Kidney AML Tumor: Complete Guide to Causes, Diagnosis & Treatment

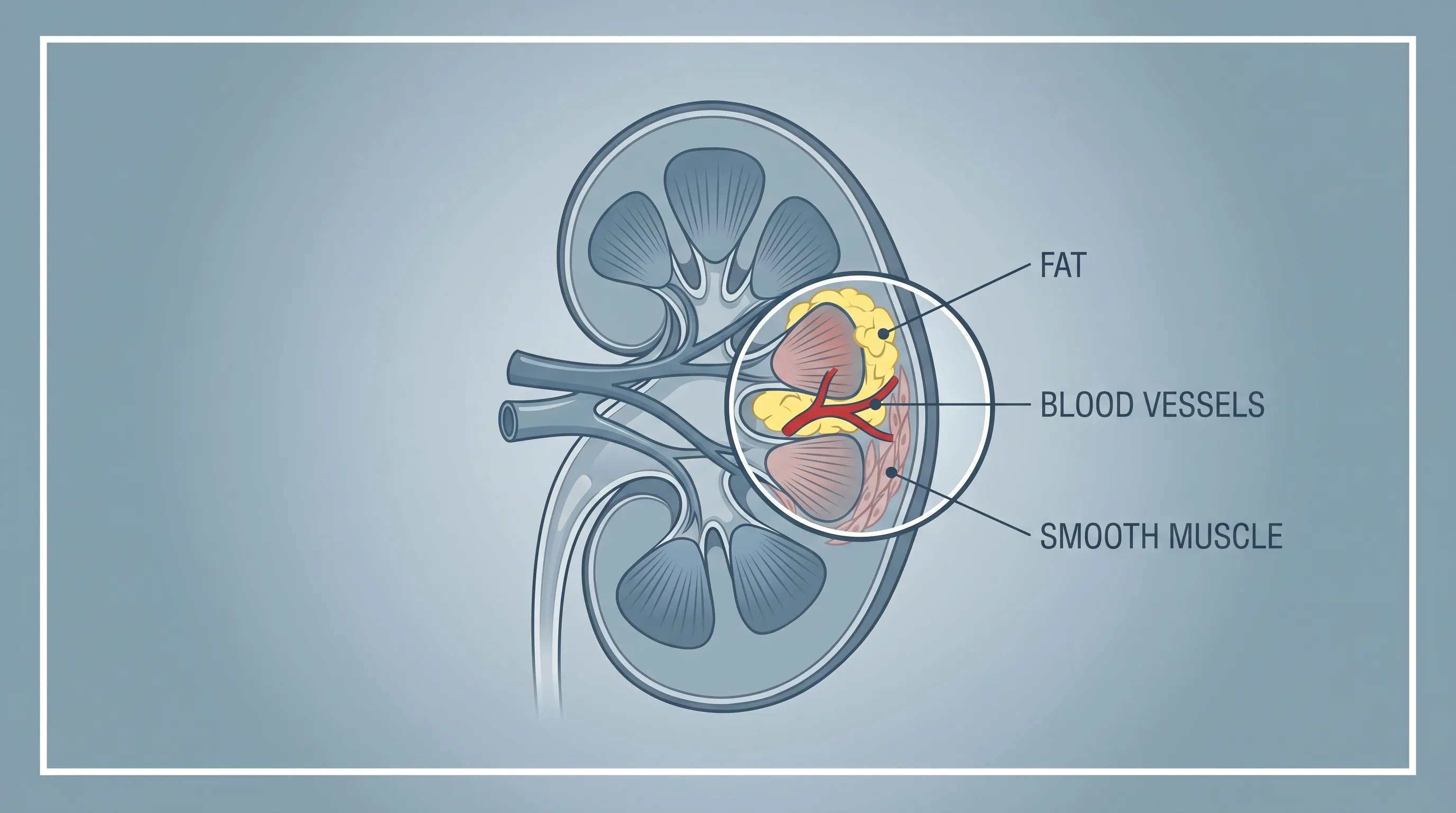
Discovering an unexpected mass during a routine medical examination can be deeply unsettling. For many individuals, the diagnosis of a kidney AML tumor arrives as an incidental finding during imaging tests ordered for completely unrelated health concerns. While the terminology may sound alarming, understanding the biological nature of this condition brings immediate reassurance. Renal angiomyolipoma represents the most frequently diagnosed benign kidney mass in adults worldwide. Unlike malignant renal cell carcinoma, a classic kidney AML tumor lacks the aggressive, invasive characteristics of true cancer. It is fundamentally a hamartomatous growth, meaning it consists of a disorganized but mature mixture of the very tissues that naturally reside in the kidney: blood vessels, smooth muscle cells, and adipose (fat) tissue. Current epidemiological data indicates that less than 1% of the general population harbors this condition, with a slight but consistent predilection for females between the ages of forty and sixty. Although the prognosis is overwhelmingly favorable, proper clinical oversight remains essential. This comprehensive guide explores the pathophysiology, diagnostic pathways, evidence-based management strategies, and long-term lifestyle considerations for individuals navigating a kidney AML tumor diagnosis. By combining established urological guidelines with recent clinical research, we provide actionable insights to help patients and caregivers make informed, confident decisions about kidney health.
What Is a Kidney AML Tumor? Understanding the Basics
The medical terminology angiomyolipoma directly describes the tumor's histological architecture. The prefix angio refers to the abnormal proliferation of thick-walled, dysmorphic blood vessels. Myo denotes the presence of smooth muscle cells that resemble normal muscular tissue but lack organized structural orientation. Lipo indicates the abundant accumulation of mature fat cells. When pathologists examine biopsy or surgical specimens, this triphasic cellular composition immediately distinguishes it from other renal neoplasms. Approximately 0.44% of individuals develop sporadic cases without any known genetic predisposition. These tumors account for roughly 1% of all renal tumors and between 2% to 3% of all clinically detected renal masses. The natural history of a kidney AML tumor typically follows an indolent course. Classic variants demonstrate remarkably slow growth patterns, averaging approximately 0.19 centimeters annually. In many documented cases, the tumor remains completely stable over decades, never causing symptoms or necessitating medical intervention.
The clinical significance of a kidney AML tumor primarily revolves around two factors: its potential size and the structural integrity of its vascular network. As these masses expand, they occupy valuable renal parenchyma, potentially compromising filtration capacity and nephron function. More critically, the blood vessels embedded within the tumor frequently lack elastic fibers and possess thickened, hyalinized walls. This structural deficiency predisposes the vasculature to microaneurysm formation, which can rupture spontaneously under certain physiological conditions. While spontaneous hemorrhage occurs in fewer than 15% of documented cases, when it does manifest, the consequences can be severe, with approximately one in three affected individuals experiencing hemorrhagic shock requiring emergency medical stabilization. Understanding this vascular vulnerability is fundamental to comprehending why urologists monitor these masses closely despite their benign classification.
Demographically, sporadic kidney AML tumor diagnoses peak in middle-aged women, though they appear across all adult age groups and genders. Hormonal influences appear to modulate tumor biology, as evidenced by accelerated growth rates observed during pregnancy and certain hormone replacement therapies. Researchers hypothesize that the high density of estrogen and progesterone receptors found within the stromal cells of these tumors directly stimulates cellular proliferation. Consequently, reproductive-age women with preexisting renal masses require specialized counseling before pursuing family planning. Regardless of demographic factors, the overarching clinical principle remains consistent: early detection, accurate radiological characterization, and personalized surveillance protocols form the cornerstone of successful management.
The Three Main Types of Renal Angiomyolipoma
Not all angiomyolipomas share identical histological features or clinical behavior. Medical literature classifies renal angiomyolipoma into three distinct subtypes, each demanding tailored diagnostic and therapeutic approaches. The classic or triphasic variant represents the overwhelming majority of cases, encompassing more than 80% of all diagnosed kidney AML tumor presentations. As previously noted, this subtype contains a balanced mixture of dysmorphic blood vessels, mature adipose tissue, and proliferative smooth muscle bundles. The abundant fat content within classic lesions creates a highly echogenic appearance on ultrasound and exhibits negative Hounsfield units on computed tomography scans, making radiological identification relatively straightforward. Patients with this variant typically experience the slowest progression rates and the lowest risk of complications.
Monophasic angiomyolipomas, conversely, present a diagnostic challenge due to their atypical cellular dominance. These masses consist predominantly of a single tissue component, either hyperplastic smooth muscle or excessive adipose deposition, while containing minimal traces of the other two elements. Fat-poor angiomyolipomas, which fall under the monophasic classification, account for approximately 5% of all cases. Because they lack the diagnostic hallmark of macroscopic fat, they frequently mimic the imaging characteristics of renal cell carcinoma. Radiologists must rely on subtle features such as the absence of calcification, distinct enhancement patterns, and occasionally perirenal stranding to differentiate them from malignant counterparts. When imaging remains inconclusive, clinicians often pursue contrast-enhanced MRI with chemical shift sequences or recommend image-guided biopsy to establish a definitive histopathological diagnosis before determining management strategies.
The third and most clinically significant subtype is the epithelioid angiomyolipoma (EAML). This rare variant constitutes less than 5% of all angiomyolipoma cases but carries substantial oncological implications. Unlike classic or monophasic forms, EAMLs are predominantly composed of atypical epithelioid cells that line abnormal blood vessel networks. Pathologists identify this variant through the absence of typical fat droplets and the presence of large, pleomorphic cells with prominent nucleoli. EAMLs exhibit unpredictable biological behavior, ranging from indolent growth to aggressive local invasion and distant metastasis. Clinical studies indicate that epithelioid variants account for the majority of AML-related mortality. Urologic oncologists closely monitor these lesions for specific high-risk features, including tumor diameter exceeding nine centimeters, venous tumor thrombus formation, extensive necrosis, and epithelioid cell composition greater than seventy percent. Patients diagnosed with this subtype require multidisciplinary care involving surgical oncology, medical oncology, and specialized pathology review.
Genetic Drivers and Associated Medical Conditions
The molecular pathogenesis of renal angiomyolipoma centers primarily on the dysregulation of the mTOR signaling pathway. Under normal physiological conditions, the mTOR complex coordinates cellular metabolism, protein synthesis, autophagy, and proliferation. Two critical tumor suppressor genes, TSC1 and TSC2, act as molecular brakes on this pathway. The TSC1 gene encodes hamartin, while TSC2 produces tuberin. These proteins form a functional heterodimer that inhibits Rheb, a small GTPase responsible for activating mTORC1. The National Institutes of Health details how TSC mutations disrupt cellular regulation, leading to uncontrolled mTOR activation. This uncontrolled signaling cascade drives excessive cellular proliferation and inhibits programmed cell death, ultimately fostering the development of hamartomatous growths like the kidney AML tumor.
Approximately 70% of renal angiomyolipomas arise sporadically, meaning the genetic mutations are somatic and confined strictly to the tumor tissue without systemic manifestation or familial transmission. However, the remaining 20% to 30% of cases emerge in the context of hereditary syndromes, with Tuberous Sclerosis Complex (TSC) representing the most prominent association. Individuals with TSC inherit autosomal dominant mutations in TSC1 or TSC2, leading to systemic manifestations including cortical tubers, subependymal nodules, facial angiofibromas, cardiac rhabdomyomas, and multiple bilateral renal AMLs. Patients with TSC-associated disease frequently develop tumors at younger ages, exhibit faster growth trajectories, and face higher risks of renal function deterioration. The prevalence of angiomyolipomas among TSC patients exceeds 75%, making renal surveillance a mandatory component of comprehensive syndrome management.
Other genetic and neurological conditions demonstrate established correlations with renal AML development. Lymphangioleiomyomatosis (LAM) shares identical TSC gene mutations and predominantly affects women of childbearing age. LAM patients commonly develop cystic lung disease alongside progressive renal angiomyolipomas, requiring coordinated pulmonary and nephrological care. Neurofibromatosis type 1 and von Hippel-Lindau disease occasionally present with renal vascular anomalies that histologically overlap with angiomyolipoma, though these represent distinct pathological entities. Genetic counseling and molecular testing become indispensable when patients present with multiple bilateral tumors, early-onset disease, or extrarenal clinical features suggestive of syndromic involvement. The CDC provides comprehensive resources on hereditary genetic testing to support these clinical evaluations. Identifying the underlying genetic etiology directly influences treatment algorithms, particularly regarding the utilization of targeted mTOR inhibitors.
Clinical Presentation: Symptoms and Warning Signs
The clinical trajectory of a kidney AML tumor remains predominantly asymptomatic, particularly during the early stages of tumor development. Radiologists frequently identify masses measuring less than three centimeters incidentally during abdominal CT scans, ultrasounds, or MRI evaluations ordered for gastrointestinal complaints, trauma assessments, or routine cancer screening protocols. When symptoms do manifest, they typically correlate with tumor dimensions exceeding four centimeters or complications arising from vascular compromise. Flank pain represents the most common presenting complaint, resulting from capsular distension, parenchymal stretching, or localized tissue necrosis within the expanding mass. This discomfort often radiates toward the lower abdomen or groin, mimicking renal colic or musculoskeletal strain.
Macroscopic hematuria occurs when tumor-associated blood vessels erode into the collecting system. While often transient, visible blood in the urine warrants immediate urological evaluation to exclude concurrent urinary tract pathology or malignant transformation. Persistent or heavy bleeding frequently induces secondary iron-deficiency anemia, manifesting as fatigue, pallor, tachycardia, and exertional dyspnea. Hypertension develops in a subset of patients due to activation of the renin-angiotensin-aldosterone system, particularly when the expanding tumor compresses renal vasculature or ischemic parenchyma. Clinicians should monitor blood pressure regularly, as poorly controlled hypertension accelerates chronic kidney disease progression.
Spontaneous retroperitoneal hemorrhage, historically termed Wunderlich syndrome, represents the most feared complication of a kidney AML tumor. Patients experiencing acute vascular rupture typically present with the classic Lenk triad: sudden flank pain, palpable abdominal mass, and signs of hypovolemic shock including tachycardia, hypotension, and diaphoresis. Emergency management prioritizes hemodynamic stabilization, blood transfusion protocols, and urgent selective arterial embolization to achieve hemostasis. Fever, nausea, and vomiting occasionally accompany large or rapidly expanding tumors due to localized inflammatory responses or gastrointestinal compression. Urinary tract infections may arise secondary to urinary stasis caused by extrinsic ureteral obstruction. Any new onset of severe flank pain, dizziness, or hemodynamic instability in a patient with known renal masses necessitates immediate emergency department evaluation.
Diagnostic Protocols and Imaging Techniques
Accurate radiological characterization serves as the foundation for safe and effective management of a kidney AML tumor. Ultrasound examination typically serves as the initial screening modality, revealing a markedly hyperechoic renal mass. The intense echogenicity directly correlates with the macroscopic fat content reflecting sound waves more efficiently than surrounding renal parenchyma. However, ultrasonography lacks the spatial resolution and tissue differentiation capabilities required for definitive diagnosis or surgical planning, prompting clinicians to pursue advanced cross-sectional imaging.
Contrast-enhanced computed tomography (CT) remains the gold standard diagnostic tool, consistent with Mayo Clinic guidelines for renal mass evaluation. Radiologists evaluate non-contrast, corticomedullary, and nephrographic phases to quantify fat density, assess vascular supply, and measure tumor dimensions precisely. The presence of macroscopic fat exhibiting attenuation values below negative ten Hounsfield units reliably confirms angiomyolipoma diagnosis with over 95% specificity. Additional diagnostic hallmarks include the absence of intratumoral calcifications, which strongly favors benign angiomyolipoma over renal cell carcinoma. CT angiography further delineates feeding arteries and identifies microaneurysms exceeding five millimeters, directly informing embolization planning and hemorrhage risk stratification.
Magnetic resonance imaging (MRI) provides superior soft-tissue contrast without ionizing radiation, making it particularly valuable for pregnant patients, individuals with contrast allergies, or those requiring long-term serial monitoring. Chemical shift MRI sequences excel at detecting microscopic fat, while diffusion-weighted imaging and dynamic contrast enhancement help differentiate fat-poor angiomyolipomas from malignant lesions. When imaging findings remain equivocal, clinicians may pursue percutaneous core needle biopsy. Histopathological evaluation utilizing immunohistochemical staining confirms diagnosis through positive expression of melanocytic markers (HMB-45, Melan-A) and smooth muscle actin, alongside negative staining for epithelial markers like cytokeratin. Pathologists carefully evaluate cellular atypia, mitotic rate, and necrosis to exclude epithelioid transformation before finalizing management recommendations.
Evidence-Based Treatment Pathways
Management strategies for a kidney AML tumor follow a risk-stratified approach balancing intervention morbidity against hemorrhage prevention. Active surveillance constitutes the first-line management paradigm for the majority of patients. Urological guidelines strongly recommend observation for asymptomatic masses measuring less than four centimeters with stable imaging characteristics. Surveillance protocols typically incorporate renal ultrasound or low-dose CT scans at six-month intervals initially, transitioning to annual or biennial evaluations once stability is confirmed over two to three years. This conservative approach preserves nephron architecture, avoids procedural complications, and maintains quality of life while ensuring timely intervention if growth accelerates.
Intervention becomes medically indicated when tumors exceed four centimeters, demonstrate growth rates surpassing 0.25 centimeters annually, contain intralesional aneurysms measuring five millimeters or larger, or provoke clinically significant symptoms. Selective arterial embolization (SAE) has emerged as the preferred first-line interventional therapy. This minimally invasive, image-guided procedure involves catheter navigation through the femoral or radial artery into renal vasculature. Interventional radiologists inject embolic agents such as ethanol, polyvinyl alcohol particles, or microcoils directly into feeding arteries, inducing targeted ischemic necrosis while preserving healthy renal tissue. Clinical studies demonstrate volume reduction exceeding fifty percent in most treated patients, with hemorrhage risk decreasing to less than two percent post-procedure. Complications remain rare but may include post-embolization syndrome, characterized by transient fever, nausea, and localized pain manageable with supportive care.
Nephron-sparing surgery (NSS), typically performed as partial nephrectomy, offers definitive tumor removal for patients unsuitable for embolization or those with complex anatomical locations compromising renal vasculature. Robotic-assisted laparoscopic techniques minimize incision size, reduce postoperative pain, and accelerate recovery while maintaining oncological safety margins. Total nephrectomy remains a last resort, reserved for massive tumors destroying functional renal tissue or life-threatening hemorrhage uncontrollable by embolization. Pharmacological intervention utilizing mTOR inhibitors such as everolimus demonstrates remarkable efficacy for patients with TSC-associated or multifocal disease. By pharmacologically inhibiting constitutively active mTORC1 signaling, these targeted therapies induce significant tumor shrinkage, reduce hemorrhage risk, and delay or eliminate the need for surgical intervention. Clinical trials confirm sustained volume reduction with manageable adverse event profiles including stomatitis, rash, and hyperlipidemia, a finding further validated by ongoing NIH-funded clinical research. The following table summarizes key management modalities:
| Treatment Approach | Indications | Mechanism of Action | Key Advantages | Potential Limitations |
|---|---|---|---|---|
| Active Surveillance | <4 cm, asymptomatic, slow growth | Periodic monitoring without intervention | Zero procedural risk, preserves renal function | Requires long-term compliance, anxiety for some patients |
| Selective Arterial Embolization | >4 cm, aneurysms ≥5 mm, symptomatic | Catheter-guided vascular occlusion | Minimally invasive, rapid recovery, high hemostasis success | Risk of post-embolization syndrome, potential need for retreatment |
| Nephron-Sparing Surgery | Complex anatomy, failed embolization, large localized masses | Surgical excision with renal preservation | Definitive removal, histological confirmation | Surgical risks, longer recovery, anesthesia exposure |
| mTOR Inhibitor Therapy | TSC-associated, bilateral/multifocal disease | Targeted pathway inhibition reducing cellular proliferation | Systemic effect on all lesions, non-invasive, kidney-sparing | Chronic medication adherence, metabolic side effects, cost |
Long-Term Management and Lifestyle Considerations
Navigating life with a kidney AML tumor requires proactive health monitoring and informed lifestyle adjustments. Renal functional deterioration represents a universal concern regardless of chosen management strategy. Chronic pressure effects, recurrent microhemorrhages, and procedural ischemic changes can progressively compromise glomerular filtration rates over decades. Consequently, longitudinal monitoring of serum creatinine, estimated glomerular filtration rate, and urinalysis remains mandatory. Patients should maintain optimal hydration, adhere to heart-healthy dietary patterns low in processed sodium, and strictly avoid nephrotoxic medications including nonsteroidal anti-inflammatory drugs (NSAIDs) unless explicitly prescribed and monitored by their care team.
Physical activity recommendations warrant individualized counseling. While regular cardiovascular exercise supports metabolic health and blood pressure control, individuals with tumors exceeding four centimeters or containing identified aneurysms should temporarily avoid high-impact contact sports, heavy weightlifting, and activities carrying significant abdominal trauma risk. These restrictions minimize mechanical stress on fragile tumor vasculature, reducing spontaneous hemorrhage likelihood. Once embolization successfully shrinks the mass or surgical removal eliminates vascular vulnerability, patients typically resume unrestricted athletic participation following physician clearance.
Reproductive health counseling constitutes a critical component of long-term management. Women of childbearing age diagnosed with a kidney AML tumor must engage in comprehensive pre-pregnancy discussions with maternal-fetal medicine specialists and urologists. Elevated estrogen and progesterone levels during gestation stimulate receptor-rich tumor cells, accelerating growth and increasing hemorrhage risk, particularly during the second and third trimesters. Prophylactic embolization before conception dramatically improves maternal and fetal safety outcomes. Genetic counseling becomes highly advisable for patients presenting with multiple, bilateral, or early-onset tumors. Identifying germline TSC mutations informs family planning decisions, enables early pediatric screening, and unlocks access to targeted therapies and clinical support networks.

Patients should establish clear communication channels with their healthcare team and promptly report emergent symptoms including sudden flank pain, hematuria, dizziness, or rapid abdominal swelling. Carrying medical identification documenting the diagnosis proves invaluable during emergency presentations when prior imaging records remain inaccessible. Adhering to prescribed surveillance intervals, maintaining blood pressure within target ranges, and participating in shared decision-making processes empower patients to actively manage their condition while preserving long-term renal function and overall quality of life.
The Epithelioid Variant: Prognosis and Specialized Care
While the prognosis for classic angiomyolipoma remains overwhelmingly favorable, the epithelioid variant demands heightened clinical vigilance and aggressive multidisciplinary management. EAML accounts for a small fraction of diagnosed cases but demonstrates unpredictable biological behavior that occasionally crosses into malignant territory. Pathological evaluation focuses on quantifying epithelioid cell percentage, assessing nuclear atypia, measuring tumor dimensions, and identifying venous invasion or necrotic tissue regions. When tumors reach or exceed nine centimeters, contain greater than sixty to seventy percent epithelioid cells, or demonstrate vascular thrombus extension, clinical outcomes deteriorate significantly due to elevated metastatic potential.
Immunohistochemical profiling confirms diagnosis through strong positivity for melanocytic markers including HMB-45 and Melan-A, alongside consistent negativity for epithelial cytokeratins and neural S100 proteins. Distinguishing EAML from metastatic melanoma or clear cell renal carcinoma requires expert pathological correlation and molecular testing when morphological features overlap. Therapeutic strategies integrate complete surgical resection when anatomically feasible, followed by adjuvant mTOR inhibitor therapy to suppress residual disease progression. Advanced cases unresponsive to conventional interventions may benefit from clinical trial enrollment exploring immune checkpoint inhibitors or combination targeted therapies, though robust longitudinal data remains under active investigation. Long-term surveillance protocols mandate cross-sectional imaging of the chest, abdomen, and pelvis every three to six months initially, transitioning to extended intervals upon demonstrated stability.
Overall prognosis hinges on early recognition, histological grading, and access to specialized urologic oncology centers. Patients with localized disease treated promptly experience prolonged survival comparable to low-grade renal malignancies. Conversely, advanced presentations with distant metastases or extensive venous invasion face substantial challenges requiring palliative symptom management and systemic disease control. Ongoing research into genomic profiling and biomarker identification promises refined risk stratification and personalized therapeutic algorithms in the coming decade.
Frequently Asked Questions
Is a kidney AML tumor cancerous?
The vast majority of kidney AML tumors are benign, meaning they are noncancerous and do not invade surrounding tissues or metastasize to distant organs. They consist of a disorganized mixture of mature blood vessels, smooth muscle, and fat cells. However, a rare subtype known as epithelioid angiomyolipoma carries malignant potential and requires specialized oncological monitoring and intervention.
At what size does a renal angiomyolipoma require treatment?
Urological guidelines generally recommend considering active intervention when a kidney AML tumor exceeds four centimeters in maximum diameter. Additional triggers include documented growth rates faster than 0.25 centimeters per year, the presence of intralesional microaneurysms measuring five millimeters or larger, onset of persistent flank pain, or macroscopic hematuria. Smaller, asymptomatic lesions typically undergo conservative surveillance.
Can pregnancy affect a kidney AML tumor?
Yes, pregnancy significantly influences tumor biology. Classic angiomyolipomas express high densities of estrogen and progesterone receptors. Elevated hormonal concentrations during gestation directly stimulate cellular proliferation, frequently causing accelerated growth. This physiological expansion substantially increases the risk of spontaneous vascular rupture, particularly during the second and third trimesters. Pre-pregnancy counseling and prophylactic treatment are strongly advised for women with known masses.
What is the difference between active surveillance and selective embolization?
Active surveillance involves periodic imaging evaluations and clinical monitoring without immediate procedural intervention, representing the standard of care for small, asymptomatic lesions. Selective arterial embolization constitutes a minimally invasive radiological procedure where a catheter delivers embolic agents directly into the tumor's feeding arteries, inducing targeted ischemia and volume reduction. Embolization becomes the preferred approach when tumors exceed four centimeters or exhibit high-risk vascular features.
Are kidney AML tumors linked to genetic conditions?
Approximately 20% to 30% of renal angiomyolipomas occur in association with hereditary syndromes. Tuberous Sclerosis Complex represents the most prevalent connection, often presenting with multiple bilateral tumors at younger ages. Other associated conditions include lymphangioleiomyomatosis, neurofibromatosis type 1, and von Hippel-Lindau disease. Patients with bilateral or multifocal disease should undergo comprehensive genetic counseling and molecular testing to evaluate underlying hereditary drivers.
Conclusion
Receiving a diagnosis of a kidney AML tumor initially generates understandable apprehension, yet current medical evidence overwhelmingly supports a favorable clinical trajectory for the vast majority of patients. Understanding that these masses represent benign hamartomatous growths rather than aggressive malignancies provides crucial psychological relief. The cornerstone of successful management lies in personalized risk stratification, adhering to structured surveillance protocols, and timely intervention when specific size thresholds, growth patterns, or symptomatic presentations emerge. Advances in minimally invasive techniques such as selective arterial embolization and targeted pharmacological therapies utilizing mTOR inhibitors have dramatically reduced procedural morbidity while preserving vital renal parenchyma. Patients must remain engaged in their care through regular follow-up appointments, blood pressure monitoring, symptom awareness, and informed reproductive health planning. By partnering closely with urologists, interventional radiologists, and genetic counselors, individuals can confidently navigate their diagnosis, minimize complications, and maintain optimal kidney function throughout their lifespan. Continued research into genomic profiling and novel targeted agents promises even more precise, individualized treatment pathways in the years ahead.
About the author
Carlos Ruiz, MD, FACS, is a board-certified urologist specializing in minimally invasive and robotic surgery for urologic cancers. He is a senior partner at a large urology group in Houston, Texas, and is involved in clinical trials for new prostate cancer treatments.