Dysarthria vs. Aphasia: Understanding the Key Differences

Key points
- Stroke: Especially strokes affecting the brainstem, cerebellum, or motor pathways. Ischemic or hemorrhagic events in these regions directly impair motor neuron function.
- Traumatic Brain Injury (TBI): Diffuse axonal injury or focal lesions can disrupt the neural networks responsible for motor coordination and timing.
- Neurodegenerative Diseases: Such as Parkinson's disease, Amyotrophic Lateral Sclerosis (ALS), Multiple Sclerosis (MS), and Huntington's disease. These progressive conditions gradually degrade neural integrity, leading to evolving speech profiles.
- Brain Tumors: Mass effect or surgical resection near motor cortex regions can compromise speech muscle innervation.
- Cerebral Palsy: A non-progressive neurological disorder arising from early brain development that frequently involves motor planning and execution deficits, including dysarthria.
- Guillain-Barré Syndrome and Myasthenia Gravis: Autoimmune or neuromuscular junction disorders that cause fluctuating muscle weakness, significantly impacting vocal and articulatory endurance.
Medically Reviewed by [Speech-Language Pathologist's Name], M.S., CCC-SLP
When a stroke, brain injury, or neurological condition affects communication, the terms "dysarthria" and "aphasia" often arise. While both disorders disrupt the ability to speak, they are fundamentally different. Understanding their unique characteristics is crucial for accurate diagnosis, effective treatment, and providing the right support for loved ones. The emotional toll of losing one's voice or ability to communicate is profound, often leading to social isolation, depression, and decreased independence. For patients, families, and healthcare providers, distinguishing between these conditions is the first critical step toward restoring connection and improving daily functioning.
Aphasia is a language disorder, affecting the brain's ability to process and use words. In contrast, dysarthria is a motor speech disorder, stemming from weakness or poor control of the muscles used for speaking.
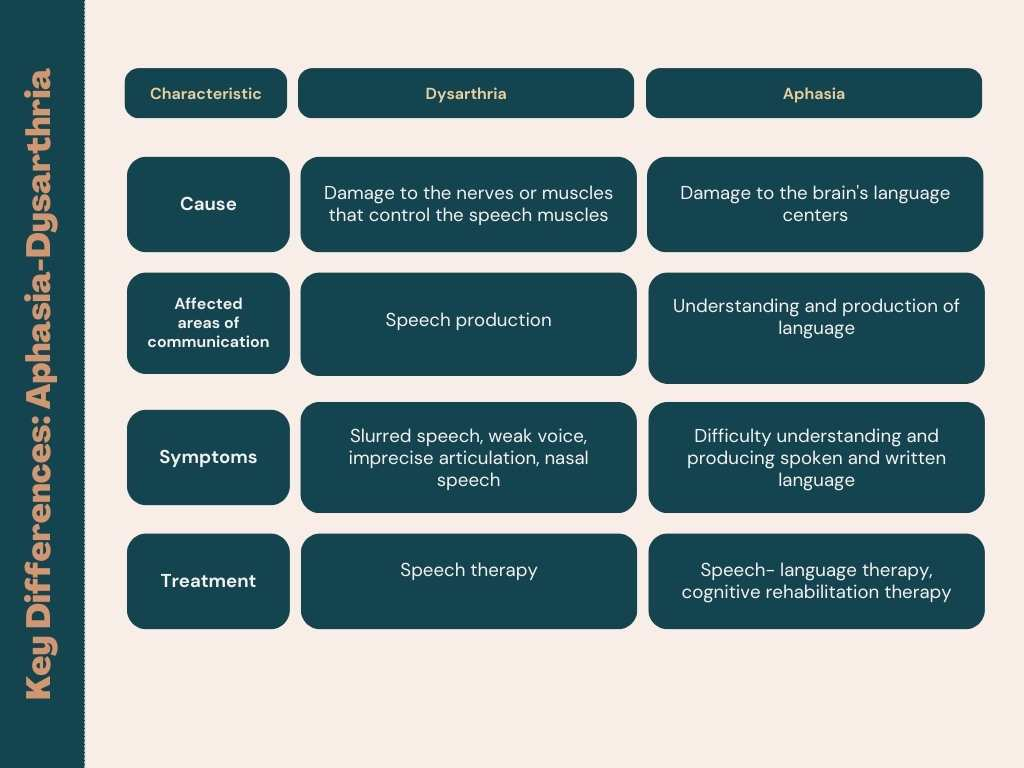
At a Glance: Dysarthria vs. Aphasia
This table provides a quick overview of the primary differences between the two conditions.
| Feature | Dysarthria | Aphasia |
|---|---|---|
| What It Is | Motor Speech Disorder | Language Disorder |
| Primary Problem | Muscle weakness or incoordination affects speech articulation. | Brain damage affects the ability to understand or produce language. |
| Core Deficit | The "how" of speaking (physical production of sounds). | The "what" of communication (word choice, grammar, meaning). |
| Language Comprehension | Generally intact. The person understands what is said to them. | Often impaired, especially in receptive or global aphasia. |
| Speech Characteristics | Slurred, slow, rapid, mumbled, monotone, breathy, or strained. | Difficulty finding words, using wrong words or sounds, producing short/fragmented sentences, or speaking fluently but nonsensically. |
| Reading & Writing | Unaffected, unless motor control of the hand is also impaired. | Almost always affected. |
 Source: Connected Speech Pathology
Source: Connected Speech Pathology
Beyond this quick comparison, it is essential to recognize that both conditions exist on a wide spectrum. A person with mild dysarthria might only struggle with clarity when tired or speaking quickly, while severe cases may render speech nearly unintelligible. Similarly, aphasia can range from occasional word-finding pauses to a complete loss of verbal expression and comprehension. The brain's remarkable capacity for neuroplasticity means that with targeted intervention, individuals can develop new neural pathways to bypass damaged regions, allowing for meaningful functional improvement over time.
Deep Dive into Dysarthria (The "How" of Speech)
Think of dysarthria as a mechanical problem. The brain knows exactly what it wants to say, but the muscles needed to articulate the words are weak, slow, or uncoordinated. The neurological signal originates correctly, but its transmission through the corticobulbar tracts or peripheral nerves to the cranial nerves (V, VII, IX, X, XII) is disrupted. This breakdown prevents the precise timing, force, and range of motion required for clear speech.
What Causes Dysarthria?
Dysarthria results from damage to the parts of the nervous system that control the speech muscles. Common causes include:
- Stroke: Especially strokes affecting the brainstem, cerebellum, or motor pathways. Ischemic or hemorrhagic events in these regions directly impair motor neuron function.
- Traumatic Brain Injury (TBI): Diffuse axonal injury or focal lesions can disrupt the neural networks responsible for motor coordination and timing.
- Neurodegenerative Diseases: Such as Parkinson's disease, Amyotrophic Lateral Sclerosis (ALS), Multiple Sclerosis (MS), and Huntington's disease. These progressive conditions gradually degrade neural integrity, leading to evolving speech profiles.
- Brain Tumors: Mass effect or surgical resection near motor cortex regions can compromise speech muscle innervation.
- Cerebral Palsy: A non-progressive neurological disorder arising from early brain development that frequently involves motor planning and execution deficits, including dysarthria.
- Guillain-Barré Syndrome and Myasthenia Gravis: Autoimmune or neuromuscular junction disorders that cause fluctuating muscle weakness, significantly impacting vocal and articulatory endurance.
Signs and Symptoms of Dysarthria
The specific sound of dysarthric speech varies based on the type and severity, but common characteristics include:
- Slurred, mumbled, or imprecise speech
- Abnormally slow or rapid rate of speech
- Monotone or robotic-sounding pitch
- Strained, hoarse, or breathy voice quality
- Nasal-sounding speech (hypernasality or hyponasality)
- Difficulty controlling volume (too soft or too loud)
- Reduced stress patterns and abnormal rhythm (prosodic abnormalities)
- Inconsistent intelligibility depending on fatigue, posture, or environmental noise
Types of Dysarthria
There are several types of dysarthria, each linked to damage in different parts of the nervous system. Clinicians use these classifications to tailor therapy to the specific neuromuscular profile:
- Spastic: Caused by damage to upper motor neurons (typically bilateral), resulting in slow, effortful, and strained-strangled speech. The vocal folds and articulatory muscles exhibit increased tone and reduced range of motion.
- Flaccid: Caused by damage to lower motor neurons or peripheral nerves, leading to a weak, breathy, and hypernasal voice. Muscle atrophy and fasciculations may be present.
- Ataxic: From damage to the cerebellum, causing uncoordinated, "drunken-sounding" speech with irregular breakdowns in articulation. Scanning speech (equal and excessive stress on syllables) is a hallmark.
- Hypokinetic: Most commonly associated with Parkinson's disease, characterized by a rapid rate of speech (festination), reduced loudness, monopitch, and imprecise consonants due to bradykinesia and rigidity.
- Hyperkinetic: Resulting from damage to the basal ganglia, causing involuntary movements that disrupt speech, leading to sudden changes in pitch and loudness, vocal arrests, or strained voice quality.
- Mixed: A combination of two or more types, common in conditions like ALS or severe TBI, presenting with overlapping symptoms that require highly customized management strategies.
Management often involves a combination of direct muscle training, compensatory techniques, and assistive technology. For example, LSVT LOUD (Lee Silverman Voice Treatment) is highly effective for hypokinetic dysarthria, while pacing strategies, amplification devices, and palatal lifts may benefit flaccid or spastic presentations.
Deep Dive into Aphasia (The "What" of Language)
Aphasia is a problem with the brain's language processing centers, most often in the left hemisphere. The person's intelligence is not affected, but their ability to access and use the "rules" of language—vocabulary, grammar, and sentence structure—is impaired. Neuroanatomically, aphasia typically involves the middle cerebral artery (MCA) territory, affecting critical hubs like Broca's area (inferior frontal gyrus), Wernicke's area (superior temporal gyrus), the arcuate fasciculus (connecting pathway), and subcortical structures.
Language is highly modular, and aphasia disrupts these modules differently depending on lesion location and extent. Importantly, language comprehension and production rely on complex, bilateral networks, which is why some recovery occurs in right-hemisphere homologues during rehabilitation. Aphasia does not reflect cognitive decline; rather, it represents a specific disruption in the neural coding and retrieval of linguistic information.
What Causes Aphasia?
The most common cause of aphasia is a stroke that damages language-dominant areas of the brain. Other causes include:
- Severe head injury
- Brain tumors
- Brain infections (e.g., encephalitis, abscess)
- Hypoxic-ischemic encephalopathy (prolonged lack of oxygen to the brain)
- Progressive neurological conditions like Primary Progressive Aphasia (PPA), a form of frontotemporal dementia characterized by gradual language network degeneration without significant early memory loss.
- Seizure activity (postictal aphasia) or transient ischemic attacks (TIAs)
Signs and Symptoms of Aphasia
Aphasia can affect all aspects of language. Key signs include:
- Anomia: Difficulty finding the right words, often manifesting as circumlocution (talking around the word) or frequent pauses.
- Paraphasias: Using the wrong word or sound (e.g., saying "table" for "chair," or "gable" for "table"). Phonemic paraphasias involve sound substitutions, while semantic paraphasias involve related concepts.
- Agrammatism: Speaking in short, fragmented phrases and omitting small connecting words (e.g., "Walk dog" instead of "I will walk the dog").
- Jargon: Speaking in fluent, grammatically correct sentences that are nonsensical, sometimes containing neologisms (invented words).
- Comprehension Difficulties: Trouble understanding spoken or written language, particularly with complex syntax or rapid speech.
- Impaired Reading and Writing: These skills are often affected similarly to speaking and understanding, though agraphia (writing impairment) and alexia (reading impairment) can occur independently.
- Repetition Deficits: Inability to accurately repeat words or phrases, a key diagnostic marker for conduction aphasia.
Types of Aphasia
Aphasia is broadly classified into fluent and non-fluent types based on speech output and effort, though modern classification also considers comprehension and repetition abilities.
Non-Fluent Aphasia
- Broca's Aphasia: The hallmark is effortful, halting speech with short sentences. While expression is difficult, the person's comprehension is usually relatively strong. Individuals are often aware of their difficulties, which can lead to significant frustration, depression, or anxiety. Therapy focuses heavily on verb retrieval, sentence-building drills, and melodic intonation therapy to leverage intact right-hemisphere musical processing.
Fluent Aphasia
- Wernicke's Aphasia: The person can speak in long, fluid sentences, but the words may be incorrect, made up, or strung together in a way that doesn't make sense. They often have significant difficulty understanding language and may be unaware of their own errors (anosognosia). Treatment emphasizes auditory comprehension training, contextual cueing, and functional communication strategies.
Conduction Aphasia
A less common subtype marked by intact comprehension and relatively fluent speech, but severely impaired repetition due to damage to the arcuate fasciculus connecting Broca's and Wernicke's areas.
Global Aphasia
This is the most severe form, caused by extensive damage to the brain's language networks, typically involving large MCA infarcts. It results in profound difficulties with both expressing and understanding language. Therapy at this stage focuses on establishing reliable yes/no responses, gesture training, and basic functional communication to prevent learned helplessness.
Can You Have Both Dysarthria and Aphasia?
Yes, it is common for both disorders to occur simultaneously, especially after a large stroke that affects both the language centers (cortical/subcortical) and the motor control pathways (brainstem/corticobulbar tracts) in the brain. This co-occurrence can make diagnosis challenging, as the slurred speech of dysarthria can overlap with the word-finding struggles of aphasia. A patient might exhibit reduced speech rate and articulatory imprecision from dysarthria, alongside severe anomia and paraphasic errors from aphasia, creating a complex clinical picture.
A comprehensive evaluation by a Speech-Language Pathologist (SLP) is essential to differentiate between the two conditions and understand how each contributes to the communication problem. Clinicians will administer separate assessments targeting motor speech execution versus linguistic processing. When both are present, an integrated, multimodal treatment plan is required. Therapy may alternate between strengthening oral musculature, practicing breath support, and drilling semantic word retrieval, ensuring that neither deficit is overlooked. Family members must also be educated on how to distinguish between a motor error and a language error to respond appropriately during daily conversations.
Clearing Up Confusion: Aphasia, Dysarthria, and Apraxia
To add another layer of complexity, a third condition called Apraxia of Speech is often confused with dysarthria and aphasia. Apraxia is a motor planning disorder. The muscles are not weak (as in dysarthria), but the brain has trouble planning and coordinating the sequence of movements needed to form words. Individuals with apraxia know what they want to say, but their brains cannot reliably translate that intention into the precise motor commands required for articulation.
Key differentiators include inconsistency of errors, difficulty initiating speech, and a "groping" or trial-and-error behavior with the mouth and tongue. Unlike dysarthria, where errors are consistent and predictable due to muscle weakness, apraxia errors vary from one attempt to the next. Unlike aphasia, language comprehension and reading remain largely intact, and the core issue lies purely in motor programming rather than linguistic knowledge.
| Disorder | Core Problem | Key Characteristic |
|---|---|---|
| Aphasia | Language | Difficulty with word choice, grammar, and comprehension. |
| Dysarthria | Muscle Weakness | Slurred, weak, or uncoordinated speech. Errors are consistent. |
| Apraxia | Motor Planning | Difficulty sequencing speech sounds. Errors are inconsistent, and the person may "grope" for the right mouth position. |
Modern therapeutic approaches for apraxia heavily rely on cueing hierarchies (visual, tactile, auditory), integral stimulation ("watch me, listen to me, do what I do"), and principles of motor learning, including high repetition and massed practice. Differentiating between these three conditions is critical because therapeutic targets and evidence-based protocols differ significantly.
Diagnosis and Treatment Pathways
Getting an Accurate Diagnosis
A neurologist and an SLP work together to diagnose these conditions. Neuroimaging (MRI, CT, DTI) provides structural and functional context, while standardized behavioral assessments quantify the specific deficits. An SLP will perform a detailed evaluation that includes:
- An oral motor examination to check the strength, tone, symmetry, and coordination of the lips, tongue, jaw, soft palate, and larynx. This directly helps differentiate dysarthria and apraxia from aphasia.
- Language testing to assess comprehension, word finding, grammar, reading, writing, and pragmatics. Tools like the Western Aphasia Battery (WAB) or Boston Diagnostic Aphasia Examination (BDAE) are commonly utilized.
- Speech analysis to evaluate articulation precision, rate control, prosody (rhythm and intonation), and vocal quality using standardized tools like the Frenchay Dysarthria Assessment or the Assessment of Motor and Process Skills (AMPS).
- Cognitive-communication screening to rule out co-occurring attention, memory, or executive function deficits that may mimic or exacerbate aphasia.
Treatment Approaches
Speech and language therapy is the primary treatment for both disorders, but the focus is different. Evidence-based practice dictates that therapy must be intensive, repetitive, and highly individualized to drive neuroplastic change.
- For Dysarthria: Therapy targets the physical aspects of speech. This may include exercises to improve respiratory support, strengthen articulators (where evidence supports), strategies to slow the rate of speech, techniques for speaking more loudly, and practice exaggerating sounds to improve clarity. Devices like amplification systems, pacing boards, or text-to-speech software may be introduced for functional communication. In progressive conditions, early voice banking and message construction are recommended.
- For Aphasia: Therapy focuses on rebuilding language skills and compensating for deficits. This can involve semantic feature analysis (linking words to their properties), phonemic cueing, verb network strengthening, melodic intonation therapy (MIT), and constraint-induced language therapy (CILT), which forces use of the impaired modality while restricting compensatory gestures. Technology-assisted apps and computer programs can facilitate independent home practice.
- For Co-occurring Conditions: The SLP will develop an integrated plan that addresses both motor speech and language goals, carefully balancing cognitive load to prevent fatigue and frustration. Task complexity is systematically graded, starting with high-support activities and gradually moving toward real-world conversational demands.
- Augmentative and Alternative Communication (AAC): For individuals with severe impairments, AAC devices—from simple picture boards and communication books to high-tech speech-generating devices (SGDs) and eye-gaze technology—can provide a vital way to communicate. AAC does not hinder natural speech recovery; in fact, it reduces communication anxiety and often stimulates vocal output by providing linguistic models and successful interaction experiences.
Communication partner training is equally vital. Family members learn to use modified communication strategies: speaking in a quiet environment, using short sentences, allowing ample response time, avoiding speaking for the person, asking yes/no or choice questions, confirming understanding, and utilizing multimodal input (gestures, writing, pointing).
Prognosis and Recovery: What to Expect
Recovery varies greatly depending on the cause, severity, and location of the brain damage, as well as the individual's age, overall health, and motivation. The brain's inherent plasticity allows for functional reorganization, but this process requires targeted stimulation and consistent practice.
- Dysarthria: Research suggests that dysarthria may resolve more frequently than aphasia after an isolated stroke, particularly if rehabilitation focuses on motor learning principles and compensatory pacing. For progressive conditions like ALS, MS, or Parkinson's, therapy shifts from recovery to maintenance, emphasizing vocal conservation, energy-efficient speech strategies, respiratory support, and early AAC integration to preserve communication independence as the disease evolves.
- Aphasia: Spontaneous neurological recovery is most significant in the first 3 to 6 months post-stroke. While a complete return to pre-injury linguistic levels is rare if severe symptoms persist beyond the initial recovery window, substantial functional improvement is absolutely possible for years, even decades, with dedicated, high-dose therapy. Neuroplasticity does not expire; it requires the right intensity and meaningful context. Persistent aphasia is often associated with more significant long-term functional challenges in vocational and social domains, but quality of life can still be profoundly improved through environmental modifications, support groups, and AAC.
- Intensity Matters: Studies consistently show that higher therapy intensity (more hours per week) correlates with better outcomes. Intensive comprehensive aphasia programs (ICAPs) and constraint-induced language therapy have demonstrated robust efficacy. However, therapy must be balanced with emotional well-being to prevent burnout and depression, which are highly prevalent in post-stroke communication disorders.
Support Systems and Long-Term Management
Living with dysarthria or aphasia extends far beyond clinical sessions. Long-term success relies heavily on community integration, psychosocial support, and lifestyle modifications. Support groups—both in-person and virtual—provide invaluable peer connection, reducing the profound isolation that often accompanies communication disorders. Organizations like the National Aphasia Association and the American Speech-Language-Hearing Association offer extensive resources, advocacy tools, and caregiver networks.
Caregiver education is a cornerstone of effective long-term management. Partners must learn to adapt their communication style, modify the home environment (reducing background noise, using visual aids, establishing predictable routines), and advocate for the individual in medical and social settings. Mental health support, including counseling for both the individual and family members, is crucial to address grief, role changes, and anxiety. Occupational therapists often collaborate to address fine motor deficits impacting writing or device use, while neuropsychologists help manage emotional lability and executive dysfunction.
Nutritional safety is another critical consideration, particularly in severe dysarthria. Weakness often extends to the pharyngeal and laryngeal muscles, increasing the risk of dysphagia (swallowing difficulty) and aspiration pneumonia. A modified barium swallow study (MBSS) or fiberoptic endoscopic evaluation of swallowing (FEES) should be considered when dysarthria is present, and diet texture or liquid consistency modifications may be necessary.
Frequently Asked Questions
Is dysarthria or aphasia permanent?
Not necessarily. Many individuals experience significant recovery, particularly when rehabilitation begins early and is sustained over time. Stroke-related speech and language deficits often show the most improvement within the first six months due to natural neurological healing and reduced cerebral edema. However, chronic aphasia and progressive dysarthria can be lifelong. The focus shifts from "curing" to maximizing functional communication, leveraging neuroplasticity, and integrating assistive technologies to ensure the individual remains connected to their environment.
Can dysarthria affect swallowing and eating?
Yes, frequently. The same cranial nerves and motor pathways that control speech articulation also govern the complex swallowing mechanism. Weakness or incoordination in the lips, tongue, or throat can lead to dysphagia, making it difficult to chew, safely transport food, or protect the airway during swallowing. If you or a loved one experiences coughing, choking, or a "wet" voice during meals, a comprehensive swallowing evaluation by an SLP is essential to prevent malnutrition and aspiration pneumonia.
How do I communicate with someone who has severe aphasia?
Effective communication requires patience, environmental control, and multimodal strategies. Reduce background noise, maintain eye contact, and speak at a normal volume and pitch in short, clear sentences. Give them plenty of time to respond—wait at least 10-15 seconds before repeating your question. Avoid finishing their sentences. Use gestures, pointing, drawings, or written keywords. Ask yes/no questions or provide simple choices. Confirm what you understood, and don't hesitate to ask them to write or gesture if they know how. Your calm, supportive presence reduces anxiety, which significantly improves their ability to access language.
Does apraxia of speech get worse over time?
It depends on the underlying cause. Childhood Apraxia of Speech (CAS) is developmental and typically improves significantly with intensive, motor-based speech therapy. In adults, apraxia of speech (AOS) is most commonly acquired from stroke or trauma and does not progressively worsen; rather, it plateaus as the brain heals. However, in neurodegenerative conditions like Primary Progressive Apraxia of Speech (a variant of PPA) or certain forms of Parkinson's disease, the symptoms may gradually decline over years due to ongoing neural degeneration. Early diagnosis and compensatory strategy training are key in progressive cases.
Are there medications that treat aphasia or dysarthria?
Currently, there are no FDA-approved medications specifically designed to cure aphasia or dysarthria. Treatment is primarily behavioral and delivered through targeted speech-language therapy. However, some neurostimulant and nootropic medications (like donepezil, memantine, or bromocriptine) are occasionally used off-label in specific aphasia cases or progressive neurological conditions to potentially enhance neuroplasticity, attention, or motor drive, though evidence is mixed. Any medication should be carefully evaluated by a neurologist. Importantly, medications that manage underlying conditions—such as Parkinson's treatments (levodopa/carbidopa) or muscle relaxants for spasticity—can indirectly improve speech intelligibility by optimizing motor control.
Conclusion
Distinguishing between dysarthria and aphasia is essential for effective clinical management, yet both represent profound disruptions to one of our most fundamental human functions: communication. Dysarthria is a mechanical, motor execution deficit where the muscles of speech falter despite intact language processing. Aphasia, conversely, is a linguistic disruption affecting the brain's ability to encode, retrieve, and comprehend words, grammar, and meaning, even when the speech apparatus is physically intact. While apraxia of speech adds a third layer of motor planning complexity, skilled speech-language pathologists are trained to differentiate these conditions and construct highly individualized rehabilitation plans.
Recovery is rarely linear, and the journey requires patience, intensive practice, and a strong support network. Whether through targeted articulatory training, language reconstruction techniques, compensatory pacing, or advanced AAC technology, meaningful communication is almost always achievable. If you or a loved one are navigating a sudden or progressive change in speech or language, seeking a prompt evaluation from a neurologist and a certified speech-language pathologist is the most critical step. With early intervention, evidence-based therapy, and unwavering community support, individuals can reclaim their voice, restore their independence, and maintain the vital connections that make life rich and fulfilling.
References
- Medical News Today. (2023). Aphasia vs. dysarthria: Differences, types, and more. https://www.medicalnewstoday.com/articles/aphasia-vs-dysarthria
- Connected Speech Pathology. (2024). Dysarthria vs. Aphasia Disorders: A Complete Guide. https://connectedspeechpathology.com/blog/dysarthria-vs-aphasia-disorders-a-complete-guide
- Better Speech. (2022). Dysarthria vs Aphasia: Definition and Key Differences. https://www.betterspeech.com/post/dysarthria-vs-aphasia
- Mayo Clinic. (2025). Aphasia: Symptoms and Causes. https://www.mayoclinic.org/diseases-conditions/aphasia/symptoms-causes/syc-20369518
- American Speech-Language-Hearing Association (ASHA). Dysarthria in Adults. Dysarthria
About the author
David Chen, DO, is a board-certified neurologist specializing in neuro-oncology and stroke recovery. He is the director of the Comprehensive Stroke Center at a New Jersey medical center and has published numerous articles on brain tumor treatment.