Itchy on Roof of Mouth: Causes, Evidence-Based Relief, and Prevention

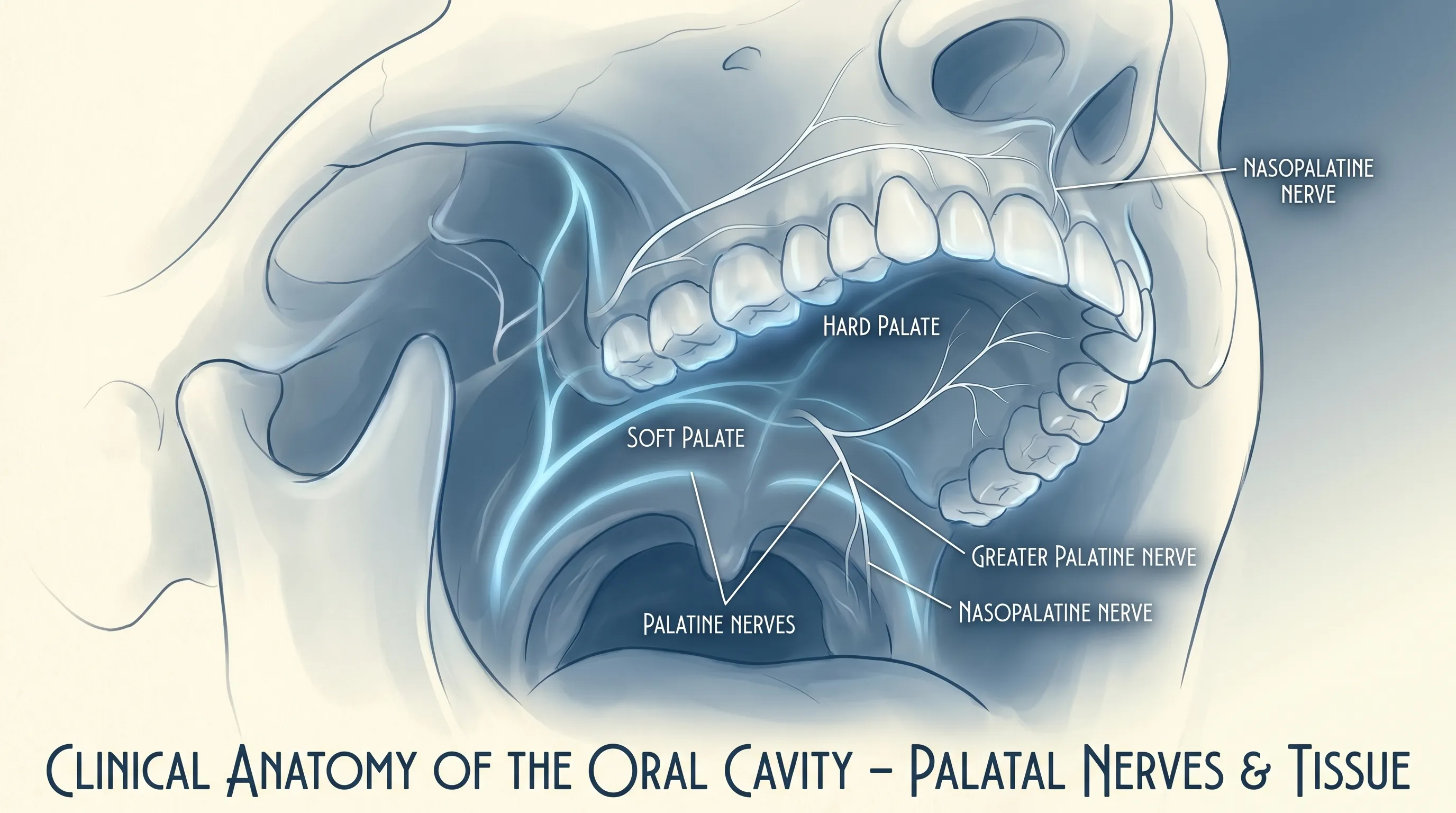
That familiar, relentless tickle right behind your front teeth can be incredibly distracting and deeply uncomfortable. When you find yourself constantly pressing your tongue against an itchy on roof of mouth sensation, it is easy to wonder whether it is just a minor irritation or the beginning of a more serious physiological response. This specific type of oral discomfort affects millions of people worldwide, yet it frequently remains undiscussed in mainstream clinical conversations. The hard and soft palate is densely packed with sensory nerve endings and highly vascularized tissue, making it exceptionally reactive to environmental shifts, dietary compounds, microbial imbalances, and immune-mediated signaling pathways. Understanding why this occurs and how to address it effectively requires a thorough examination of both localized tissue physiology and systemic inflammatory triggers. In this comprehensive guide, we will explore the clinical root causes, differentiate between temporary sensory annoyances and chronic immunological patterns, and provide you with actionable, evidence-based strategies to achieve lasting oral comfort. Whether your symptoms appear seasonally, emerge after specific meals, or develop completely without warning, this resource will equip you with scientifically grounded insights and practical management techniques.
Understanding Oral Pruritus: What Causes an Itchy Roof of Mouth?
The clinical term for localized itching in the oral cavity is oral pruritus, a symptom rather than a standalone disease. When patients report feeling an itchy on roof of mouth, they are describing a complex neuroimmune event. The palatal mucosa contains specialized nerve fibers called C-fibers and A-delta fibers that transmit pruritic signals to the brainstem. Under normal conditions, these fibers remain dormant. However, exposure to certain allergens, temperature extremes, or inflammatory mediators triggers the release of histamine, bradykinin, and leukotrienes from mast cells and basophils embedded in the palatal tissue. These chemicals bind to H1 and H4 receptors on sensory nerves, generating the characteristic tickling or burning sensation that many describe as relentless and deeply uncomfortable.
The Role of Mast Cells and Histamine Release
Mast cells are resident immune sentinels located throughout mucosal surfaces, particularly concentrated in the nasopharyngeal and palatal regions. When they encounter an unrecognized protein or chemical compound, they rapidly degranulate, releasing stored histamine and synthesizing new inflammatory mediators. This cascade increases local blood flow, induces mild tissue edema, and directly stimulates peripheral itch receptors. For many individuals, the sensation of an itchy on roof of mouth is simply the clinical manifestation of localized mast cell activation. Research published by the National Institute of Allergy and Infectious Diseases demonstrates that even subclinical allergen exposure can trigger measurable histamine spikes in palatal tissue, explaining why some people experience persistent mild itching without obvious hives or respiratory symptoms. Understanding this biological pathway is essential, as it clarifies why antihistamines often provide rapid relief while structural interventions like dental adjustments rarely address the underlying mechanism.
Oral Allergy Syndrome and Pollen-Food Cross-Reactivity
One of the most prevalent drivers of palatal pruritus is oral allergy syndrome (OAS), a condition that occurs when the immune system mistakenly identifies certain raw plant proteins as identical to environmental pollen allergens. This phenomenon, known as pollen-food syndrome, arises because the molecular structures of proteins like Bet v 1 (birch pollen), Profilin (grass), or Lipid Transfer Proteins (ragweed) share high homology with proteins found in common fruits, vegetables, and nuts. When consumed raw, these proteins survive the initial digestive phase and bind to IgE antibodies already present on palatal mast cells. The result is an almost immediate onset of localized itching, mild swelling, or tingling sensations concentrated on the roof of the mouth, lips, and posterior tongue. Studies indicate that up to seventy percent of individuals with seasonal hay fever will develop some degree of OAS, making it a leading clinical explanation for recurrent oral pruritus. Notably, cooking or microwaving these foods denatures the labile proteins, which is why many patients report zero discomfort when consuming the same items in processed form.
Infections, Microbial Shifts, and Inflammatory Conditions
Beyond allergic mechanisms, localized infections and dysbiosis within the oral microbiome can directly trigger palatal itching. Candidiasis, commonly referred to as oral thrush, frequently presents with a persistent scratchy or tickling sensation across the hard palate before progressing to visible white plaques or erythema. The overgrowth of Candida species alters local pH levels and stimulates epithelial Toll-like receptors, prompting inflammatory cytokine release that mimics histamine-driven pruritus. Similarly, early-stage viral infections like herpangina or coxsackievirus can begin with subtle palatal irritation days before vesicle formation. Dental professionals also note that poorly fitted orthodontic appliances, rough dental restorations, or chronic mouth breathing can cause micro-abrasions and mucosal dryness. When the protective salivary layer is compromised, nerve endings become hypersensitive to normal dietary acids, temperature fluctuations, and even ambient air flow, generating a false itch response that feels identical to allergic reactions.
Identifying Triggers and Risk Factors
Pinpointing the exact trigger behind an itchy on roof of mouth requires systematic observation and occasionally, professional diagnostic testing. Because the symptom overlaps with multiple physiological systems, a structured approach to trigger identification prevents unnecessary lifestyle restrictions while ensuring genuine allergens are properly managed. Clinical allergy guidelines emphasize the importance of maintaining a detailed symptom journal that tracks environmental exposure, dietary intake, medication changes, and symptom onset timing. This data often reveals patterns that would otherwise remain hidden, allowing patients and practitioners to isolate specific culprits rather than treating vague generalized discomfort.
Seasonal Pollen and Environmental Allergens
Environmental allergens represent the most common external triggers for palatal pruritus. During spring, tree pollen concentrations peak, heavily sensitizing individuals with birch or oak allergies. Summer months introduce grass pollen, while late summer and early fall see dramatic increases in weed pollen, particularly ragweed. These microscopic particles travel easily into the oral cavity during normal breathing, mouth talking, or light chewing. Once deposited on the palatal mucosa, they interact with pre-sensitized IgE antibodies, initiating the familiar tickling sensation. Airborne particulate matter, indoor mold spores, and dust mite debris can produce identical responses, especially in individuals with preexisting allergic rhinitis or asthma. Research from the American College of Allergy, Asthma & Immunology confirms that localized oral symptoms often precede nasal congestion by several days, making palate itching an early warning sign of seasonal allergen exposure.
Food Intolerances and Chemical Sensitivities
While true IgE-mediated food allergies dominate clinical discussions, non-allergic food intolerances and chemical sensitivities frequently masquerade as oral pruritus. Sulfites, commonly found in dried fruits, wine, and processed potatoes, can trigger mast cell degranulation in sensitive individuals, resulting in rapid-onset palatal itching. Monosodium glutamate and certain artificial colorants may also provoke localized neurogenic inflammation, particularly in patients with heightened sensory processing. Additionally, highly acidic foods like citrus fruits, tomatoes, and vinegar-based condiments can temporarily lower mucosal pH, irritating compromised epithelial tissue and creating a scratchy, uncomfortable sensation that many interpret as itching. Distinguishing between immune-mediated reactions and chemical irritation is crucial, as their management pathways differ significantly. Elimination diets supervised by a registered dietitian remain the gold standard for identifying non-allergic food triggers.
Medications and Hormonal Fluctuations
Pharmacological agents and endocrine shifts can indirectly provoke palatal itching through systemic pathways. Angiotensin-converting enzyme inhibitors, commonly prescribed for hypertension, are well-documented to cause persistent dry cough and mucosal irritation due to bradykinin accumulation. Certain antidepressants and antihistamines paradoxically reduce salivary output, leading to xerostomia-related palatal discomfort that closely mimics true pruritus. Hormonal fluctuations during pregnancy, menopause, or menstrual cycles also alter mucosal blood flow and tissue elasticity. Estrogen withdrawal reduces collagen synthesis in oral epithelium, making the palate more susceptible to micro-tears and nerve hyperreactivity. Women frequently report heightened oral sensitivity during luteal phases, a pattern supported by gynecological immunology research linking progesterone and estrogen ratios to localized inflammatory thresholds. Recognizing these systemic contributors ensures that treatment targets the root cause rather than merely masking surface symptoms.
Immediate Relief Strategies You Can Use at Home
When discomfort strikes unexpectedly, having a repertoire of evidence-based home interventions can significantly reduce symptom duration and intensity. The goal of immediate relief is to stabilize local mast cells, wash away irritants, soothe exposed nerve endings, and restore optimal mucosal hydration. These strategies should complement, not replace, professional medical evaluation, but they provide highly effective symptomatic control while awaiting clinical appointments.
Cold Therapy and Controlled Hydration
Temperature modulation remains one of the most reliable methods for interrupting the itch cycle. Applying cold to the palatal region causes localized vasoconstriction, which reduces blood flow to inflamed tissue and temporarily decreases nerve conduction velocity. This physiological response directly dampens the transmission of pruritic signals to the central nervous system. Simple interventions include sucking on ice chips, consuming chilled water slowly, or applying a cool compress to the external upper lip area for two-minute intervals. Avoid placing solid ice directly against the palate for extended periods, as thermal shock can cause epithelial damage and worsen sensitivity. Consistent, moderate hydration also supports salivary gland function, maintaining the protective mucous layer that naturally buffers allergens and prevents nerve exposure.
Saline Rinses and Soothing Natural Agents
Isotonic saline rinses effectively clear allergen particles, residual food proteins, and inflammatory debris from the oral cavity without disrupting natural tissue pH. Preparing a solution with one-half teaspoon of non-iodized salt dissolved in eight ounces of warm filtered water, then gently gargling and allowing it to pool on the palate for thirty seconds before spitting, can provide immediate mechanical cleansing. For additional mucosal support, adding a quarter teaspoon of baking soda enhances buffering capacity against dietary acids. Natural demulcents like pure aloe vera juice, marshmallow root extract, or slippery elm preparations coat irritated tissue, creating a temporary protective barrier that reduces friction and soothes exposed nerve endings. Clinical dermatology studies consistently rank mucosal coating agents among the safest and most effective immediate interventions for localized oral irritation.
Over-the-Counter Antihistamines and Topical Solutions
When home remedies provide insufficient relief, second-generation oral antihistamines remain the clinical standard for rapid histamine receptor blockade. Medications containing cetirizine, loratadine, or fexofenade demonstrate high specificity for H1 receptors, effectively halting the itch cascade with minimal sedation compared to older formulations. Liquid suspensions often provide faster onset than tablets, making them ideal for acute symptom management. Topical oral analgesic gels containing benzocaine or lidocaine can temporarily numb palatal tissue, but they should be used sparingly due to the risk of masking more serious inflammatory progression or triggering localized hypersensitivity. Always follow package dosing instructions and consult a pharmacist before combining antihistamines with other medications to avoid adverse interactions.
Long-Term Management and Prevention Techniques
Sustainable symptom control requires moving beyond reactive treatment toward proactive physiological management. Long-term strategies focus on reducing systemic inflammatory burden, rebuilding mucosal resilience, and identifying personal trigger thresholds through structured lifestyle adjustments. Patients who implement comprehensive prevention protocols typically experience significant reductions in symptom frequency and severity within three to six months.
Dietary Modifications and Elimination Protocols
Strategic dietary adjustments form the cornerstone of long-term oral pruritus management. Identifying and eliminating confirmed cross-reactive foods prevents repeated mast cell activation, allowing palatal tissue to heal and recalibrate sensitivity levels. Patients benefit from adopting a low-inflammatory nutritional framework emphasizing omega-3 rich fish, leafy greens, fermented vegetables, and whole grains while minimizing refined sugars, processed seed oils, and excessive alcohol consumption. Fermented foods like kefir, sauerkraut, and kimchi introduce beneficial probiotic strains that modulate gut-immune crosstalk, indirectly stabilizing oral mucosal immunity. For those struggling to identify specific triggers, a structured four-to-six week elimination diet supervised by a healthcare professional provides definitive clarity. Systematic reintroduction of foods every three days allows clear symptom tracking without triggering chronic flare-ups.
Professional Allergy Testing and Immunotherapy
When symptoms persist despite conservative management, formal allergy testing becomes essential. Skin prick tests and serum-specific IgE blood panels accurately identify environmental and dietary sensitivities, guiding targeted avoidance strategies. Component-resolved diagnostics now allow clinicians to distinguish between true food allergies and benign cross-reactivity, preventing unnecessary dietary restrictions. For patients with severe seasonal or multi-allergen profiles, sublingual immunotherapy drops or tablets offer disease-modifying benefits. Unlike antihistamines that merely suppress symptoms, immunotherapy gradually retrains the immune system to tolerate previously problematic proteins. Clinical trials published in leading allergy journals demonstrate sustained symptom reduction in over seventy percent of participants after one to three years of consistent use. This approach addresses the underlying immunological dysfunction rather than managing surface discomfort.
Oral Care Routines and Microbiome Support
Daily oral hygiene practices significantly influence palatal tissue health. Brushing twice daily with a soft-bristled brush, using fluoride-free or low-SLS toothpaste for sensitive individuals, and flossing consistently prevent secondary bacterial irritation that compounds allergic discomfort. Alcohol-based mouthwashes should be avoided, as they rapidly desiccate mucosal surfaces and strip protective lipid layers. Instead, opt for xylitol-enhanced rinses or neutral pH formulations that maintain microbial balance. Regular dental check-ups allow early detection of occult infections, periodontal inflammation, or structural irritants that may contribute to chronic palatal sensitivity. Supporting systemic vitamin D and zinc levels through sunlight exposure or targeted supplementation also strengthens epithelial integrity and reduces baseline inflammatory markers, creating a resilient oral environment less prone to reactive itching.
| Trigger Category | Common Sources | Primary Mechanism | Recommended Management | Expected Onset | Duration Without Treatment |
|---|---|---|---|---|---|
| Pollen-Food Cross-Reactivity | Raw apples, stone fruits, celery, melons | IgE-mediated mast cell degranulation via shared protein structures | Avoid raw forms, cook foods, use second-gen antihistamines | 2–15 minutes | 1–3 hours post-exposure |
| Seasonal Environmental Allergens | Birch, grass, ragweed pollen, indoor mold | Airborne allergen deposition on palatal mucosa | HEPA air filtration, saline rinses, daily nasal corticosteroids | 30 minutes–2 hours | Days during peak season |
| Chemical Sensitivities | Sulfites, MSG, artificial dyes, high-acid foods | Direct mast cell activation or pH-induced nerve irritation | Read ingredient labels, switch to whole foods, buffer acidity | 10–45 minutes | 4–12 hours |
| Oral Microbial Overgrowth | Candida species, oral thrush precursors | Toll-like receptor activation and cytokine release | Probiotic support, antifungal rinses, reduced refined sugars | Gradual, 2–5 days | Weeks until microbiome rebalanced |

When to Consult a Healthcare Provider
While most cases of palatal itching resolve with conservative measures, certain clinical presentations warrant professional evaluation to rule out underlying pathology or prevent symptom progression. Recognizing the boundary between self-managed comfort and medically necessary intervention protects long-term health and prevents complications from delayed diagnosis.
Red Flag Symptoms Requiring Immediate Attention
Patients should seek urgent medical care if palatal itching is accompanied by lip or tongue swelling, voice changes, wheezing, difficulty swallowing, gastrointestinal cramping, dizziness, or widespread urticaria. These systemic indicators suggest an evolving anaphylactic cascade or severe angioedema that requires immediate epinephrine administration and emergency department evaluation. Additionally, persistent palatal ulcers, white patches that cannot be gently wiped away, unexplained bleeding, or numbness warrant prompt dental or otolaryngology assessment to exclude dysplastic changes, viral infections, or neurological involvement. Early intervention dramatically improves outcomes and prevents avoidable tissue damage.
Diagnostic Procedures and Clinical Pathways
Healthcare providers typically begin with a comprehensive medical history and targeted physical examination of the oral cavity, nasal passages, and oropharynx. When allergic etiology is suspected, referral for comprehensive allergy panel testing clarifies specific IgE reactivity patterns. For chronic or atypical cases, providers may order salivary flow measurements, microbial cultures, or blood work to assess thyroid function, vitamin deficiencies, and autoimmune markers. In rare instances, a minor palatal biopsy may be recommended to rule out lichen planus, pemphigus vulgaris, or other mucocutaneous disorders. Understanding the diagnostic roadmap empowers patients to actively participate in care decisions, ask informed questions, and adhere to prescribed treatment timelines.
Specialized Treatment Pathways
Depending on confirmed etiology, specialists may prescribe targeted therapies beyond standard antihistamines. Intranasal corticosteroids reduce upper airway inflammation that frequently exacerbates palatal reactivity. Leukotriene receptor antagonists like montelukast address secondary inflammatory pathways particularly useful for patients with overlapping asthma and oral allergy symptoms. For confirmed candidal involvement, short-course nystatin or fluconazole prescriptions rapidly restore mucosal equilibrium. Patients with refractory cases may benefit from referral to an allergist-immunologist for advanced desensitization protocols, biologics, or mast cell stabilizer therapy. Collaborative care between primary physicians, dental professionals, and immunology specialists ensures comprehensive symptom resolution.
Frequently Asked Questions
Why does my palate itch only during allergy season?
Seasonal pollen triggers an IgE-mediated immune response that releases histamine in oral tissues. The roof of your mouth contains dense mast cell populations that react to airborne allergens like birch, ragweed, or grass pollen. When these cells degranulate, nerve endings in the hard and soft palate fire, creating localized pruritus that typically peaks during high pollen counts. Maintaining a daily antihistamine regimen and using nasal saline irrigation during peak seasons significantly reduces cross-reactive oral symptoms by limiting allergen deposition.
Can an itchy roof of the mouth indicate a serious allergic reaction?
While most cases are mild oral allergy syndrome or localized irritation, persistent or worsening itchiness accompanied by throat swelling, difficulty breathing, hives, or dizziness can signal anaphylaxis. Immediate medical evaluation is required if systemic symptoms develop, as delayed treatment can become life-threatening. Patients with known severe allergies should always carry prescribed epinephrine auto-injectors and review emergency action plans with their allergist before allergy seasons begin.
What foods commonly cause cross-reactive mouth itching?
Patients allergic to birch pollen often experience itching after eating raw apples, stone fruits, carrots, celery, and hazelnuts due to shared Bet v 1 proteins. Ragweed cross-reactivity typically involves bananas, melons, cucumbers, and zucchini. Heat generally denatures these proteins, which is why cooked versions rarely trigger symptoms. Processing methods like peeling, blending, or fermenting also reduce protein load, allowing many individuals to tolerate modified versions without experiencing an itchy on roof of mouth sensation.
How long does it take for an itchy palate to resolve naturally?
If triggered by mild environmental exposure or temporary dietary cross-reactivity, the sensation typically resolves within thirty minutes to a few hours once the allergen is cleared. Chronic cases related to persistent allergic rhinitis, untreated oral candidiasis, or dry mouth syndrome may last days or weeks without targeted treatment. Implementing consistent hydration, mucosal barrier support, and trigger avoidance accelerates tissue recovery and prevents recurrent inflammatory cycling.
Are there specific vitamins or supplements that reduce oral itching?
Quercetin-rich foods, omega-3 fatty acids, and vitamin C demonstrate natural mast cell-stabilizing properties in clinical studies. Bromelain from pineapples may reduce localized inflammation, while zinc and vitamin D support immune regulation. Always consult a healthcare provider before starting supplements, especially if taking antihistamines, anticoagulants, or immunomodulators, as certain botanicals can interact with prescription medications or alter diagnostic test results.
Conclusion
Experiencing an itchy on roof of mouth is far more than a fleeting annoyance; it is your body's sophisticated signaling system requesting attention. By understanding the neuroimmunological pathways behind palatal pruritus, recognizing environmental and dietary triggers, and implementing structured relief protocols, you can effectively manage discomfort while protecting long-term oral health. Immediate home strategies like cold therapy, saline rinses, and appropriate antihistamines provide rapid symptom control, while long-term approaches including dietary modifications, microbiome support, and professional allergy testing address the underlying physiological drivers. Always remain vigilant for systemic warning signs that require urgent clinical intervention, and partner with qualified healthcare providers to develop a personalized management plan. With consistent implementation of evidence-based practices, most individuals achieve lasting relief and restore comfortable, resilient oral tissue. Prioritize proactive care, honor your body's signals, and maintain open communication with your medical team to ensure optimal wellness across all seasons.
For additional verified medical guidance on allergy management and oral health, visit the National Institute of Allergy and Infectious Diseases or review clinical resources at the American College of Allergy, Asthma & Immunology. The Mayo Clinic also provides comprehensive patient education materials on oral allergy syndrome and symptom tracking protocols.

About the author
Benjamin Carter, MD, is a board-certified otolaryngologist specializing in head and neck surgery, with an expertise in treating throat cancer. He is an associate professor and the residency program director at a medical school in North Carolina.