Is a Creatinine Level of 1.7 Dangerous? Understanding Your Kidney Health

Key points
- Age and Sex: Normal ranges differ between men and women, and kidney function naturally declines with age. As we get older, the glomerular filtration rate gradually decreases, and muscle mass changes, altering baseline creatinine production and clearance rates.
- Muscle Mass: Individuals with more muscle mass (like athletes) naturally produce more creatinine. A 1.7 might be less concerning for a bodybuilder than for a frail, elderly person. Conversely, individuals with low muscle mass may have artificially low creatinine levels, masking underlying kidney dysfunction until significant damage has already occurred.
- Baseline Level: If your creatinine has been stable around 1.4 and crept up to 1.7, it's different from it suddenly jumping from 0.8 to 1.7. A gradual increase often points toward chronic kidney disease (CKD) progression, while a rapid spike typically indicates acute kidney injury (AKI), which may be reversible with prompt treatment.
- Underlying Health Conditions: The result is more significant in individuals with diabetes, high blood pressure, or heart disease. These conditions place continuous hemodynamic stress on the renal vasculature and filtration units, making the kidneys more susceptible to functional decline.
- Hydration Status: Recent fluid intake heavily influences blood concentration. Dehydration can cause transient elevations, while overhydration might temporarily dilute serum markers.
Receiving a blood test result showing a creatinine level of 1.7 mg/dL can be unsettling. This number is outside the typical normal range, and it's natural to wonder what it means for your health. While a 1.7 creatinine level is a clear signal that you need to consult a healthcare professional, understanding the context behind this number is crucial to determining its seriousness. In today's medical landscape, where routine blood panels have become standard components of preventive healthcare, encountering an out-of-range value often triggers anxiety. However, modern nephrology emphasizes that lab values are starting points, not final diagnoses. The kidneys are remarkably resilient organs, and early detection of functional changes allows for timely interventions that can slow or even reverse damage.
This article will break down what a creatinine level of 1.7 mg/dL signifies, its potential causes, the symptoms to watch for, and the necessary next steps to protect your kidney health. We will also explore the physiological mechanisms behind creatinine production, how healthcare providers interpret these results alongside complementary markers, and the evidence-based strategies used to manage elevated levels effectively. By the end, you will have a comprehensive understanding of why this number matters and how to navigate your follow-up care with confidence.
Understanding the Numbers: Is a 1.7 Creatinine Level a Cause for Concern?
Yes, a creatinine level of 1.7 mg/dL is considered elevated and is a valid reason for concern, as it suggests your kidneys are not filtering waste from your blood as efficiently as they should. However, the term "dangerous" is relative. The significance of this result depends heavily on your individual health profile. In clinical practice, nephrologists rarely interpret a single lab value in isolation. Instead, they evaluate it within the broader context of your medical history, current medications, hydration status, and concurrent laboratory findings.
Think of it as a warning light on a car's dashboard—it tells you something needs to be investigated, but it doesn't immediately tell you the full extent of the problem. A healthcare provider will interpret this value based on several factors, including:
- Age and Sex: Normal ranges differ between men and women, and kidney function naturally declines with age. As we get older, the glomerular filtration rate gradually decreases, and muscle mass changes, altering baseline creatinine production and clearance rates.
- Muscle Mass: Individuals with more muscle mass (like athletes) naturally produce more creatinine. A 1.7 might be less concerning for a bodybuilder than for a frail, elderly person. Conversely, individuals with low muscle mass may have artificially low creatinine levels, masking underlying kidney dysfunction until significant damage has already occurred.
- Baseline Level: If your creatinine has been stable around 1.4 and crept up to 1.7, it's different from it suddenly jumping from 0.8 to 1.7. A gradual increase often points toward chronic kidney disease (CKD) progression, while a rapid spike typically indicates acute kidney injury (AKI), which may be reversible with prompt treatment.
- Underlying Health Conditions: The result is more significant in individuals with diabetes, high blood pressure, or heart disease. These conditions place continuous hemodynamic stress on the renal vasculature and filtration units, making the kidneys more susceptible to functional decline.
- Hydration Status: Recent fluid intake heavily influences blood concentration. Dehydration can cause transient elevations, while overhydration might temporarily dilute serum markers.
Some experts suggest a creatinine level of 1.7 mg/dL may indicate that kidney function is at approximately 50% of its normal capacity, but this is a rough estimate. The relationship between serum creatinine and glomerular filtration rate is non-linear. When GFR drops from 100% to 50%, creatinine only rises moderately. However, once filtration capacity falls below 30%, even minor further losses cause exponential spikes in blood creatinine levels. A more precise assessment is needed, which is why additional testing and clinical correlation are mandatory.
What Is Creatinine and What Are Normal Levels?
A Byproduct of Muscle Activity
Creatinine is a chemical waste product generated from the normal wear and tear on muscles. It's a byproduct of a compound called creatine, which helps supply energy to your muscles. Specifically, creatine phosphate breaks down during muscle contraction, and creatinine is produced at a relatively steady, non-enzymatic rate proportional to an individual's total muscle mass. Your kidneys act as a sophisticated filtration system, constantly removing creatinine from your bloodstream and excreting it through urine. Because you produce creatinine at a fairly constant rate, blood levels can be a reliable indicator of how well your kidneys are performing their filtering duties.
It is important to note that dietary intake of creatine (found naturally in meat and fish) and synthetic creatine supplementation can temporarily influence serum levels. The kidneys handle this exogenous load through glomerular filtration, with minimal tubular reabsorption. Under normal physiological conditions, nearly all filtered creatinine is eliminated, making it an ideal marker for assessing renal clearance. However, because creatinine production varies between individuals, reference ranges must be tailored to demographic and physiological factors rather than applied universally.
Typical Normal Creatinine Ranges
Normal serum creatinine ranges can vary slightly between laboratories but are generally accepted as:
| Population | Normal Creatinine Range (mg/dL) |
|---|---|
| Adult Men | 0.7 to 1.3 mg/dL |
| Adult Women | 0.6 to 1.1 mg/dL |
Source: Medical News Today, Mayo Clinic
A level of 1.7 mg/dL is above the typical range for both men and women, signaling that creatinine is accumulating in the blood instead of being filtered out. It is worth noting that pediatric populations and pregnant individuals have distinct reference intervals due to differences in muscle mass, metabolic rates, and increased renal plasma volume during gestation. Laboratories often employ age- and sex-specific percentile curves to ensure accurate clinical interpretation across diverse patient demographics.
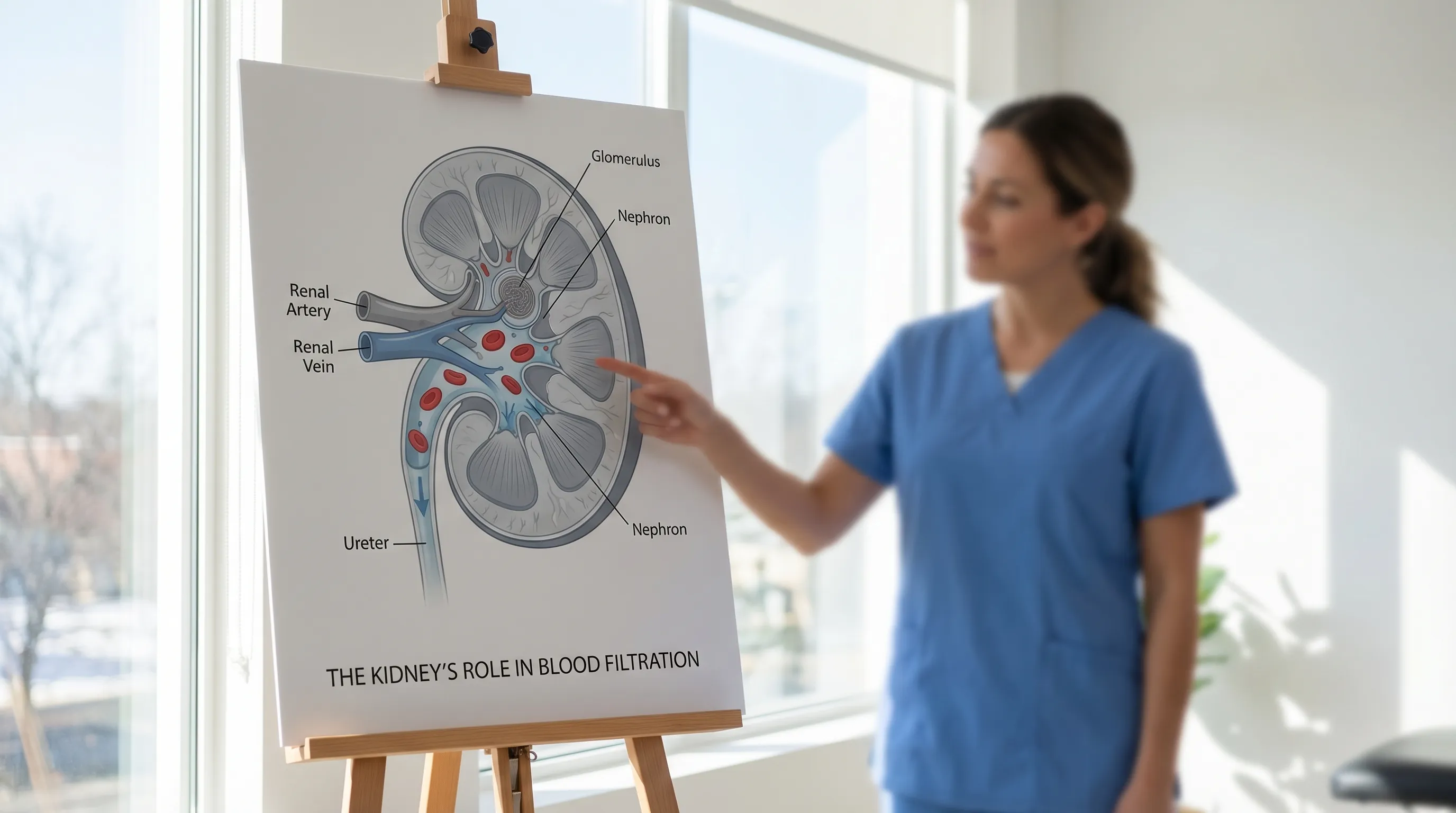 Image Source: Cleveland Clinic
Image Source: Cleveland Clinic
Why a Single Number Isn't the Whole Story: Creatinine vs. eGFR
While your creatinine level is an important clue, it's not the definitive measure of kidney health. Doctors use this number to calculate a more comprehensive value: the estimated Glomerular Filtration Rate (eGFR).
The eGFR is a calculation that estimates how much blood your kidneys filter per minute. It provides a much clearer picture of your overall kidney function. The formula uses your serum creatinine level, age, sex, and sometimes race to generate a result. Modern clinical guidelines, particularly those from the National Kidney Foundation and KDIGO (Kidney Disease: Improving Global Outcomes), have transitioned toward race-free eGFR calculations using the CKD-EPI 2021 equation to improve equity and accuracy across all populations.
Here’s why this matters: A creatinine of 1.7 mg/dL can translate to very different eGFR values and kidney disease stages for different people. For example, this level might place a younger woman in a more advanced stage of chronic kidney disease (CKD) than an older man. Your eGFR result is what doctors primarily use to diagnose and stage kidney disease.
Additionally, creatinine alone can be misleading. In patients with significant muscle wasting (sarcopenia) or advanced liver disease, creatinine production is reduced, potentially yielding a falsely reassuring normal creatinine level despite compromised kidney function. Conversely, highly muscular individuals may show elevated creatinine without actual renal impairment. To address these limitations, clinicians sometimes order a cystatin C test. Cystatin C is a protein produced by all nucleated cells at a constant rate, and it is less influenced by muscle mass, diet, or inflammation. Combining creatinine and cystatin C in a dual-marker eGFR calculation significantly improves diagnostic precision, especially when results hover in borderline zones like 1.5–1.9 mg/dL.
Potential Causes of a 1.7 Creatinine Level
An elevated creatinine level can stem from temporary, reversible issues or from more serious, chronic conditions. A medical evaluation is essential to distinguish between them. Understanding the underlying etiology is the first step toward targeted intervention, as the therapeutic approach varies dramatically depending on whether the elevation is acute, chronic, prerenal, intrarenal, or postrenal.
Temporary and Reversible Causes
In some cases, a high creatinine level can be corrected by addressing the root cause:
- Dehydration: Not drinking enough fluids concentrates waste products in your blood, temporarily raising creatinine. Reduced plasma volume decreases renal perfusion pressure, triggering the renin-angiotensin-aldosterone system (RAAS) and causing the kidneys to conserve water and sodium. This physiological adaptation reduces urine output and temporarily impairs waste clearance.
- High Protein Intake or Creatine Supplements: Consuming large amounts of protein, especially red meat, or taking creatine supplements can increase creatinine levels. Cooking meat converts dietary creatine to creatinine, which is rapidly absorbed into the bloodstream. Athletes using creatine monohydrate for performance enhancement typically experience a predictable, dose-dependent rise in serum markers without pathological kidney damage.
- Intense Exercise: Strenuous physical activity can lead to a faster breakdown of muscle, temporarily spiking creatinine. Extreme exertion, particularly resistance training or endurance events, can also cause rhabdomyolysis—a condition where severe muscle breakdown releases myoglobin into the bloodstream, potentially causing direct tubular toxicity and acute kidney injury.
- Certain Medications: Drugs like non-steroidal anti-inflammatory drugs (NSAIDs) and some antibiotics can affect kidney function. NSAIDs inhibit prostaglandin synthesis, which normally helps dilate afferent arterioles to maintain renal blood flow. Blocking this pathway reduces glomerular filtration, especially in vulnerable individuals. Other nephrotoxic agents include proton pump inhibitors (PPIs), certain antivirals, and aminoglycoside antibiotics.
- Urinary Tract Obstruction: A blockage from a kidney stone or an enlarged prostate can prevent urine from leaving the body, causing waste to back up. This postrenal mechanism increases hydrostatic pressure within the nephrons, eventually reducing net filtration pressure and impairing the kidneys' ability to clear metabolic byproducts.
Chronic and More Serious Conditions
More often, a persistently high creatinine level is linked to an underlying condition affecting the kidneys:
- Chronic Kidney Disease (CKD): Progressive and long-term damage to the kidneys. CKD is typically classified into five stages based on eGFR. A creatinine of 1.7 often corresponds to Stage 3 CKD (eGFR 30–59 mL/min), where the kidneys have lost moderate function. At this stage, complications like secondary hyperparathyroidism, metabolic acidosis, and renal anemia often emerge.
- Kidney Infection (Pyelonephritis): An infection that can damage kidney tissue if left untreated. Bacterial ascension from the lower urinary tract to the renal pelvis causes inflammation, scarring, and permanent loss of functional nephrons if treatment is delayed.
- Glomerulonephritis: Inflammation of the kidneys' tiny filters (glomeruli). This can be primary or secondary to autoimmune disorders like lupus, IgA nephropathy, or ANCA-associated vasculitis. Immune complex deposition damages the glomerular basement membrane, leading to proteinuria, hematuria, and declining filtration capacity.
- Unmanaged Diabetes: High blood sugar can damage blood vessels in the kidneys over time. Diabetic nephropathy begins with glomerular hyperfiltration, progresses to thickening of the basement membrane and mesangial expansion, and eventually leads to glomerulosclerosis and declining eGFR. It remains the leading cause of end-stage renal disease worldwide.
- High Blood Pressure (Hypertension): Uncontrolled high blood pressure can damage the arteries leading to the kidneys. Chronic hypertension causes arteriolar hyalinosis and nephrosclerosis, reducing blood supply to the renal parenchyma. The kidneys, in turn, struggle to regulate blood pressure, creating a vicious cycle of progressive renal and cardiovascular damage.
- Heart Disease: Conditions like congestive heart failure can reduce blood flow to the kidneys. Cardiorenal syndrome describes the bidirectional relationship where heart failure compromises renal perfusion, and kidney dysfunction exacerbates fluid overload and cardiac stress. Elevated creatinine in this context often reflects venous congestion rather than primary renal pathology.
Symptoms Associated with High Creatinine
In the early stages of kidney dysfunction, you might not notice any symptoms. The kidneys possess a remarkable functional reserve, meaning patients often remain asymptomatic until filtration capacity drops below 50%. However, as creatinine levels rise and kidney function declines, toxins accumulate, electrolytes become imbalanced, and hormonal regulation falters. You may experience:
- Fatigue and weakness: Resulting from decreased erythropoietin production by the kidneys, leading to anemia, and from the buildup of uremic toxins that disrupt cellular metabolism and neurological function.
- Swelling (edema) in the legs, feet, ankles, or around the eyes: Caused by the kidneys' inability to excrete excess sodium and fluid, leading to intravascular volume expansion and leakage into interstitial tissues.
- Changes in urination, such as urinating more or less often, or having foamy or dark-colored urine: Foamy urine indicates proteinuria (albumin leakage through damaged glomeruli), while dark or bloody urine may signal glomerular inflammation or structural damage.
- Shortness of breath: Arising from pulmonary edema due to fluid overload, metabolic acidosis causing compensatory hyperventilation, or anemia reducing oxygen-carrying capacity.
- Nausea and vomiting: Common in advancing uremia as nitrogenous waste products irritate the gastrointestinal lining and alter central nervous system signaling pathways responsible for appetite and digestion.
- Loss of appetite: Mediated by uremic toxins, altered taste perception (dysgeusia), and hormonal dysregulation, often leading to malnutrition and muscle wasting over time.
- Muscle cramps: Triggered by electrolyte imbalances, particularly low calcium, high phosphorus, or abnormal potassium levels, combined with fluid shifts and peripheral neuropathy.
- Dry, itchy skin: Known as uremic pruritus, caused by mineral and bone disorders, calcium-phosphorus precipitation in the skin, dryness, and systemic inflammation.
- Confusion or difficulty concentrating: Resulting from the neurotoxic effects of accumulated uremic solutes, altered neurotransmitter metabolism, and reduced cerebral oxygenation secondary to anemia or fluid imbalances.
When to Seek Immediate Medical Attention
While any elevated creatinine level requires a doctor's visit, certain symptoms alongside it signal a medical emergency, possibly indicating acute kidney injury. Seek immediate care if you experience:
- A sudden and significant decrease in urine output (anuria or oliguria), which may indicate severe obstruction, profound hypoperfusion, or rapid nephron failure.
- Severe swelling that develops rapidly, especially if accompanied by weight gain of more than 2–3 pounds per day, suggesting acute fluid retention that can strain the cardiovascular system.
- Difficulty breathing or chest pain, which could indicate fluid accumulation in the lungs (pulmonary edema), pericardial effusion, or hyperkalemia-induced arrhythmias.
- Confusion or an altered mental state, potentially signaling uremic encephalopathy, severe electrolyte disturbances, or sepsis.
- Palpitations or irregular heart rhythms, often caused by dangerously high potassium levels (hyperkalemia), a life-threatening complication of impaired renal excretion.
- Unexplained severe back or flank pain, particularly if accompanied by fever, which may suggest acute pyelonephritis or a obstructing kidney stone requiring urgent intervention.
Diagnosis and Next Steps: What to Expect from Your Doctor
If your blood test shows a creatinine level of 1.7, do not panic. Your doctor will begin a thorough investigation to understand the cause. Modern diagnostic pathways are highly structured, aiming to differentiate acute from chronic disease, identify reversible contributors, and establish a baseline for monitoring. You can expect the following steps:
- Medical History Review: Your doctor will ask about your diet, medications, supplements, and any existing health conditions like diabetes or hypertension. They will also inquire about recent illnesses, fluid intake, urinary symptoms, family history of kidney disease, and occupational or environmental exposures that could impact renal function.
- Follow-Up Tests: Additional tests will likely be ordered to get a complete picture of your kidney health. These may include:
- Repeat Creatinine Test and eGFR Calculation: To confirm the initial result and assess trend over days or weeks. A single abnormal value is insufficient for diagnosis; persistence or progression is required.
- Blood Urea Nitrogen (BUN): Another waste product that can indicate kidney issues. The BUN-to-creatinine ratio helps differentiate prerenal causes (e.g., dehydration, ratio >20:1) from intrinsic renal damage (ratio 10–15:1).
- Urinalysis and Albumin-to-Creatinine Ratio (ACR): To check for protein (albumin) or blood in your urine, which are early markers of glomerular damage. Microalbuminuria often appears years before serum creatinine rises, making it a critical early screening tool.
- Kidney Ultrasound: An imaging test to look for structural abnormalities, cysts, stones, hydronephrosis, or differences in kidney size. Small, echogenic kidneys typically indicate chronic scarring, while normal or enlarged kidneys suggest acute or infiltrative processes.
- Electrolyte Panel: To check the balance of sodium, potassium, chloride, bicarbonate, calcium, phosphorus, and magnesium in your blood. Kidneys play a central role in maintaining these homeostatic parameters.
- Cystatin C Testing: If creatinine is deemed unreliable due to muscle mass extremes or dietary factors, cystatin C provides a complementary filtration estimate.
- Specialist Referral: Depending on the findings, your primary care provider may refer you to a nephrologist. Nephrologists specialize in managing complex electrolyte disorders, progressive CKD, glomerular diseases, and preparing patients for renal replacement therapies if necessary.
Managing and Treating High Creatinine Levels
Treatment for a high creatinine level focuses entirely on addressing its underlying cause. There is no single medication that directly "lowers creatinine"; rather, therapy targets the physiological pathways responsible for impaired filtration or elevated production. Early intervention can stabilize kidney function, prevent complications, and significantly delay the need for dialysis or transplantation.
Medical Treatments
Based on your diagnosis, your doctor may recommend:
- Managing Blood Pressure or Diabetes: Prescribing medications like ACE inhibitors (e.g., lisinopril) or ARBs (e.g., losartan) to protect the kidneys. These drugs reduce intraglomerular pressure, decrease proteinuria, and slow fibrotic remodeling of renal tissue. For diabetes, SGLT2 inhibitors (e.g., empagliflozin) and GLP-1 receptor agonists have revolutionized care by demonstrating robust cardio-renal protective benefits independent of glycemic control.
- Treating Infections: Using antibiotics for a kidney infection. Prompt, culture-directed antimicrobial therapy prevents permanent parenchymal scarring and preserves functional nephron mass.
- Adjusting Medications: Stopping or changing any drugs that may be harming your kidneys. Pharmacists and physicians will review nephrotoxic agents, adjust dosages based on current eGFR, and substitute safer alternatives when available.
- Correcting Electrolyte Imbalances: Administering potassium-lowering agents (like patiromer or sodium polystyrene sulfonate) or bicarbonate supplementation for metabolic acidosis, both of which are common in moderate CKD.
- Advanced Treatments: In cases of severe kidney failure, treatments like dialysis (filtering the blood mechanically) or a kidney transplant may be necessary. Hemodialysis, peritoneal dialysis, and preemptive transplantation are carefully coordinated based on vascular access readiness, comorbidities, and patient preference.
Lifestyle and Dietary Adjustments
Lifestyle changes are crucial for supporting kidney function and can help manage creatinine levels:
- Stay Hydrated: Drink plenty of water throughout the day unless your doctor advises otherwise. Adequate fluid intake maintains renal perfusion, prevents crystallization of minerals that cause stones, and supports optimal urine concentration. However, patients with advanced fluid retention or heart failure must adhere to strict fluid restrictions to avoid volume overload.
- Discuss Protein Intake: Your doctor or a dietitian may recommend limiting protein consumption to reduce the workload on your kidneys. For non-dialysis CKD patients, current guidelines suggest 0.55–0.60 g/kg/day of high-biological-value protein to minimize nitrogenous waste accumulation while preventing malnutrition. Plant-based proteins are increasingly favored due to their lower acid load and beneficial fiber content.
- Reduce Sodium: A low-sodium diet helps control blood pressure and fluid balance. Aim for less than 2,300 mg daily, or 1,500 mg if you have hypertension or edema. Reading nutrition labels, avoiding processed foods, and cooking with herbs instead of salt can dramatically improve renal hemodynamics.
- Manage Potassium and Phosphorus: As kidney function declines, the body struggles to excrete these minerals. Limiting high-potassium foods (bananas, oranges, potatoes, tomatoes) and high-phosphorus items (dairy, dark colas, processed meats with phosphate additives) prevents cardiac arrhythmias and bone demineralization.
- Avoid NSAIDs: Limit the use of over-the-counter pain relievers like ibuprofen and naproxen. For pain management, acetaminophen is generally safer for renal patients when used within recommended dosage limits. Always consult your physician before starting new supplements or herbal remedies, as many lack safety data and may interact with prescriptions.
- Exercise Moderately: Regular, moderate exercise is beneficial, but avoid overly intense workouts. Physical activity improves cardiovascular health, insulin sensitivity, and blood pressure control. Focus on low-impact activities like walking, swimming, cycling, or yoga, and always warm up adequately to prevent muscle breakdown that could temporarily elevate creatinine.
- Quit Smoking and Limit Alcohol: Smoking accelerates renal vascular damage and reduces blood flow to the glomeruli. Excessive alcohol consumption can lead to dehydration, hypertension, and liver disease, all of which indirectly impair renal clearance.
Conclusion: Taking Proactive Steps for Your Kidney Health
A creatinine level of 1.7 mg/dL is a significant health signal that should be taken seriously. It is a call to action, prompting a conversation with your healthcare provider to investigate the cause and protect your long-term kidney health. While the result can be caused by temporary factors like dehydration, dietary shifts, or intense exercise, it can also be the first measurable sign of a chronic condition requiring structured management. The modern approach to kidney care is highly proactive, emphasizing early detection, precise staging, and multidisciplinary intervention.
The kidneys operate silently until their functional reserve is significantly depleted, which makes routine monitoring essential, particularly for individuals with diabetes, hypertension, obesity, or a family history of renal disease. Early diagnosis and proactive management are your best tools for preventing further kidney damage and maintaining your overall well-being. By partnering with your healthcare team, adhering to prescribed therapies, implementing sustainable lifestyle modifications, and staying informed about your lab trends, you can effectively navigate this finding. Remember that a single elevated creatinine value does not define your future health trajectory. With timely evaluation and consistent care, many individuals stabilize their kidney function, minimize symptoms, and continue living active, fulfilling lives.
Frequently Asked Questions
Can dehydration alone cause a creatinine level of 1.7?
Yes, significant dehydration is a common and reversible cause of transient creatinine elevation. When you lose fluids through sweating, vomiting, diarrhea, or insufficient water intake, blood volume decreases and renal perfusion drops. The kidneys respond by conserving water and reducing urine output, which concentrates waste products in the bloodstream. This prerenal state typically causes a disproportionate rise in BUN compared to creatinine. Rehydrating under medical guidance usually normalizes levels within days, though severe or prolonged dehydration can occasionally trigger acute tubular injury.
Should I stop taking creatine supplements if my level is 1.7?
If you use creatine monohydrate, it is advisable to pause supplementation temporarily and discuss your lab results with a healthcare provider. Creatine breaks down into creatinine, so supplement use will predictably raise serum creatinine without necessarily indicating kidney damage. Your physician may recommend discontinuing it for two to four weeks, repeating the test, and possibly ordering a cystatin C test to obtain a filtration estimate unaffected by muscle metabolism or exogenous creatine intake. Never stop or start supplements without professional guidance, especially if you have underlying health conditions.
How long does it take for creatinine levels to return to normal after an acute kidney injury?
The recovery timeline varies widely depending on the cause, severity, and your baseline health. In mild, reversible cases like medication-induced injury or dehydration, creatinine often begins declining within a few days of intervention and may normalize within one to three weeks. More severe acute kidney injuries, particularly those requiring hospitalization, dialysis, or involving prolonged ischemia, can take months to stabilize. Some patients experience partial recovery, leaving them with a lower baseline kidney function than before the event. Serial monitoring and strict adherence to renal-protective strategies are essential during the recovery phase.
Does having a creatinine level of 1.7 automatically mean I need dialysis?
No, a creatinine level of 1.7 mg/dL does not automatically indicate a need for dialysis. Dialysis is generally initiated when kidney function declines to end-stage renal disease (eGFR typically below 15 mL/min) or when life-threatening complications arise, such as severe fluid overload, refractory hyperkalemia, uremic encephalopathy, or pericarditis. A creatinine of 1.7 usually corresponds to moderate (Stage 3) chronic kidney disease or a reversible acute process. The goal at this stage is aggressive medical management and lifestyle modification to preserve remaining kidney function and delay progression, often for many years.
What dietary changes are most effective for managing a 1.7 creatinine level?
The most effective dietary approach focuses on reducing sodium, moderating high-quality protein, managing potassium and phosphorus intake, and emphasizing whole, plant-forward foods. A registered dietitian specializing in renal nutrition can create a personalized plan based on your eGFR, electrolyte levels, and comorbidities. Generally, adopting a DASH-style or Mediterranean-inspired diet low in processed foods, added sugars, and saturated fats supports blood pressure control and reduces systemic inflammation. Staying consistently hydrated with water, reading food labels meticulously, and avoiding crash diets or extreme fasting will help stabilize metabolic waste production and support overall kidney health.
About the author
Carlos Ruiz, MD, FACS, is a board-certified urologist specializing in minimally invasive and robotic surgery for urologic cancers. He is a senior partner at a large urology group in Houston, Texas, and is involved in clinical trials for new prostate cancer treatments.