Understanding COPD Pink Puffer Blue Bloater: History, Symptoms, and Modern Care

When navigating the complex landscape of chronic obstructive pulmonary disease (COPD), you may encounter historical clinical descriptors like the copd pink puffer blue bloater terminology. These phrases originated in the mid-twentieth century as a shorthand method for clinicians to rapidly categorize patients based on visible physical traits and breathing patterns. While modern respiratory medicine has largely retired these labels in favor of more precise, evidence-based classifications, understanding the underlying physiological differences they represent remains highly valuable for patients, caregivers, and healthcare students. This comprehensive guide explores the pathophysiology, clinical manifestations, diagnostic approaches, and modern management strategies associated with these classic phenotypes, providing actionable insights to help you navigate respiratory wellness with confidence and clarity.
The Historical Origins of COPD Clinical Classification
During the 1950s and 1960s, before the widespread availability of high-resolution computed tomography scanning and standardized pulmonary function testing, clinicians relied heavily on bedside observation to diagnose and categorize chronic lung diseases. The copd pink puffer blue bloater descriptors emerged from clinical teaching hospitals where physicians noticed two distinct patterns among patients presenting with chronic airflow obstruction. The classification system was built on visible characteristics: skin color, body weight distribution, breathing effort, sputum production, and secondary cardiovascular complications.
At that time, respiratory physiology was still being mapped, and the relationship between chronic tobacco exposure and progressive lung destruction was only beginning to gain formal recognition in medical literature. The phenotypic classification provided a practical framework for predicting disease progression, anticipating complications like right heart failure, and tailoring initial therapeutic interventions. It also helped medical students quickly recognize life-threatening respiratory decompensation in emergency settings.
However, as diagnostic technology advanced and longitudinal cohort studies revealed the true heterogeneity of obstructive lung disease, the rigid binary model began to show significant limitations. Researchers discovered that the vast majority of patients exhibited overlapping pathological processes rather than pure presentations. Despite these scientific advancements, the copd pink puffer blue bloater framework persists in medical education and patient advocacy circles as a foundational teaching tool for understanding the divergent pathways of emphysema-predominant and chronic bronchitis-predominant disease processes.
Understanding the Emphysema-Predominant Presentation
Pathophysiology and Structural Lung Changes
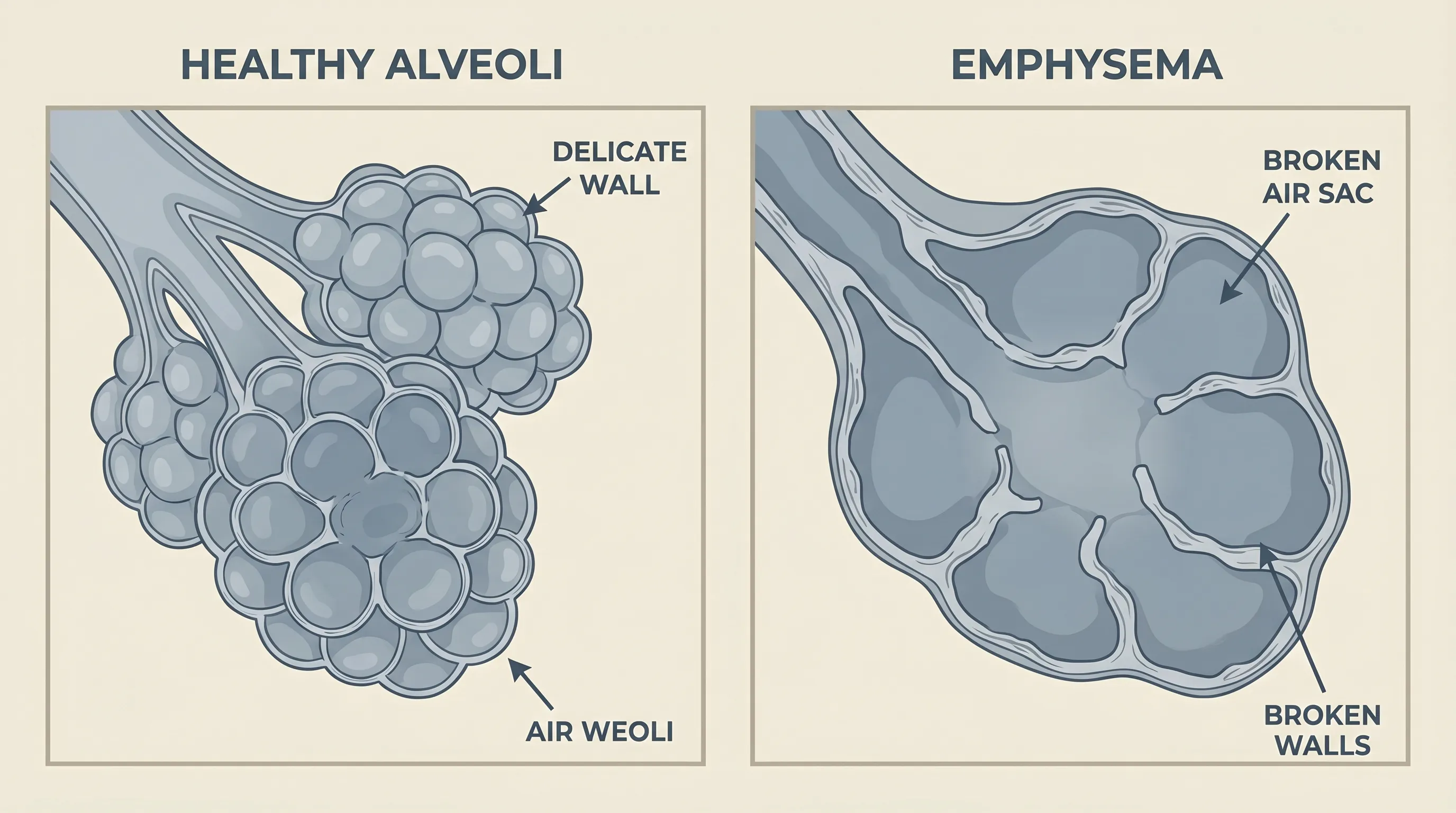
The pink puffer phenotype corresponds clinically to severe emphysema, a condition defined by irreversible destruction of alveolar walls and loss of pulmonary elastic recoil. The primary driver of this process is typically prolonged exposure to cigarette smoke, though alpha-1 antitrypsin deficiency can cause early-onset disease in non-smokers. Inhaled toxins trigger chronic neutrophilic and macrophage inflammation, leading to the release of proteolytic enzymes that degrade elastin and collagen in the alveolar septa.
As the microscopic air sacs merge into larger, irregularly shaped bullae, the surface area available for gas exchange dramatically decreases. Concurrently, the loss of elastic recoil prevents small airways from remaining open during exhalation, resulting in premature airway collapse and air trapping. This hyperinflation increases the resting lung volume, flattens the diaphragm, and expands the rib cage into the characteristic barrel chest configuration. The increased work of breathing forces patients to recruit accessory muscles, including the sternocleidomastoid, scalene, and intercostal groups, which becomes visible during clinical examination.
Clinical Presentation and Symptom Recognition
Patients with this emphysema-dominant presentation typically exhibit profound dyspnea that disproportionately exceeds radiographic findings. Unlike chronic bronchitis, sputum production is minimal, and coughing episodes are infrequent. The term pink reflects the fact that these individuals maintain relatively normal arterial oxygen saturation levels, often appearing ruddy or pink despite severe respiratory compromise. This preservation of oxygenation is achieved through compensatory tachypnea and increased minute ventilation, which effectively washes out carbon dioxide but requires massive caloric expenditure.
Weight loss and muscle wasting are prominent features, stemming from both the elevated metabolic cost of breathing and systemic inflammatory cytokines that promote catabolism. Many patients adopt adaptive strategies, such as leaning forward with arms braced on knees or furniture, to optimize diaphragmatic positioning and reduce the mechanical disadvantage of hyperinflated lungs. Pursed-lip breathing becomes an involuntary or consciously learned technique to maintain positive airway pressure during exhalation, preventing premature bronchiolar collapse and improving ventilation efficiency.
Diagnostic Markers and Pulmonary Function Assessment
Pulmonary function testing reveals a markedly reduced FEV1/FVC ratio confirming airflow obstruction, alongside significantly decreased diffusing capacity for carbon monoxide (DLCO), reflecting the loss of alveolar-capillary membrane surface area. High-resolution chest CT scans demonstrate low lung attenuation, prominent bullae, and reduced vascular markings. Arterial blood gas analysis typically shows compensated respiratory alkalosis with low or normal PaCO2 and near-normal PaO2, differentiating this profile from the hypoxic-hypercapnic state seen in chronic bronchitis.
Decoding the Chronic Bronchitis-Dominant Presentation
Airway Inflammation and Mucus Hypersecretion
The blue bloater phenotype represents severe chronic bronchitis, defined clinically by a productive cough lasting at least three months per year for two consecutive years, without other identifiable causes. The pathophysiological hallmark is chronic airway inflammation triggered by repeated irritant exposure, predominantly tobacco smoke. In response to persistent injury, bronchial submucosal glands undergo hypertrophy, and goblet cell hyperplasia dramatically increases mucus production.
Thick, tenacious secretions accumulate in narrowed airways, creating mechanical obstruction and fostering bacterial colonization. Chronic inflammation also leads to smooth muscle hypertrophy, airway edema, and fibrotic remodeling, further restricting airflow. Unlike emphysema, where structural destruction dominates, chronic bronchitis is primarily an obstructive disease of the conducting airways. Gas exchange impairment occurs secondary to ventilation-perfusion mismatching, as mucus-plugged airways prevent oxygen from reaching functioning alveoli, while perfusion continues to those regions.
Clinical Presentation and Complication Development
Cyanosis gives rise to the blue descriptor, reflecting chronic hypoxemia and reduced hemoglobin oxygen saturation. Peripheral hypoxia stimulates compensatory polycythemia, which increases blood viscosity and further impairs microcirculation. The term bloater describes the frequent presence of fluid retention, weight gain, and peripheral edema, which signal the development of cor pulmonale. Chronic alveolar hypoxia triggers hypoxic pulmonary vasoconstriction, elevating pulmonary artery pressures over years or decades.
The right ventricle compensates initially through concentric hypertrophy, but sustained pressure overload eventually leads to dilation and systolic dysfunction. Clinical signs include distended jugular veins, hepatomegaly, hepatojugular reflux, and pitting edema in the lower extremities. Patients often report fatigue, morning headaches (from nocturnal hypercapnia), and recurrent lower respiratory infections. Shortness of breath may be less pronounced at rest compared to the emphysema phenotype, but exercise tolerance is severely limited by both airflow obstruction and cardiovascular strain.
Diagnostic Markers and Gas Exchange Evaluation
Pulmonary function testing confirms obstructive physiology with reduced FEV1/FVC, but DLCO is typically preserved or only mildly reduced, since alveolar architecture remains relatively intact. Chest radiographs often show increased bronchovascular markings, peribronchial cuffing, and enlarged pulmonary artery segments. Arterial blood gas analysis reveals chronic hypoxemia with secondary hypercapnia, compensated by renal bicarbonate retention, resulting in a near-normal or slightly elevated pH. Polycythemia is evident on complete blood count, and echocardiography typically demonstrates right ventricular enlargement with elevated pulmonary artery systolic pressure.
Pink Puffer vs. Blue Bloater: A Comprehensive Comparison
Understanding the divergent clinical trajectories of these phenotypes clarifies why treatment protocols historically differed, even though modern medicine recognizes a broad disease spectrum. The copd pink puffer blue bloater framework highlights how identical primary etiologies can manifest through fundamentally different physiological pathways.
| Feature | Emphysema-Dominant Presentation | Chronic Bronchitis-Dominant Presentation |
|---|---|---|
| Primary Pathology | Alveolar wall destruction, loss of elastic recoil | Airway inflammation, mucus gland hyperplasia, bronchial narrowing |
| Body Habit | Cachectic, low BMI, muscle wasting | Overweight, fluid retention, peripheral edema |
| Skin Color | Pink, well-perfused, normal oxygenation maintained via hyperventilation | Cyanotic, bluish lips and nail beds due to chronic hypoxemia |
| Cough and Sputum | Minimal, non-productive, dry cough | Chronic, productive, thick mucopurulent sputum |
| Breathing Effort | Marked tachypnea, pursed-lip breathing, accessory muscle use | Moderate tachypnea, often less obvious respiratory distress at rest |
| Arterial Blood Gases | Normal PaO2, low or normal PaCO2, compensated alkalosis | Low PaO2, elevated PaCO2, compensated acidosis |
| Cardiovascular Impact | Pulmonary hypertension develops late, cor pulmonale uncommon early | Early cor pulmonale, right ventricular failure, edema common |
| Radiographic Findings | Hyperinflation, flat diaphragms, bullae, decreased vascular markings | Prominent bronchovascular markings, enlarged pulmonary arteries |
| Diffusing Capacity (DLCO) | Markedly reduced | Normal or mildly reduced |
This comparison underscores the physiological divergence that originally justified separate clinical categories. However, clinical reality frequently demonstrates mixed features, with most patients exhibiting both emphysematous destruction and bronchitic inflammation to varying degrees.

Why Medical Professionals Have Phased Out These Labels
The Problem with Stereotyping and Diagnostic Inaccuracy
The gradual abandonment of these descriptors stems from recognition that they oversimplify a highly heterogeneous disease and can inadvertently delay accurate diagnosis. Patients who do not fit the classic physical stereotypes often experience diagnostic delays, as clinicians may discount their symptoms if they present without expected weight changes or skin discoloration. Furthermore, the terms reduce complex, multidimensional disease processes to reductive physical caricatures, which many patients find demeaning and stigmatizing.
Clinical studies consistently demonstrate that pure phenotypic presentations occur in less than twenty percent of diagnosed individuals. Most patients exhibit overlapping pathology, with CT imaging revealing coexisting emphysematous regions alongside airway wall thickening and mucus plugging. Supplemental oxygen therapy, now standard for advanced disease, effectively eliminates cyanosis, rendering the blue descriptor clinically obsolete. Similarly, improved nutritional counseling and pulmonary rehabilitation have mitigated the extreme cachexia historically associated with the pink puffer presentation.
The Shift Toward Precision Phenotyping and Guideline-Driven Care
Modern respiratory medicine employs the Global Initiative for Chronic Obstructive Lung Disease (GOLD) strategy, which classifies patients based on symptom burden, exacerbation frequency, spirometric severity, and blood eosinophil counts. This evidence-based framework directly informs pharmacologic selection, prioritizing combination inhalers, biologic therapies, and targeted pulmonary rehabilitation over outdated physical descriptors.
High-resolution computed tomography and quantitative imaging now allow precise measurement of emphysema percentage, airway wall thickness, and vascular remodeling. Blood biomarkers, including C-reactive protein, eosinophils, and fibrinogen, predict exacerbation risk and treatment responsiveness more accurately than visual inspection. Consequently, the copd pink puffer blue bloater terminology persists only as a historical teaching concept, gradually replaced by patient-centered, multidimensional classification systems that prioritize functional status and quality of life.
Evidence-Based Management and Treatment Strategies
Targeted Approaches for Emphysema-Dominant Disease
Management focuses on reducing dynamic hyperinflation, improving exercise tolerance, and preserving remaining alveolar surface area. Long-acting muscarinic antagonists and beta-2 agonists form the pharmacological cornerstone, relaxing bronchial smooth muscle and delaying expiratory airway collapse. In selected patients with upper lobe-predominant disease and severe hyperinflation, lung volume reduction surgery or endobronchial valve implantation can improve diaphragmatic mechanics and increase FEV1.
Nutritional intervention is equally critical. Patients experiencing cachexia benefit from high-calorie, protein-dense diets divided into smaller, frequent meals to avoid gastric distension and diaphragmatic splinting. Resistance training preserves skeletal muscle mass, while aerobic conditioning improves oxygen utilization efficiency. Pursed-lip breathing and diaphragmatic retraining remain foundational techniques, taught through structured pulmonary rehabilitation programs that demonstrate measurable improvements in six-minute walk distances and dyspnea scores.
Targeted Approaches for Chronic Bronchitis-Dominant Disease
Therapeutic priorities center on enhancing mucociliary clearance, reducing exacerbation frequency, and managing cor pulmonale complications. Mucolytic agents like carbocisteine and N-acetylcysteine thin viscous secretions, facilitating expectoration and reducing bacterial colonization. Regular use of oscillatory positive expiratory pressure devices and supervised huff-coughing techniques significantly improves airway clearance efficiency.
For patients with chronic hypoxemia, long-term supplemental oxygen therapy (minimum fifteen hours daily) remains the only intervention proven to reduce mortality and slow pulmonary hypertension progression. Diuretics may be cautiously prescribed to manage peripheral edema and right ventricular volume overload, though careful monitoring prevents electrolyte imbalances and dehydration. Vaccination against Streptococcus pneumoniae, influenza, and respiratory syncytial virus substantially reduces severe exacerbation rates, preserving baseline lung function.
Universal Interventions and Lifestyle Modifications
Regardless of phenotypic predominance, complete smoking cessation remains the most effective intervention for altering disease trajectory. Behavioral counseling combined with pharmacotherapy including varenicline, bupropion, or nicotine replacement therapy significantly improves quit rates. Environmental modifications, such as HEPA air filtration, avoidance of occupational dust and chemical exposures, and proper humidity control, reduce chronic airway irritation.
Early antibiotic administration guided by symptom exacerbation criteria prevents progression to respiratory failure. Structured action plans, developed collaboratively with healthcare providers, empower patients to recognize warning signs, adjust maintenance medications appropriately, and seek timely emergency care when indicated. Regular follow-up spirometry, six-minute walk testing, and quality-of-life assessments ensure treatment alignment with individual goals and functional capacity.
Living Well: Practical Tips for Patients and Caregivers
Navigating chronic obstructive pulmonary disease requires a proactive, multidimensional approach that extends far beyond daily inhaler use. Implementing consistent energy conservation techniques allows patients to complete essential daily activities without triggering severe dyspnea. Pacing strategies involve breaking tasks into manageable segments, sitting while showering or preparing meals, and utilizing adaptive equipment such as wheeled carts or long-handled tools to minimize overhead reaching.
Sleep hygiene significantly impacts respiratory function, particularly for individuals experiencing nocturnal desaturation. Elevating the head of the bed, maintaining cool room temperatures, and avoiding heavy evening meals reduce diaphragmatic pressure and improve ventilatory efficiency during sleep. Caregivers should be trained in recognizing early exacerbation indicators, including increased sputum purulence, rapid onset of fatigue, unexplained weight gain, and altered mental status, which warrant prompt medical evaluation.
Mental health support remains an underutilized component of comprehensive COPD management. Chronic breathlessness frequently coexists with anxiety and depression, creating a vicious cycle where psychological distress increases respiratory rate and muscle tension, further worsening oxygenation. Cognitive behavioral therapy, mindfulness-based stress reduction, and peer support groups provide effective coping strategies, reducing hospitalization rates and improving overall treatment adherence.
Nutritional optimization should address both extremes of the disease spectrum. Emphysema-predominant patients require calorie-dense, anti-inflammatory diets rich in omega-3 fatty acids, lean proteins, and antioxidant vitamins to counteract systemic catabolism. Chronic bronchitis-predominant patients benefit from sodium restriction, adequate hydration to thin respiratory secretions, and balanced macronutrient intake to prevent excessive weight gain that compromises diaphragmatic excursion.
Frequently Asked Questions
What exactly defines the copd pink puffer blue bloater classification system?
The classification originated in the 1950s to describe two observable clinical patterns among patients with chronic airflow obstruction. The pink puffer category represents emphysema-predominant disease, characterized by thin body habitus, severe dyspnea, hyperinflated lungs, and maintained oxygen levels through rapid breathing. The blue bloater category represents chronic bronchitis-predominant disease, featuring chronic productive cough, cyanosis from low blood oxygen, fluid retention, and elevated carbon dioxide levels. While historically useful, modern pulmonology recognizes that most patients exhibit mixed features, making strict classification increasingly obsolete.
How do pulmonary function tests differentiate between these two clinical patterns?
Spirometry confirms airflow obstruction in both presentations through a reduced FEV1/FVC ratio. The critical differentiator is the diffusing capacity for carbon monoxide (DLCO) test, which measures gas exchange efficiency across the alveolar-capillary membrane. Patients with emphysema-predominant disease demonstrate markedly reduced DLCO due to alveolar wall destruction and surface area loss. Patients with chronic bronchitis-predominant disease typically show preserved or mildly reduced DLCO, since their primary pathology involves conducting airway inflammation rather than gas exchange unit destruction.
Why does chronic bronchitis lead to heart complications more frequently than emphysema?
Chronic alveolar hypoxia triggers sustained pulmonary artery vasoconstriction, gradually increasing vascular resistance and elevating pulmonary artery pressures. The right ventricle compensates through hypertrophy but eventually fails under prolonged strain, resulting in cor pulmonale. This pathway is more prominent in chronic bronchitis because mucus plugging and airway narrowing create significant ventilation-perfusion mismatch, perpetuating hypoxemia. Emphysema-predominant patients typically maintain better oxygenation through compensatory hyperventilation, delaying or preventing pulmonary vascular remodeling.
Are there specific breathing exercises proven to improve daily functioning?
Pursed-lip breathing remains the most evidence-based technique, creating positive expiratory pressure that prevents premature small airway collapse, reduces air trapping, and decreases work of breathing. Diaphragmatic breathing retraining strengthens the primary respiratory muscle, improving tidal volume efficiency while reducing accessory muscle fatigue. Both techniques are best learned through supervised pulmonary rehabilitation programs, where respiratory therapists provide real-time feedback, ensure proper form, and gradually integrate these methods into functional exercise training and daily activity routines.
Can patients transition from one phenotype presentation to the other over time?
Disease progression often alters clinical presentation, though complete phenotype switching is uncommon. A patient initially presenting with chronic bronchitis features may develop significant emphysema as alveolar destruction accumulates from ongoing inflammation and oxidative stress. Conversely, aggressive smoking cessation, optimized nutrition, and pulmonary rehabilitation may improve hyperinflation and weight status in emphysema-predominant patients, masking classic physical signs. Longitudinal monitoring through spirometry, imaging, and symptom assessment provides more accurate disease tracking than relying on static physical descriptors.
Conclusion
The copd pink puffer blue bloater framework once served as a foundational teaching model, offering clinicians a rapid method for recognizing divergent disease trajectories based on physical examination findings. While modern pulmonary medicine has rightly transitioned toward precision phenotyping, symptom-driven classification, and biomarker-guided therapy, understanding the physiological principles behind these historical descriptors remains clinically valuable. Recognizing how alveolar destruction drives dynamic hyperinflation versus how airway inflammation precipitates mucus obstruction and cor pulmonale empowers patients and providers to implement targeted, evidence-based interventions.
Successful COPD management requires a comprehensive approach that prioritizes complete smoking cessation, optimized inhaler therapy, structured pulmonary rehabilitation, infection prevention, and proactive exacerbation management. Patients benefit most from individualized care plans that address their specific symptom burden, functional limitations, and comorbid conditions. By embracing modern diagnostic tools, adhering to prescribed treatment regimens, and implementing sustainable lifestyle modifications, individuals living with chronic obstructive pulmonary disease can significantly improve respiratory function, reduce hospitalizations, and maintain meaningful quality of life. For personalized guidance, always consult a board-certified pulmonologist or respiratory therapist who can tailor interventions to your unique clinical profile and long-term wellness goals.

About the author
Evelyn Reed, MD, is double board-certified in pulmonary disease and critical care medicine. She is the Medical Director of the Medical Intensive Care Unit (MICU) at a major hospital in Denver, Colorado, with research interests in ARDS and sepsis.