Tendon Ligament Difference: A Complete Guide to Anatomy, Injuries, and Treatment

Every step you take, every weight you lift, and every twist your body makes relies on an intricate network of fibrous connective tissues working in perfect harmony. Yet, when pain strikes your joints or limits your mobility, it can be incredibly difficult to distinguish whether the underlying issue stems from a strained muscle attachment or a damaged joint stabilizer. Understanding the tendon ligament difference is not merely an academic exercise; it is a foundational element of accurate self-assessment, effective injury management, and long-term musculoskeletal health. These two tissue types are frequently confused in everyday language, but they possess vastly different structural properties, physiological functions, and healing trajectories. By exploring their distinct anatomical roles, injury mechanisms, and evidence-based recovery pathways, you can make informed decisions that protect your joints, accelerate healing, and prevent recurrent damage. This comprehensive guide will walk you through everything from microscopic collagen alignment to practical rehabilitation protocols, ensuring you have the medical knowledge needed to navigate soft tissue injuries safely and effectively.
The Fundamental Anatomy: What Connects What?
To truly grasp the tendon ligament difference, we must first examine their foundational roles within the musculoskeletal framework. The human body contains approximately four thousand tendons and an even more extensive network of ligaments, all meticulously engineered to withstand tremendous mechanical stress while facilitating controlled movement and structural integrity.
Understanding Tendons: Muscle-to-Bone Bridges
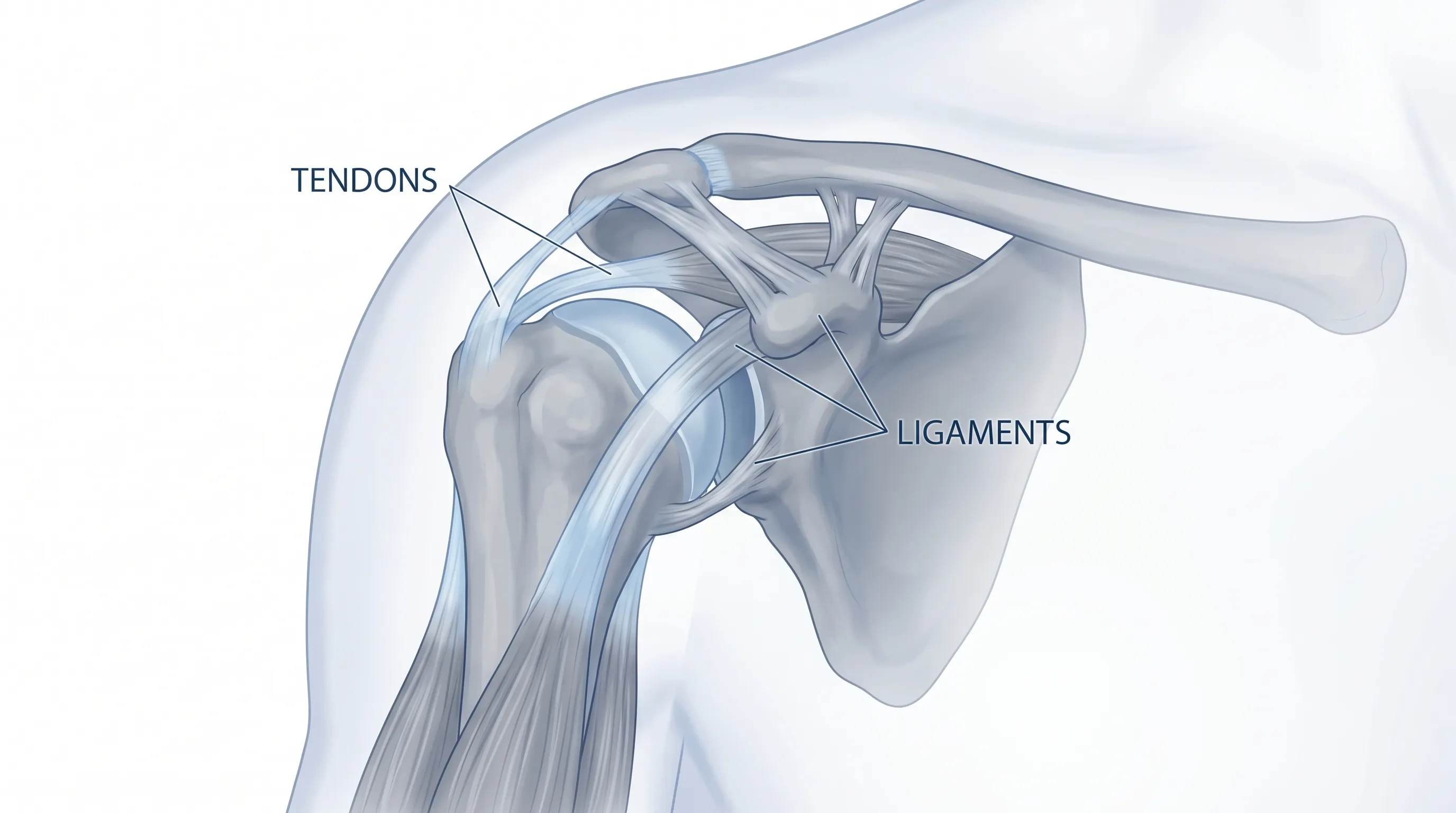
Tendons serve as the critical mechanical link between your contractile muscle fibers and the rigid skeletal framework. When a muscle contracts, it generates force. However, that force cannot translate into joint movement unless it is efficiently transferred across a highly specialized interface. This is precisely where tendons operate. Acting as biological shock absorbers and force transmitters, tendons endure tensile loads that can exceed several times your body weight during dynamic activities like sprinting or jumping. Their primary mandate is to convert muscular contraction into skeletal leverage, enabling everything from delicate finger movements to powerful athletic propulsion.
Tendons are strategically distributed throughout the body, with the most mechanically vulnerable and commonly injured sites located at the shoulders (rotator cuff tendons), elbows, wrists, knees (patellar tendon), and heels (Achilles tendon). The Achilles, in particular, represents the thickest and strongest tendon in the human body, yet it remains highly susceptible to overuse injuries due to its repetitive loading during gait and athletic maneuvers.
Understanding Ligaments: Bone-to-Bone Stabilizers
In contrast, ligaments function primarily as joint stabilizers rather than movement enablers. By connecting bone directly to adjacent bone across synovial joints, ligaments restrict excessive or aberrant motion while permitting physiological ranges of movement. Think of ligaments as biological seatbelts that prevent your joints from dislocating or moving in directions they were not designed to handle. They contain specialized proprioceptive nerve endings that constantly relay positional information to your central nervous system, allowing your brain to make micro-adjustments that maintain balance and joint alignment.
The most frequently injured ligaments are found in highly mobile, weight-bearing joints that experience multidirectional forces. The lateral ligaments of the ankle are injured far more often than any other in the human body, typically when the foot rolls inward during walking or sports. The medial and lateral collateral ligaments of the knee, along with the crucial anterior cruciate ligament (ACL), are also exceptionally vulnerable to traumatic tearing, particularly during sudden deceleration, pivoting, or direct impact scenarios. Recognizing the tendon ligament difference becomes especially critical when determining appropriate initial management, as joint instability from ligament trauma requires fundamentally different protective strategies than the muscle weakness associated with tendon strains.
Structural Composition: A Microscopic Deep Dive
At the cellular level, both tendons and ligaments are composed primarily of dense regular connective tissue dominated by collagen. However, their microscopic organization, cellular composition, and extracellular matrix characteristics diverge significantly, directly influencing their mechanical behavior and injury responses.
Cellular Architecture of Tendons
Tendons are engineered for maximum tensile strength through highly organized structural alignment. They are composed of approximately 60 to 85 percent dry-weight collagen, with Type I collagen comprising 60 to 80 percent of that total. Type I collagen fibers are exceptionally strong and are densely packed in parallel arrays that run precisely along the axis of anticipated force. This parallel alignment minimizes shear stress and maximizes load-bearing capacity. Scattered within this dense matrix are specialized fibroblasts known as tenocytes. These elongated cells reside between collagen fascicles and continuously synthesize extracellular matrix components, repairing microdamage and adapting tissue density in response to mechanical loading. The remaining 15 to 40 percent of tendon tissue consists of non-collagenous components, including proteoglycans that retain water and provide compressive resistance, along with small amounts of Type III, IV, V, and VI collagens that facilitate matrix organization.
Tendons attach securely to bone through a highly specialized transitional structure known as Sharpey's fibers. These mineralized collagen extensions penetrate directly into the bone matrix, creating a seamless gradient from flexible soft tissue to rigid osseous structure. This gradation is essential for dissipating stress concentrations at the bone-tendon interface, which would otherwise lead to avulsion fractures or attachment site failures.
Elastic Properties and Collagen Alignment in Ligaments
Ligaments also rely heavily on Type I collagen for structural integrity, but their fiber organization and matrix composition differ meaningfully from tendons. While ligaments still feature densely packed collagen bundles, they contain a notably higher concentration of elastic fibers. This increased elastin content grants ligaments a degree of controlled flexibility, allowing them to stretch slightly under physiological loads before recoiling to maintain joint stability. Additionally, ligament collagen fibers are arranged in a more irregular, multi-directional weave rather than the strictly parallel alignment seen in tendons. This architectural variation reflects their functional requirement to stabilize joints across multiple planes of motion rather than simply transmitting unidirectional force.
Ligaments possess fewer tenocytes per unit volume compared to tendons, and their cellular activity is generally lower at rest. However, they demonstrate remarkable adaptive capacity when subjected to appropriate mechanical stimuli. The extracellular matrix of ligaments contains different proportions of proteoglycans and glycosaminoglycans, which contribute to joint lubrication and nutrient diffusion across avascular or poorly vascularized regions. Understanding these structural nuances clarifies why the tendon ligament difference extends beyond simple function and directly dictates their respective healing capacities, vulnerability profiles, and rehabilitation requirements.
| Structural Feature | Tendons | Ligaments |
|---|---|---|
| Primary Connection | Muscle to bone | Bone to bone |
| Collagen Alignment | Strictly parallel bundles | Irregular, multi-directional weave |
| Dominant Collagen Type | Type I (60-80% of dry mass) | Type I, with higher Type III proportion |
| Elastic Fiber Content | Low (focuses on tensile strength) | Moderate to high (allows controlled recoil) |
| Primary Cell Type | Tenocytes (highly active) | Fibroblasts/Ligamentocytes (moderate activity) |
| Bone Attachment | Sharpey's fibers | Direct osseous integration |
| Blood Supply | Moderate (better proximally) | Limited to sparse (varies by location) |
Injury Classification: Sprains vs. Strains Explained
When connective tissue fails under mechanical stress, the resulting injury is clinically classified based on the specific structure damaged. Confusing these classifications can lead to inappropriate treatment choices and prolonged recovery times. Medical professionals strictly differentiate between the two based on the tendon ligament difference.
How Sprains Occur and Their Grading System
A sprain represents trauma to a ligament, typically resulting from sudden stretching beyond its physiological range or direct impact that forces a joint into abnormal alignment. The American Academy of Orthopaedic Surgeons (AAOS) classifies ligament sprains into three distinct severity grades. Grade 1 sprains involve microscopic tearing of ligament fibers with minimal structural disruption, presenting as localized tenderness and mild swelling but retaining full joint stability. Grade 2 sprains feature partial macroscopic tearing, resulting in measurable joint laxity, moderate swelling, bruising, and noticeable functional impairment. Grade 3 sprains constitute complete ligament rupture, often accompanied by a audible or palpable pop at the moment of injury, immediate swelling, joint instability, and inability to bear weight or utilize the affected limb.
Sprains most commonly affect the ankles, knees, and wrists due to their mobility and exposure to unpredictable mechanical forces. An ankle sprain typically occurs when the foot suddenly inverts, placing extreme tensile stress on the lateral collateral ligaments. Knee sprains frequently result from sudden twisting motions or valgus stress that compromises the medial collateral ligament or ACL. Wrist sprains are classically seen in individuals who fall onto an outstretched hand, forcing the carpal joints into hyperextension.
Understanding Strains: From Microtears to Ruptures
Strains affect the muscle-tendon unit and range from mild microscopic overstretching to complete tendon avulsion. Unlike sprains, strains can occur at any point along the continuum from the muscle belly to the osseous attachment site, though they are most frequently diagnosed at the musculotendinous junction where tissue architecture transitions. Strains are particularly common in high-velocity sports requiring explosive starts and stops. Basketball players, sprinters, and long jumpers frequently experience hamstring strains, while soccer players and tennis players are highly susceptible to calf and Achilles tendon strains. Athletes in gripping-intensive disciplines like gymnastics, rowing, or golf often develop forearm and wrist flexor/extensor strains.
The clinical presentation of strains includes localized pain along the muscle or tendon path, muscle spasms, palpable weakness, cramping, and swelling. Unlike ligament injuries, strains rarely cause profound joint instability unless the tendon completely detaches from the bone, which requires immediate orthopedic evaluation. High-risk strain activities share common biomechanical themes: inadequate warm-up, sudden intensity spikes, muscle fatigue, poor flexibility, and improper movement mechanics. Recognizing whether your injury is a strain or sprain is essential, as early loading strategies that benefit tendon recovery can exacerbate ligamentous joint instability if applied incorrectly.
Common Symptoms and Diagnostic Clues
Accurate identification of soft tissue trauma requires careful observation of symptom onset, progression, and localization. Medical professionals utilize these clinical markers alongside imaging modalities to formulate precise treatment plans.
Recognizing Tendon Inflammation (Tendinitis)
Tendinitis describes the acute inflammatory phase of tendon injury, typically triggered by sudden overload or repetitive microtrauma that overwhelms the tissue's repair mechanisms. The Mayo Clinic identifies repetitive movements as the predominant causative factor, particularly in occupations requiring overhead reaching, sustained gripping, or awkward postural positions. Common anatomical sites include the rotator cuff (shoulders), common extensor origin (tennis elbow), common flexor origin (golfer's elbow), patellar tendon (jumper's knee), and Achilles tendon. Patients typically experience localized aching that worsens with specific movements, morning stiffness, and a burning sensation during activity. Swelling may be visible or palpable along the tendon sheath, and crepitus (a grating sensation) may accompany joint motion in chronic cases.
Age serves as a significant risk factor, as tendons progressively lose water content and elasticity, reducing their capacity to absorb mechanical stress. Certain medications, particularly fluoroquinolone antibiotics, systemic corticosteroids, and aromatase inhibitors, substantially increase rupture risk by disrupting collagen synthesis pathways. Systemic conditions like diabetes mellitus and rheumatoid arthritis also compromise tendon vascularity and healing potential. Without appropriate intervention, acute tendinitis can transition to tendinosis, a degenerative state characterized by disorganized collagen, neovascularization, and chronic pain that becomes increasingly resistant to conservative management.
Identifying Acute Ligament Trauma
Ligament injuries typically present with immediate, sharp pain localized directly over the affected joint. Swelling develops rapidly as hemarthrosis (blood accumulation within the joint capsule) or periarticular edema occurs. Ecchymosis (bruising) often migrates distally due to gravity within 24 to 48 hours. Patients frequently report a distinct popping or tearing sensation at the moment of injury, followed by immediate functional compromise and joint instability.
Diagnostic accuracy relies heavily on clinical orthopedic testing. Ligament integrity is assessed through stress examinations that evaluate joint laxity across multiple planes. Lachman and anterior drawer tests evaluate ACL integrity, varus and valgus stress tests assess collateral ligaments, and anterior drawer or talar tilt tests examine ankle ligament complexes. Advanced imaging, particularly magnetic resonance imaging (MRI), provides definitive visualization of partial versus complete tears, meniscal involvement, and associated cartilage damage. Ultrasound offers dynamic, real-time assessment of ligament behavior during controlled joint movement. Differentiating ligament trauma from tendinopathy or muscle strains remains essential, as the tendon ligament difference dictates whether early immobilization and bracing should take priority over progressive mechanical loading.
Evidence-Based Treatment Pathways
Effective soft tissue injury management follows a phased, evidence-based approach that prioritizes inflammation control, tissue protection, gradual mechanical stimulation, and functional restoration. Treatment strategies diverge significantly based on whether the injury involves tendons or ligaments.
Immediate First Aid: The RICE Protocol and Beyond
The universally recommended initial intervention for acute sprains and strains remains the RICE protocol, as endorsed by the AAOS and the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS). Rest involves immediately ceasing the aggravating activity to prevent further structural damage and initiating protective loading limitations. Ice application should utilize cold packs or cryotherapy wraps applied for 15 to 20 minutes per hour during the first 48 to 72 hours, always separated from direct skin contact by a thin cloth to prevent thermal injury. Compression involves wrapping the affected area with an elastic bandage or neoprene sleeve to limit extravascular fluid accumulation and provide proprioceptive feedback. Elevation requires positioning the injured limb above cardiac level to facilitate venous and lymphatic drainage, significantly reducing swelling and pain.
Modern sports medicine has evolved the RICE concept to include POLICE (Protection, Optimal Loading, Ice, Compression, Elevation) and PEACE & LOVE protocols, emphasizing that complete immobilization should be brief. Controlled, pain-free range of motion exercises initiated within 48 to 72 hours stimulate collagen realignment, prevent adhesions, and accelerate tissue remodeling. However, optimal loading parameters differ between tissues: ligaments require protected stabilization to prevent permanent elongation, while tendons benefit from early, progressive eccentric loading to normalize collagen architecture.
Rehabilitation, Bracing, and Surgical Interventions
Rehabilitation for sprains focuses heavily on joint stabilization and proprioceptive retraining. Physical therapists utilize hinged braces for knees and CAM walking boots or lace-up stabilizers for ankles to restrict pathological movement while permitting controlled weight-bearing. Rehabilitation progresses through distinct phases: initial swelling management and pain control, followed by neuromuscular re-education, progressive strengthening of dynamic stabilizers, plyometric training for tissue resilience, and sport-specific functional drills. Severe Grade 3 ligament tears or complete ACL ruptures often require arthroscopic surgical reconstruction, particularly in active individuals or those experiencing chronic instability despite conservative management.
Strain and tendinitis rehabilitation emphasizes progressive mechanical loading, particularly eccentric exercises where the muscle lengthens under tension. Eccentric protocols have demonstrated superior outcomes in Achilles and patellar tendinopathy by stimulating collagen synthesis, increasing tendon stiffness, and promoting organized fiber alignment. Physical therapy incorporates therapeutic ultrasound, instrument-assisted soft tissue mobilization, dry needling, and targeted strengthening of antagonistic muscle groups to correct biomechanical imbalances. Chronic cases unresponsive to 3 to 6 months of structured conservative therapy may require percutaneous needle fenestration, platelet-rich plasma (PRP) injections, or surgical debridement to remove degenerative tissue and initiate fresh healing cascades. Understanding the tendon ligament difference ensures clinicians select the most appropriate rehabilitation velocity and loading parameters for each patient.

Prevention Strategies and Long-Term Joint Health
Prevention remains the most cost-effective and clinically successful approach to soft tissue injury management. Implementing structured preventive strategies reduces acute trauma incidence, minimizes chronic degeneration, and preserves lifelong mobility.
Training Modifications and Cross-Training
The foundation of injury prevention lies in intelligent programming and biomechanical awareness. Athletes and fitness enthusiasts must prioritize gradual progression, avoiding sudden spikes in training volume, intensity, or frequency that exceed tissue adaptive capacity. The 10 percent rule provides a practical guideline: increase weekly training load by no more than 10 percent to allow connective tissues adequate time to remodel. Cross-training significantly reduces repetitive strain injuries by distributing mechanical stress across multiple musculoskeletal pathways. Runners should incorporate cycling or swimming to maintain cardiovascular fitness while reducing impact loading. Strength training must emphasize balanced development between agonist and antagonist muscle groups; neglecting posterior chain development frequently precipitates anterior knee tendinitis and hamstring strains.
Improving movement technique remains paramount. Poor squat mechanics, overstriding during running, or improper racquet grip placement all create abnormal force vectors that concentrate stress on specific tendons and ligaments. Engaging qualified coaches for biomechanical analysis, utilizing video feedback, and prioritizing form over weight load dramatically reduces injury susceptibility. Proper equipment selection, including footwear with adequate cushioning, arch support, and sport-specific traction patterns, ensures optimal force distribution across joints. Additionally, incorporating regular dynamic warm-ups that elevate tissue temperature and enhance viscoelastic properties before intense activity significantly lowers acute tear risk.
Nutrition, Hydration, and Medical Risk Factors
Connective tissue health extends far beyond mechanical factors; it is profoundly influenced by systemic physiology and nutritional status. Adequate protein consumption provides essential amino acids for collagen synthesis, with glycine and proline serving as critical building blocks. Vitamin C supplementation or dietary optimization through citrus fruits, bell peppers, and broccoli supports proline hydroxylase activity, which is mandatory for stable collagen triple-helix formation. Zinc, copper, and manganese act as enzymatic cofactors that facilitate cross-linking and matrix maturation.
Hydration status directly impacts tissue viscoelasticity. Dehydrated tendons and ligaments exhibit reduced shock-absorbing capacity and increased brittleness, elevating rupture risk during high-velocity movements. Conversely, certain medications require heightened vigilance. Fluoroquinolone antibiotics carry a well-documented black box warning for tendinitis and tendon rupture, particularly in patients over 60 or those concurrently using corticosteroids. Long-term corticosteroid use suppresses inflammatory healing responses and weakens collagen matrix density. Patients with diabetes, thyroid disorders, or rheumatological conditions must collaborate closely with healthcare providers to optimize systemic inflammation markers and blood glucose control, as hyperglycemia directly impairs fibroblast function and tissue repair timelines. Addressing these modifiable risk factors creates a resilient physiological environment that supports both acute injury recovery and long-term connective tissue integrity.
Frequently Asked Questions
What exactly distinguishes a sprain from a strain in clinical practice?
A sprain specifically involves damage to a ligament, which connects bone to bone and primarily stabilizes joints. A strain affects muscle tissue or the tendon that connects muscle to bone. While both present with pain, swelling, and bruising, sprains typically cause joint instability and require protective bracing, whereas strains involve muscle weakness, spasms, and respond better to controlled eccentric loading and mobility restoration.
How long does it realistically take for a torn tendon or ligament to fully heal?
Healing timelines depend heavily on injury grade, tissue vascularity, and rehabilitation compliance. Grade 1 sprains and mild strains typically resolve within 2 to 4 weeks. Grade 2 injuries require 4 to 10 weeks of structured rehabilitation. Grade 3 complete tears, whether managed conservatively or surgically, undergo a prolonged remodeling phase lasting 6 to 12 months. Full collagen maturation and return to pre-injury strength levels require progressive loading over many months, regardless of symptom resolution.
Can I continue exercising if I suspect a tendon or ligament injury?
You should immediately cease any activity that provokes sharp pain, joint instability, or significant swelling. Continuing to load injured tissue without professional guidance risks converting partial tears into complete ruptures, exacerbating chronic tendinosis, or causing permanent joint laxity. Maintain cardiovascular fitness through non-weight-bearing cross-training like swimming or stationary cycling only if it remains entirely pain-free, and consult a physical therapist or sports medicine physician before returning to sport-specific loading.
Why do certain medications like fluoroquinolones increase tendon rupture risk?
Fluoroquinolone antibiotics disrupt tenocyte function and alter collagen synthesis pathways by inhibiting critical enzymes responsible for maintaining extracellular matrix integrity. They also upregulate matrix metalloproteinases, which degrade collagen faster than it can be replaced, and reduce tendon vascularization. This biochemical disruption creates tissue that appears structurally normal but exhibits significantly reduced tensile strength, making it highly susceptible to rupture under normal physiological loads.
What are the most reliable early warning signs that I am developing tendinitis or tendon degeneration?
Early indicators include localized aching that intensifies during specific movements but subsides at rest, morning stiffness lasting longer than 10 minutes, reduced range of motion, and a sensation of tissue thickening or nodularity along the tendon path. Pain that initially appears only at the beginning of exercise but diminishes after warming up often progresses to pain that persists throughout activity and continues afterward. Recognizing these patterns early allows for timely intervention through load management, eccentric strengthening, and biomechanical correction before irreversible structural changes occur.
Conclusion
Mastering the tendon ligament difference empowers you to make informed, evidence-based decisions about your musculoskeletal health. Tendons and ligaments, though composed of similar collagen-rich connective tissue, serve fundamentally different mechanical roles. Tendons act as dynamic force transmitters linking muscle to bone, demanding progressive loading strategies and eccentric rehabilitation to maintain optimal tensile strength. Ligaments function as passive joint stabilizers connecting bone to bone, requiring protective stabilization, proprioceptive retraining, and careful load management to prevent permanent elongation or chronic instability. Whether you are navigating an acute sprain, managing persistent tendinitis, or implementing preventive strategies to safeguard your joints, understanding their unique structural properties and healing pathways is indispensable.
Effective recovery demands patience, adherence to structured rehabilitation protocols, and recognition that connective tissue remodeling operates on biological timelines rather than arbitrary calendar dates. Prioritizing gradual training progression, cross-training, proper nutrition, and professional guidance when pain persists will dramatically reduce your risk of recurrent injury. Always consult qualified healthcare providers for accurate diagnosis, particularly when experiencing joint instability, severe swelling, or inability to bear weight. By respecting the intricate biology that governs your tendons and ligaments, you lay the foundation for lifelong mobility, athletic resilience, and uncompromised joint health.
For further authoritative guidance on soft tissue injuries, consult resources from the Mayo Clinic Tendinitis Guide, the Mayo Clinic Sprains Overview, and comprehensive injury protocols from the American Academy of Orthopaedic Surgeons or NIAMS Sports Injuries Resource.

About the author
Samuel Jones, MD, is a board-certified orthopedic surgeon specializing in joint replacement and orthopedic trauma. He is a team physician for a professional sports team and practices at a renowned orthopedic institute in Georgia.