Is Stage 4 Cancer Terminal? A Comprehensive Look at Prognosis and Hope

Key points
- Incurable but Treatable: This describes a condition that cannot be completely eradicated but can be managed with ongoing therapy. The goals of treatment are to control the disease, slow its progression, shrink tumors, and extend survival while maintaining a good quality of life. Many Stage 4 cancers now fall into this category.
- Terminal: A disease is considered terminal when it no longer responds to curative or life-extending treatments. At this point, the focus of medical care shifts from controlling the cancer to providing comfort, known as palliative or end-of-life care.
A diagnosis of Stage 4 cancer is a life-altering event, filled with uncertainty and fear. The first question that often comes to mind is a heavy one: "Is it terminal?" While Stage 4 represents the most advanced phase of the disease, the answer is no longer a simple "yes." Thanks to remarkable medical advancements, the landscape is shifting from a universally terminal prognosis to one where many advanced cancers can be treated and managed as chronic illnesses, extending both the length and quality of life.
This article will provide a comprehensive, expert-backed look into what a Stage 4 diagnosis means today, moving beyond the statistics to explore the realities of treatment, the importance of personalized care, and the very real reasons for hope.
In the modern era of oncology, the initial shock of a metastatic diagnosis is frequently followed by a period of complex decision-making. Patients and families must quickly learn to navigate a new medical vocabulary, understand evolving treatment paradigms, and build a support network that includes not only oncologists but also specialized nurses, dietitians, mental health professionals, and palliative care experts. This multidisciplinary approach has become the standard of care at leading cancer centers, recognizing that surviving and thriving with Stage 4 cancer requires addressing the biological, physical, emotional, and logistical dimensions of the disease simultaneously. As treatment protocols become increasingly sophisticated, so too does the framework for shared decision-making, allowing patients to maintain autonomy and purpose throughout their journey.
Understanding the Terminology: Stage 4 vs. Terminal Cancer
To understand the prognosis, it's crucial to first clarify the terms. The language used by medical professionals carries significant weight, and the difference between "Stage 4" and "terminal" is a critical one.
What Does Stage 4 Cancer Mean?
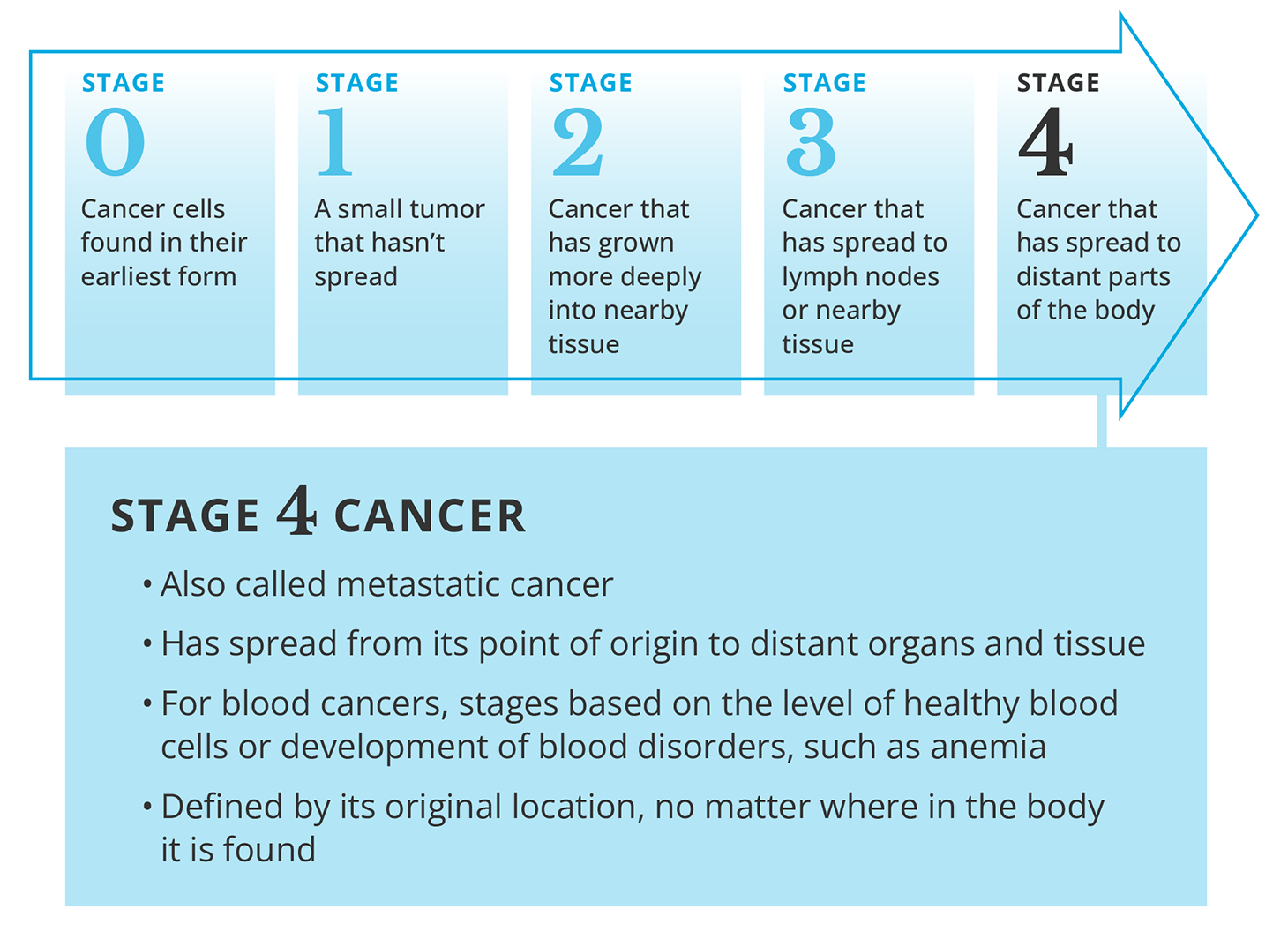
Stage 4 cancer, also known as metastatic cancer, means the cancer has spread (metastasized) from its original location to distant parts of the body. Cancer cells can break away from the primary tumor and travel through the bloodstream or lymphatic system to form new tumors in organs like the liver, lungs, bones, or brain.
 Source: Cancer Treatment Centers of America
Source: Cancer Treatment Centers of America
The stage of a cancer helps doctors determine the extent of the disease and plan the best course of treatment. It does not, however, automatically define the outcome.
In clinical practice, cancer staging typically follows the TNM system developed by the American Joint Committee on Cancer (AJCC). "T" refers to the size and extent of the primary tumor, "N" indicates whether cancer cells have spread to nearby lymph nodes, and "M" designates whether metastasis is present. A Stage 4 designation corresponds to an "M1" classification, confirming that distant metastasis has occurred regardless of the primary tumor's size or lymph node involvement. Understanding this biological progression is essential because it explains why localized treatments like surgery or localized radiation alone are rarely sufficient. Instead, systemic therapies that travel throughout the entire circulatory system become necessary to reach microscopic cancer cells circulating in the bloodstream or hiding in distant organs. Recent research into the metastatic cascade has revealed that cancer cells undergo epithelial-to-mesenchymal transition (EMT) to detach from the primary site, survive immune surveillance during transit, and colonize new tissues by adapting to entirely different microenvironments. Unpacking these mechanisms has directly led to the development of therapies that target not just rapidly dividing cells, but the specific pathways cancer uses to metastasize and evade detection.
The Critical Distinction: "Incurable but Treatable" vs. "Terminal"
While the terms are often used interchangeably in conversation, they have distinct medical meanings:
- Incurable but Treatable: This describes a condition that cannot be completely eradicated but can be managed with ongoing therapy. The goals of treatment are to control the disease, slow its progression, shrink tumors, and extend survival while maintaining a good quality of life. Many Stage 4 cancers now fall into this category.
- Terminal: A disease is considered terminal when it no longer responds to curative or life-extending treatments. At this point, the focus of medical care shifts from controlling the cancer to providing comfort, known as palliative or end-of-life care.
The psychological impact of this distinction is profound. Hearing "incurable but treatable" can instill a sense of hope and agency, empowering patients to participate actively in a long-term care plan.
Clinicians determine whether a cancer has transitioned from treatable to terminal based on objective clinical markers and performance status scales. When multiple lines of systemic therapy fail to halt tumor growth, when cancer progresses rapidly despite aggressive interventions, and when a patient's functional decline makes further treatment unsafe, the prognosis shifts toward terminal. However, this transition is not always abrupt. Many patients experience periods of stable disease, known as "treatment plateaus," where imaging scans show no new growth for extended periods. During these phases, oncologists may recommend maintenance therapy at lower doses or even treatment breaks to preserve immune function and minimize cumulative toxicity. Recognizing the fluidity of the disease course allows patients and providers to adjust expectations realistically without prematurely abandoning therapeutic options that could still offer meaningful benefit.
Why a Stage 4 Diagnosis Is Not a Monolith: Factors That Shape Your Prognosis
No two cancer cases are identical. A Stage 4 diagnosis is not a uniform sentence; the outlook is highly individual and depends on several key factors.
The Type of Cancer Matters Most
The single most significant factor in determining prognosis is the type of cancer. Survival rates for Stage 4 cancer vary dramatically from one type to another.
According to the National Cancer Institute's Surveillance, Epidemiology, and End Results (SEER) Program, 5-year relative survival rates for distant-stage cancers highlight this variance:
| Cancer Type | 5-Year Relative Survival Rate |
|---|---|
| Prostate | 34.1% |
| Breast | 31% |
| Colorectal | 15.6% |
| Lung | 8.2% |
| Stomach | 6.6% |
Source: Medical News Today, citing SEER data
It is vital to remember: These are statistics based on large groups of people diagnosed in the past. They do not predict an individual's outcome and may not reflect the impact of the very latest treatments.
Furthermore, these aggregate survival rates suffer from a significant temporal lag. SEER and other population-based registries typically report data that is several years behind the current clinical landscape. A patient diagnosed with Stage 4 lung adenocarcinoma in 2024 does not face the same statistical reality as a patient diagnosed in 2015, due to the rapid FDA approval of novel checkpoint inhibitors, antibody-drug conjugates, and targeted therapies over the past decade. Subtype differentiation also plays a massive role. For example, "lung cancer" encompasses non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC), each with drastically different biological behaviors, treatment algorithms, and prognoses. Within breast cancer alone, Stage 4 outcomes vary widely depending on hormone receptor status (ER/PR) and HER2 amplification. Understanding these molecular subcategories is the first step toward obtaining an accurate, personalized prognosis.
Other Key Factors Influencing Outlook
Beyond the cancer type, your medical team will consider:
- Patient's Age and Overall Health: Younger patients and those with fewer other health conditions generally have better outcomes.
- Location of Metastases: Where the cancer has spread can impact treatment options and prognosis.
- Genetic Makeup of the Cancer: Specific gene mutations in a tumor can make it vulnerable to new, highly effective targeted therapies.
- Response to Treatment: How well a cancer responds to initial therapy is a significant indicator of long-term prognosis.
In addition to these foundational elements, oncologists heavily rely on standardized assessment tools to gauge treatment tolerance and life expectancy. The Eastern Cooperative Oncology Group (ECOG) Performance Status scale, for instance, grades a patient from 0 (fully active) to 5 (deceased), directly correlating with survival outcomes and treatment eligibility. Patients with a status of 0-2 typically tolerate aggressive systemic regimens well, while those scoring 3-4 may require modified dosing or a pivot toward symptom management. Comorbid conditions like uncontrolled diabetes, cardiovascular disease, or chronic kidney disease can also complicate treatment, limiting the use of certain chemotherapies or targeted agents that require hepatic or renal clearance. Additionally, access to specialized care centers, eligibility for clinical trials, and the ability to adhere to complex medication schedules significantly influence real-world outcomes. Socioeconomic factors, health literacy, insurance coverage, and geographic proximity to comprehensive cancer networks can create disparities in care delivery, making it essential for patients to advocate for themselves or seek assistance from patient navigators and oncology social workers.
A New Era of Hope: How Modern Treatments Are Changing the Outlook
The narrative around Stage 4 cancer is being rewritten by groundbreaking advancements in treatment that are more precise and personalized than ever before.
The Goal of Treatment: From Cure to Control
For most Stage 4 cancers, the primary goal shifts from a complete cure to long-term control. Treatment aims to:
- Slow or stop the growth of cancer cells.
- Shrink existing tumors.
- Manage symptoms like pain or shortness of breath.
- Extend life and improve its quality.
This paradigm of chronic disease management mirrors the approaches successfully used in cardiology, endocrinology, and rheumatology. Just as patients with type 1 diabetes or HIV manage their conditions daily through medication, monitoring, and lifestyle adjustments, many Stage 4 cancer patients now take oral targeted therapies or receive scheduled immunotherapies to keep the disease in check. Treatment sequencing has become highly strategic. Oncologists often begin with first-line regimens that balance efficacy with tolerability, reserving more aggressive or novel therapies for subsequent lines as resistance develops. This "line of therapy" approach maximizes long-term outcomes by minimizing treatment-related fatigue, neuropathy, or organ damage. Furthermore, liquid biopsy technology is revolutionizing monitoring. By analyzing circulating tumor DNA (ctDNA) through simple blood draws, clinicians can detect molecular relapse months before it becomes visible on traditional CT or PET scans. This early warning system allows for preemptive treatment adjustments, potentially preventing symptomatic progression and extending progression-free survival intervals.
Breakthrough Therapies Rewriting the Rules
Conventional chemotherapy is no longer the only option. The advent of novel therapies is leading to durable, long-term responses in patients who previously had few options.
- Immunotherapy: These drugs unleash the body's own immune system to find and destroy cancer cells. They have shown remarkable success in treating advanced cancers like melanoma and non-small cell lung cancer.
- Targeted Therapy: These treatments attack cancer cells with specific genetic mutations, often with fewer side effects than traditional chemotherapy.
- Advanced Surgical and Interventional Techniques: For some patients, like those with colorectal cancer that has spread only to the liver, aggressive treatments like Hepatic Artery Infusion (HAI) pumps or even liver transplants can lead to long-term survival and, in select cases, a cure.
"Not too long ago, stage 4 colorectal cancer was considered a terminal illness. But new treatment discoveries continue to improve patient outcomes and survival rates. There are many reasons to be hopeful.” - Dr. Lauren Dias, Mass General Cancer Center. Source
Immunotherapy has fundamentally shifted oncology from cytotoxic cell killing to immune modulation. Checkpoint inhibitors (such as PD-1, PD-L1, and CTLA-4 inhibitors) work by removing the molecular "brakes" cancer cells place on T-cells, allowing the immune system to recognize and eradicate malignant tissue. However, response rates vary, prompting intensive research into biomarkers like tumor mutational burden (TMB) and microsatellite instability-high (MSI-H) to predict which patients will benefit. When immunotherapy does not elicit a response, combination strategies are emerging, pairing checkpoint inhibitors with radiation, chemotherapy, or cancer vaccines to create a synergistic effect. Targeted therapies have expanded exponentially with the advent of next-generation sequencing (NGS). Panels can now test for dozens of actionable mutations simultaneously, including EGFR, ALK, ROS1, BRAF, KRAS G12C, and NTRK fusions. The development of antibody-drug conjugates (ADCs) represents another leap forward, functioning as "guided missiles" that attach highly toxic payloads directly to cancer-specific surface receptors, sparing healthy cells and reducing systemic side effects. In parallel, radiation oncology has adopted stereotactic body radiation therapy (SBRT) and proton therapy, enabling highly precise, high-dose delivery to oligometastatic lesions (typically 1-5 metastases). This approach, sometimes called "oligometastatic-directed therapy," has demonstrated that eradicating limited metastatic deposits can delay systemic progression and, in select cases, induce long-term remission.
Stories of Resilience: Living with Stage 4 Cancer
Beyond the data are powerful stories of individuals who have defied their initial prognosis. U.S. Navy Veteran Matthew Roach, after being diagnosed with terminal stage 4 metastatic prostate cancer, underwent aggressive treatment at the Lubbock VA Clinic. A year later, his PSA levels were undetectable, and he rang a "celebration bell" he had donated to inspire others. His story is a powerful symbol of survival and the impact of dedicated care.
!Doctor and patient discussing scan results on a tablet in a modern clinic.:max_bytes(150000):strip_icc()/stage-4-cancer-5092070_color-b41add690efd427294f126c16723372c.jpg) Source: MedlinePlus - Advanced Cancer
Patient narratives also highlight the critical importance of psychosocial resilience, community support, and financial navigation. Many Stage 4 survivors credit peer support groups, online cancer communities, and integrative therapies like mindfulness-based stress reduction (MBSR), acupuncture, and supervised exercise programs for helping them cope with the emotional weight of a chronic diagnosis. Organizations like the American Cancer Society, CancerCare, and the Leukemia & Lymphoma Society offer free counseling, transportation assistance, copay relief, and educational workshops that empower patients to stay engaged in their care. Survivors frequently emphasize the value of maintaining routines, setting manageable goals, and finding purpose beyond the diagnosis—whether through advocacy, creative expression, volunteering, or mentoring newly diagnosed patients. These non-clinical pillars of survivorship do not replace medical treatment, but they profoundly influence a patient's capacity to tolerate therapy, adhere to appointments, and preserve mental well-being throughout a long, unpredictable journey.
Navigating the Journey: Quality of Life vs. Quantity of Life
With a focus on long-term management, a crucial conversation emerges: weighing the pursuit of a longer life against the quality of that life. This is a deeply personal negotiation.
The Personal Choice at the Heart of Treatment
Aggressive, life-prolonging treatments can come with significant side effects like nausea, fatigue, and pain. The decision to pursue a particular therapy involves a continuous dialogue between you, your family, and your healthcare team. It's essential to communicate your values, goals, and fears to ensure your treatment plan aligns with what matters most to you.
Shared decision-making frameworks are now standard in oncology, utilizing tools like decision aids, value clarification exercises, and structured goal-setting visits. Patients are encouraged to articulate what they want to prioritize: Is it attending a grandchild's graduation? Maintaining cognitive clarity to continue working? Traveling? Or simply minimizing hospital visits? Oncologists can then tailor regimens accordingly. For instance, a patient prioritizing cognitive function might avoid brain-penetrating chemotherapies that cause "chemo fog," opting instead for targeted agents with cleaner neurological profiles. Fatigue, one of the most pervasive side effects, can be managed through graded exercise programs, sleep hygiene optimization, anemia correction, and sometimes pharmacologic stimulants. Nausea and vomiting are now highly controllable with modern antiemetics like NK-1 receptor antagonists and 5-HT3 inhibitors, allowing patients to eat normally and maintain nutritional status. Pain management follows the World Health Organization's analgesic ladder, progressing from NSAIDs to opioids, neuropathic pain modulators (gabapentin, duloxetine), and interventional procedures like nerve blocks or epidural catheters when necessary. By proactively managing symptoms rather than reacting to them, treatment teams can preserve functional independence and ensure that life extensions remain meaningful.
The Essential Role of Palliative and Hospice Care
It's a common misconception that palliative care is only for the end of life.
- Palliative Care (Supportive Care): Its primary goal is to improve your quality of life by managing the symptoms of cancer and the side effects of treatment. It can and should be integrated at the time of diagnosis and provided alongside treatments meant to control the cancer.
- Hospice Care: This is a specific type of palliative care for patients in their final months. The focus shifts entirely to comfort when curative or life-extending treatment is no longer an option or desired.
Early integration of palliative care has been repeatedly shown in randomized clinical trials to improve survival, reduce emergency department visits, decrease depression and anxiety scores, and enhance overall satisfaction with care. Palliative specialists work concurrently with medical oncologists, managing complex symptom burdens, facilitating family meetings, addressing spiritual distress, and helping patients navigate advance directives. They are also skilled in navigating difficult conversations about prognosis, helping patients distinguish between realistic hope and false hope, and ensuring that care remains aligned with evolving patient values as the disease trajectory changes. When hospice care becomes appropriate, it provides comprehensive support in the patient's preferred setting, covering medications, medical equipment, nursing visits, bereavement counseling for families, and respite care for exhausted caregivers. The transition to hospice is not a failure of treatment; it is a medically and ethically sound pivot to prioritize dignity, comfort, and peace during life's final chapter.
Frequently Asked Questions About Stage 4 Cancer
How long can you live with Stage 4 cancer? There is no single answer, as life expectancy with Stage 4 cancer varies dramatically based on the cancer type, its genetic makeup, treatment response, and the patient's overall health. While some aggressive cancers have a prognosis of months, advances in treatments mean many patients can now live for years, managing the disease as a chronic illness. Median survival statistics continue to improve year-over-year as novel agents enter clinical practice. Some patients achieve long-term durable remissions spanning decades, particularly in cancers with strong targeted therapy options or high immunogenicity.
Can Stage 4 cancer be cured or go into remission? A complete cure for Stage 4 cancer is rare because the cancer has spread throughout the body. However, treatment can lead to long-term remission, where symptoms disappear and cancer becomes undetectable in tests. In these cases, the cancer is managed and controlled, but not considered permanently cured. The concept of "no evidence of disease" (NED) or "complete metabolic response" on PET scans is highly encouraging and often allows patients to resume normal activities, though ongoing surveillance remains necessary to monitor for molecular recurrence.
Is there a stage 5 cancer? Generally, no. The standard cancer staging system for most adult cancers ranges from Stage 0 to Stage 4. Stage 4 is the most advanced stage, indicating metastasis. The term 'Stage 5' is a misconception, though it is used for a specific childhood kidney cancer (Wilms tumor) to describe cases affecting both kidneys. Pediatric oncology occasionally utilizes modified staging systems, but for adult carcinomas and sarcomas, Stage 4 remains the definitive designation for systemic spread.
What are the symptoms of Stage 4 cancer? Symptoms depend on where the cancer has spread. For example:
- Bones: Bone pain, fractures.
- Brain: Headaches, seizures, dizziness.
- Lungs: Shortness of breath, persistent cough.
- Liver: Jaundice (yellowing of skin/eyes), abdominal swelling.
Additional systemic symptoms may include unexplained weight loss, persistent fatigue, night sweats, loss of appetite, and generalized weakness. Bone metastases frequently require bisphosphonates or RANK-ligand inhibitors (like denosumab) to prevent skeletal-related events. Brain metastases are often treated with steroids to reduce cerebral edema, alongside targeted radiation or neurosurgical intervention when accessible. Liver involvement can impair drug metabolism, necessitating careful dose adjustments and nutritional counseling to manage protein-calorie malnutrition. Prompt reporting of new or worsening symptoms to your care team is critical, as early intervention can prevent complications, hospitalizations, and irreversible organ damage.
Conclusion: Redefining Life Beyond a Stage 4 Diagnosis
So, is Stage 4 cancer terminal? While it is the most serious and advanced stage of the disease, it is not always a terminal diagnosis. The outlook is more hopeful and nuanced than ever before. It is a serious, often incurable condition, but it is also increasingly treatable.
The journey is a highly individual one, defined by your specific cancer, your health, and your personal goals. Open, honest communication with your medical team is the most powerful tool you have. By understanding your options and defining your priorities, you can navigate the path ahead with clarity, agency, and hope.
To take actionable steps forward, start by requesting a comprehensive molecular profile of your tumor to identify all potential targeted therapy options. Seek a second opinion from a National Cancer Institute (NCI)-designated cancer center, where multidisciplinary tumor boards review complex cases and clinical trial matching specialists can identify cutting-edge protocols not available locally. Prepare for oncology appointments with a written list of questions focusing on treatment goals, expected side effects, monitoring schedules, and contingency plans for disease progression. Build your support ecosystem by connecting with licensed oncology social workers, certified nutritionists, mental health professionals, and peer mentors. Remember that managing Stage 4 cancer is a marathon, not a sprint, requiring resilience, adaptability, and unwavering advocacy. With the continuous expansion of therapeutic arsenals, improved supportive care, and a growing community of long-term survivors, living meaningfully with advanced cancer is increasingly a reality. Your diagnosis is a chapter in your life, but with modern medicine and intentional care, it does not have to be the end of your story.
References
- American Cancer Society
- Cancer Treatment Centers of America. (2024). What Is Stage 4 Cancer and How Is Stage Four Treated?
- Kandola, A. (2020). Is stage 4 cancer curable? Survival rates and outlook. Medical News Today.
- Mass General Brigham. (2025). Stage 4 Colorectal Cancer Treatments Offer Hope.
- National Cancer Institute (NCI)
- VA Amarillo Health Care. (2025). Symbol of Survival: Navy Veteran defies stage 4 cancer diagnosis.
About the author
Carlos Ruiz, MD, FACS, is a board-certified urologist specializing in minimally invasive and robotic surgery for urologic cancers. He is a senior partner at a large urology group in Houston, Texas, and is involved in clinical trials for new prostate cancer treatments.