificial intraocular lens (IOL) through the same micro-incision. The IOL unfolds and positions itself securely inside the empty lens capsule. Modern IOLs are foldable, allowing them to be delivered through tiny incisions that heal rapidly and typically do not require sutures. The entire procedure usually takes less than 30 minutes per eye. Most patients are awake during surgery but receive topical anesthetic drops and mild intravenous sedation to ensure complete comfort. Vision improvement is often noticeable within 24 to 48 hours, though full visual stabilization can take several weeks as the cornea heals and the brain adapts to the new optical system.
Advancements in surgical technology have also introduced femtosecond laser-assisted cataract surgery, which uses a computer-guided laser to perform precise corneal incisions, soften the cataract, and create an optimal opening in the capsule before the surgeon completes the procedure. While laser-assisted techniques offer enhanced precision in specific anatomical cases, clinical studies indicate that both traditional phacoemulsification and laser-assisted approaches yield excellent visual outcomes when performed by experienced surgeons. The choice between techniques depends on ocular anatomy, corneal health, surgeon expertise, and patient preference.
Types of Intraocular Lenses (IOLs)
The type of IOL you choose determines how you will see after surgery, your dependence on corrective eyewear, and your out-of-pocket financial responsibility. Modern IOLs are manufactured from biocompatible materials such as hydrophobic acrylic, hydrophilic acrylic, or medical-grade silicone. They are designed to remain in the eye permanently without degradation. The main categories are standard monofocal lenses and premium lenses.
Standard Monofocal IOL
A monofocal IOL is the most basic type of lens. It has a single focal point and provides clear vision at one distance—usually far away.
- Function: Corrects vision for one distance (e.g., driving, watching TV). Patients typically choose distance vision for the dominant eye to maintain spatial awareness and safety.
- Post-Surgery Needs: You will likely need glasses for near-vision tasks like reading or for intermediate vision like using a computer. Some patients opt for "monovision," where one eye is targeted for distance and the other for near vision, though this requires neural adaptation and may reduce depth perception.
- Medicare Coverage: A standard monofocal IOL is fully covered by Medicare as part of medically necessary cataract surgery. After your Part B deductible, Medicare pays 80% of the approved amount, and you (or your supplemental insurance) pay the remaining 20%. This coverage policy is defined by the Centers for Medicare & Medicaid Services (CMS) and applies to all Original Medicare beneficiaries nationwide.
Premium IOLs
Premium IOLs offer advanced features that can reduce or eliminate the need for glasses after surgery. These are considered elective upgrades and are not fully covered by Medicare. They utilize sophisticated optical designs, diffractive rings, or specialized toric corrections to address refractive errors beyond simple cataract removal.
Toric IOL (For Astigmatism)
A toric IOL is designed to correct astigmatism, a common condition caused by an irregularly shaped cornea that results in blurry or distorted vision at all distances. Astigmatism occurs when the cornea resembles a football rather than a basketball, causing light to focus on multiple points on the retina.
- Function: Corrects both cataracts and astigmatism. The lens is precisely aligned during surgery using intraoperative marking or digital guidance systems to neutralize corneal irregularities.
- Medicare Coverage: Medicare does not cover the astigmatism-correcting feature. Medicare will pay the amount for a standard monofocal lens, but you must pay the additional cost for the toric lens out-of-pocket. Prices typically range from $1,000 to $2,000 per eye depending on the lens brand, surgical facility, and geographic region.
Multifocal and Extended Depth-of-Focus (EDOF) IOLs
These lenses have multiple focal points or an extended range of focus to provide clear vision at various distances—near, intermediate, and far. This can significantly reduce your dependence on glasses for everyday activities.
- Function: Corrects vision for multiple distances, addressing presbyopia (age-related reading vision loss). Multifocal lenses use concentric rings to split light, while EDOF lenses stretch a single focal point into a continuous range.
- Drawbacks: Some patients may experience glare, halos, starbursts, or reduced contrast sensitivity, especially in low-light conditions. The visual phenomena usually diminish over 3–6 months as the brain learns to filter out overlapping images, a process known as neuroadaptation. These lenses may not be ideal for patients who require exceptional night vision, such as commercial pilots or frequent night drivers.
- Medicare Coverage: Medicare does not cover the presbyopia-correcting features. Similar to toric lenses, Medicare pays its standard amount for a basic monofocal lens, and you pay the additional cost for the multifocal or EDOF lens. Out-of-pocket expenses generally range from $1,500 to $3,500 per eye.
Accommodating IOLs
Accommodating IOLs are designed to work with your eye's natural ciliary muscles, allowing the lens to shift focus between distant and near objects through mechanical movement or optical design.
- Function: Provides a range of vision by flexing or moving forward slightly within the eye during accommodation, mimicking the natural focusing mechanism of a younger eye.
- Drawbacks: The accommodative range may decrease over time due to capsular fibrosis or reduced ciliary muscle elasticity in older patients. Visual outcomes can be less predictable than with premium diffractive lenses.
- Medicare Coverage: These are also considered premium, presbyopia-correcting lenses. Medicare covers the base cost of the surgery and a standard lens, while you pay the extra amount for the accommodating feature. Costs typically align with other premium IOL categories.
How Medicare Covers Cataract Surgery
Medicare coverage for cataract surgery falls primarily under Part B (Medical Insurance), as it is classified as an outpatient, medically necessary procedure. Understanding the exact financial breakdown and policy guidelines is essential for avoiding unexpected bills. The Mayo Clinic and CMS publish comprehensive guidelines that outline beneficiary responsibilities, allowable charges, and coverage determinations for ocular procedures.
What Medicare Part B Covers:
- Pre-surgery exams to diagnose the cataract, assess corneal topography, measure axial length, and calculate IOL power using advanced biometry.
- The surgeon's and facility fees for the procedure, including operating room time, surgical supplies, and anesthesia services.
- The cost of a standard monofocal intraocular lens implanted in each eye.
- One pair of eyeglasses with standard frames or one set of contact lenses after the surgery. This is the only instance Medicare covers routine vision correction outside of medically necessary conditions.
- Follow-up care related to the surgery, including post-operative visits to monitor healing, check intraocular pressure, and verify visual acuity.
Your Costs with Original Medicare:
- Part B Deductible: You must first meet your annual Part B deductible (which resets each calendar year). Once met, your coverage activates for the remainder of the year.
- 20% Coinsurance: After the deductible is met, you are responsible for 20% of the Medicare-approved amount for the surgery, anesthesia, facility fees, and the standard lens. A Medigap (Medicare Supplement) plan can help cover this coinsurance, with popular plans like Plan G covering the 20% entirely after the deductible is satisfied.
- Assignment Acceptance: Ensure your ophthalmologist accepts Medicare assignment. If they do not, you may face additional balance billing charges that Medicare will not cover. Always verify provider participation status through the official Medicare Physician Compare tool.
Coverage with Medicare Advantage (Part C)
Medicare Advantage plans must cover everything Original Medicare does, including cataract surgery with a standard monofocal lens, as mandated by federal law. However, your out-of-pocket costs may differ significantly based on plan design. Instead of a fixed 20% coinsurance, you might have a flat copayment for the procedure or facility. Many Advantage plans impose network restrictions, requiring you to select surgeons and surgical centers within their contracted provider network. You may also need prior authorization before the surgery date. Check with your specific plan for details on costs, referral requirements, and supplemental vision benefits that sometimes offer additional allowances for post-surgical eyewear or frame upgrades.
Post-Surgery Benefits and Considerations
- Corrective Eyewear: Medicare's coverage for one pair of glasses or contacts post-surgery is a significant benefit, but it comes with strict parameters. You must visit a Medicare-enrolled optical supplier, and your prescription cannot be finalized until approximately 30 days post-surgery to ensure your eyes have stabilized. This applies only after an IOL has been implanted. If you choose upgraded frames or specialized lenses (like progressive, polycarbonate, photochromic, or anti-glare), you will have to pay the extra cost. Keep in mind that this eyewear benefit is a one-time allowance per eye surgery event.
- Prescription Eye Drops: Your doctor will prescribe a regimen of antibiotic and anti-inflammatory eye drops to prevent infection, control inflammation, and promote corneal healing. These medications are covered under Medicare Part D (Prescription Drug Coverage) rather than Part B. Check your Part D plan's formulary to see how your prescribed medications are tiered and what your copays will be. Generic alternatives like prednisolone acetate or moxifloxacin are often available at significantly lower costs and provide equivalent clinical efficacy.
- YAG Laser Capsulotomy: Months or years after surgery, the thin membrane (capsule) holding the IOL can become cloudy, a condition known as posterior capsular opacification or "secondary cataract." This condition affects roughly 20–30% of patients and is easily treated with a simple, painless laser procedure called a YAG laser capsulotomy. The procedure takes about five minutes, requires no incisions, and is fully covered by Medicare as a medically necessary follow-up treatment.
Preparing for Surgery and Navigating Recovery
A successful cataract surgery outcome depends heavily on proper preparation and diligent post-operative care. Before your procedure, compile a comprehensive medication list, including prescription drugs, over-the-counter supplements, and herbal products. Certain medications like alpha-blockers (e.g., tamsulosin) can cause intraoperative floppy iris syndrome, so your surgeon must be aware of their use. Blood thinners may need temporary adjustment, but this should only be done under direct guidance from your prescribing physician.
On the day of surgery, wear comfortable, loose-fitting clothing, avoid wearing makeup or perfumes, and arrange for a responsible adult to drive you home. You cannot drive immediately after the procedure due to pupil dilation, sedation effects, and initial visual blurriness. Prepare your home by clearing tripping hazards, placing medications in an accessible location, and stocking easy-to-prepare meals for the first 48 hours.
Post-operative care is critical for preventing complications. Use all prescribed eye drops exactly as scheduled; do not skip doses even if your eye feels comfortable. Avoid rubbing or pressing on the operated eye, as this can disrupt healing or displace the IOL. Wear the protective eye shield provided by your surgical center while sleeping for at least the first week. Refrain from swimming, using hot tubs, or exposing your eyes to soap or tap water for two to three weeks to prevent infection. Heavy lifting, straining, and high-impact exercise should be avoided for approximately one week to minimize intraocular pressure spikes. Most patients can return to desk work within a few days, but driving clearance depends on your visual acuity and your surgeon's evaluation.
Recognize warning signs that require immediate medical attention: sudden vision loss, severe pain unrelieved by prescribed medication, increasing redness, excessive tearing, or new flashes and floaters. These symptoms could indicate infection, retinal detachment, or elevated intraocular pressure, all of which demand urgent ophthalmic intervention.
Making Your Decision
Choosing the right IOL is a personal decision that depends on your lifestyle, vision goals, ocular anatomy, and budget. While the financial aspect is important, clinical suitability should drive your selection. Patients with advanced macular degeneration, glaucoma, or significant dry eye disease may not achieve optimal results with multifocal or EDOF lenses due to pre-existing retinal or tear film limitations. In these cases, a standard monofocal lens combined with well-fitted glasses often provides the most reliable and comfortable visual outcome.
- Talk to Your Ophthalmologist: Discuss your daily activities (e.g., driving, reading, computer use, hobbies) to determine which lens is best suited for you. Ask about corneal astigmatism, ocular surface health, and whether you are a candidate for neuroadaptation.
- Understand the Costs: Before surgery, ask your surgeon's office for a detailed cost breakdown. They should provide an Advance Beneficiary Notice (ABN) if you choose a premium lens, outlining what Medicare will cover and the exact amount you will owe out-of-pocket. Review this document carefully before signing.
- Weigh the Pros and Cons: While a standard monofocal lens is an excellent, fully covered option for restoring clear vision, a premium lens may be a worthwhile investment if your goal is to be less dependent on glasses and you understand the potential for optical side effects. Consider financing options offered by surgical centers if paying upfront is challenging.
- Verify Insurance and Network Status: Contact Medicare or your Advantage plan directly to confirm surgeon participation, facility fees, and lens upgrade policies. Request a written estimate of your expected financial responsibility to avoid surprise billing.
By understanding your options, preparing thoroughly, and reviewing Medicare's coverage rules, you can confidently move forward with cataract surgery and enjoy the benefits of clear vision for years to come.
Frequently Asked Questions
Does Medicare cover cataract surgery in both eyes?
Yes. Medicare covers cataract surgery for both eyes if both are medically necessary. However, the procedures are typically scheduled several weeks apart. Medicare allows you to receive a new pair of glasses or contacts after each surgery, but coverage applies separately to each eye's post-operative prescription once vision has stabilized.
Can I get a refund if I upgrade my lens and am unhappy with the result?
Premium IOL upgrades are considered elective services and are generally non-refundable. The out-of-pocket fee covers the lens itself, surgical planning, and enhanced intraoperative alignment. If you experience optical side effects like glare or halos, your surgeon may recommend a waiting period of three to six months for neuroadaptation. In rare cases of severe visual dissatisfaction, lens exchange may be considered, but it carries additional surgical risks and costs that are typically not covered by Medicare.
What happens if I have a Medicare Advantage plan and my surgeon is out of network?
Medicare Advantage plans operate under HMO, PPO, or POS models. If your plan is an HMO, out-of-network cataract surgery is generally not covered except in true emergencies. PPO plans may allow out-of-network care but at significantly higher copayments or coinsurance rates. Always verify network status before scheduling and request a referral or prior authorization if required. Your plan must cover the procedure at in-network cost-sharing levels if prior authorization was approved but an in-network facility was unavailable.
Are laser-assisted cataract surgeries covered differently than traditional surgery?
Laser-assisted cataract surgery (using a femtosecond laser) is classified by CMS as an adjunctive service. Medicare covers the core cataract removal and standard IOL implantation identically to traditional phacoemulsification. However, the additional laser fee for creating precise corneal incisions and softening the cataract is considered a patient-responsible upgrade. Costs for the laser component typically range from $500 to $1,500 per eye and must be paid out-of-pocket unless you have supplemental coverage that explicitly includes laser enhancements.
How do I know if I truly need a cataract removal?
Medical necessity is determined by functional impairment rather than cataract density alone. If your visual acuity has declined to 20/40 or worse, if glare impairs night driving, or if the cataract prevents proper examination of the retina for conditions like diabetic retinopathy or macular degeneration, surgery is indicated. Your ophthalmologist will perform standardized testing, including glare assessment and contrast sensitivity measurement, to document medical necessity for Medicare coverage purposes.
Conclusion
Cataract surgery remains one of the most transformative medical interventions available today, offering rapid pain relief, restored clarity, and significantly improved quality of life. Medicare comprehensively covers the core components of the procedure, including the surgeon’s fees, facility costs, anesthesia, and a standard monofocal intraocular lens. Beneficiaries must meet their Part B deductible and pay 20% coinsurance unless covered by a Medigap policy, while those enrolled in Medicare Advantage should verify network restrictions, copayment structures, and prior authorization rules. Premium IOLs—such as toric, multifocal, EDOF, and accommodating lenses—provide advanced visual customization but require substantial out-of-pocket investment since Medicare only covers the baseline monofocal equivalent.
Successfully navigating your cataract surgery journey requires thorough preparation, clear communication with your ophthalmologist, and a realistic understanding of both clinical outcomes and financial responsibilities. By reviewing your prescription eye drop coverage under Part D, utilizing your post-surgical eyewear benefit, and adhering strictly to recovery protocols, you can maximize your surgical results. Whether you choose the cost-effective standard monofocal option or invest in a premium lens for greater spectacle independence, staying informed about Medicare coverage guidelines ensures you can proceed with confidence, secure in the knowledge that medically necessary vision restoration remains fully supported by your healthcare benefits.

About the author
Benjamin Carter, MD, is a board-certified otolaryngologist specializing in head and neck surgery, with an expertise in treating throat cancer. He is an associate professor and the residency program director at a medical school in North Carolina.