Dark Area on Gums: Causes, Evaluation, and Evidence-Based Treatment

Noticing a sudden or persistent dark area on gums can understandably trigger concern, especially when oral health is so closely tied to overall wellness. The human mouth is a highly dynamic environment, and the gingival tissue surrounding your teeth naturally reflects a wide spectrum of healthy colors, ranging from pale pink to coral, salmon, or deep brown. When a dark area on gums appears, it typically stems from melanin production, external pigment deposition, vascular changes, or medication effects. While the vast majority of these cases represent normal physiological variations or harmless side effects of lifestyle choices, distinguishing between benign pigmentation and clinically significant lesions is essential. Understanding the underlying mechanisms, recognizing warning signs that warrant immediate evaluation, and exploring evidence-based treatment pathways can provide clarity and peace of mind. This comprehensive guide explores the biological foundations of gingival coloration, examines common and systemic causes, outlines professional diagnostic protocols, and reviews modern cosmetic and clinical depigmentation techniques. Whether you are evaluating your own oral tissue or seeking information for a loved one, the following information aligns with current dental medicine standards and authoritative clinical research to help you navigate this common concern with confidence.
Understanding the Anatomy and Biology of Gum Color
The color of healthy gingival tissue is determined by a complex interplay of histological and physiological factors. At the microscopic level, the gingiva consists of a stratified squamous epithelium resting on a connective tissue matrix rich in collagen fibers, blood vessels, and immune cells. The visual appearance of the tissue depends heavily on epithelial thickness, the degree of keratinization, subepithelial vascularity, and the concentration of endogenous pigments. In lighter-skinned individuals, a thinner, highly keratinized epithelium allows the underlying red-orange blood vessels to dominate, resulting in a pink or coral hue. Conversely, individuals with darker constitutive skin tones naturally exhibit higher concentrations of melanin within the basal and suprabasal layers of the oral epithelium.
How Melanin Works in the Oral Mucosa
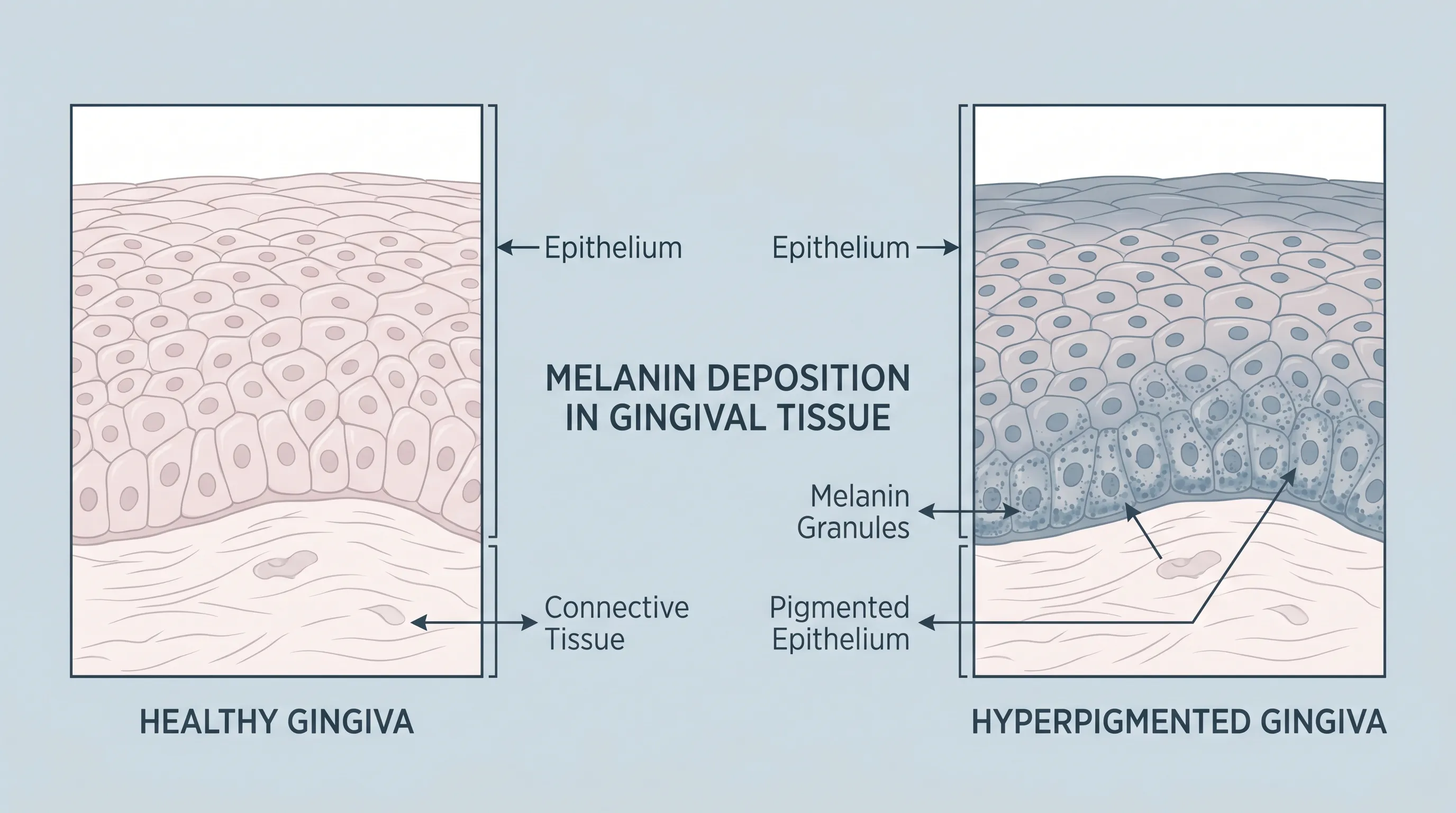
Melanin is a natural biopolymer produced by specialized cells called melanocytes. Unlike many other tissues, the oral mucosa houses a significant population of melanocytes, particularly along the attached gingiva, hard palate, and buccal mucosa. The coloration process is not driven by an increased number of melanocytes, but rather by heightened melanocytic activity. When stimulated by genetic programming, hormonal fluctuations, or environmental factors, melanocytes synthesize melanin granules within organelles called melanosomes. These granules are then transferred to neighboring keratinocytes, where they accumulate above the cell nuclei, providing photoprotection against ultraviolet and visible light radiation. Over time, this pigment accumulation becomes visible as a dark area on gums. Histological studies confirm that physiological gingival hyperpigmentation follows the same biochemical pathways seen in skin pigmentation, merely expressed in mucosal tissue.
The Role of Vascularization and Epithelial Thickness
Beyond melanin, the gingival vascular network plays a critical role in tissue coloration. Healthy gums maintain a rich capillary bed that supports tissue regeneration and immune surveillance. When inflammation occurs due to plaque accumulation, trauma, or periodontal disease, vasodilation increases blood flow, shifting gum color from pink to bright red or deep crimson. Chronic inflammation can also lead to post-inflammatory hyperpigmentation, where melanocytes become overactive in response to cytokine signaling. Additionally, variations in epithelial thickness affect how light scatters through the tissue. A thicker, more keratinized epithelium may appear paler or more opaque, while a thinner layer allows underlying melanin or vascular patterns to become more prominent. Clinicians use these visual cues, alongside probing and dermatoscopic evaluation, to assess whether a dark area on gums represents normal variation, inflammatory response, or a pathological process requiring intervention.
Primary Causes of a Dark Area on Gums
Identifying the root cause of gingival discoloration is the cornerstone of appropriate management. While patients often worry about serious disease upon noticing pigmentation, epidemiological data consistently shows that the majority of cases fall into benign, well-understood categories. Recognizing the specific characteristics of each cause helps guide clinical decision-making and prevents unnecessary anxiety.
Physiological (Racial or Ethnic) Pigmentation
Physiological gingival hyperpigmentation is the most prevalent cause of darkened gum tissue worldwide. It is a completely normal genetic trait that occurs independently across all age groups and genders, though it is markedly more common in individuals of African, Mediterranean, South Asian, Middle Eastern, and Indigenous descent. This condition typically presents as flat, light- to dark-brown or bluish-black patches that follow the contours of the attached gingiva. The pigmentation is characteristically bilateral and symmetric, often sparing the marginal gingiva and interdental papillae. From a developmental perspective, physiological pigmentation usually becomes apparent in childhood or adolescence and remains stable throughout adulthood. It requires absolutely no medical intervention, as it does not indicate disease, nor does it increase the risk of periodontal pathology. Patients seeking aesthetic modification may consult dental specialists, but from a clinical standpoint, physiological pigmentation is simply a manifestation of healthy, genetically determined tissue architecture.
Smoker’s Melanosis
Tobacco use remains one of the leading modifiable causes of oral hyperpigmentation. The chemical compounds in cigarette smoke, including polycyclic aromatic hydrocarbons and nicotine derivatives, penetrate the gingival epithelium and stimulate melanocytes to increase melanin synthesis. Smoker’s melanosis typically manifests as diffuse, brown to black macular patches on the labial and buccal gingiva. The condition is dose-dependent, meaning the severity correlates with the frequency and duration of tobacco use. Importantly, smoker's melanosis is entirely reversible. Once tobacco exposure ceases, melanocyte stimulation diminishes, and gradual repigmentation occurs. Clinical observations indicate that noticeable lightening begins within six to twelve months of complete cessation, with full resolution often taking up to three years. Dental professionals strongly emphasize smoking cessation not only for pigmentation reversal but also to dramatically reduce the risk of periodontal disease, tooth loss, and oral malignancies.
Medication-Induced Hyperpigmentation
Several systemic medications can trigger oral mucosal pigmentation as a known adverse effect. The mechanism typically involves drug-melanin binding complexes, altered melanocyte metabolism, or localized drug deposition in the gingival tissue. Common culprits include tetracycline-class antibiotics (particularly minocycline), antimalarial agents like hydroxychloroquine and chloroquine, antipsychotics such as phenothiazines, certain chemotherapeutic drugs, and long-term oral contraceptive use. Minocycline-induced pigmentation often presents as blue-gray or brownish discoloration that can affect both soft tissues and underlying bone. Antimalarials may cause slate-gray patches that resemble heavy metal poisoning. Drug-induced hyperpigmentation is generally benign and often resolves slowly after discontinuation or substitution of the offending agent, though patients must never alter their medication regimen without consulting their prescribing physician. A comprehensive medication review is a standard component of evaluating any unexplained dark area on gums.
Dental Materials and Trauma
Localized pigmentation frequently arises from iatrogenic or mechanical sources. An amalgam tattoo is a classic example, occurring when silver-containing dental restorative materials become embedded in the soft tissue during filling placement, crown preparation, or root canal therapy. The trapped metallic particles oxidize over time, creating a permanent blue-gray or black macule that is completely harmless but will not fade spontaneously. Diagnosis is typically straightforward, and confirmation can be achieved with dental radiography if the embedded material is visible. Traumatic pigmentation, on the other hand, results from localized injury such as aggressive tooth brushing, accidental bites, sharp food impaction, or ill-fitting dental appliances. The resulting bruising (hemorrhage into the tissue) appears as a purple or dark red patch that mimics melanin pigmentation but actually represents pooled blood. Unlike melanin deposits, traumatic bruises resolve naturally within one to two weeks as the body breaks down and clears the extravasated red blood cells. Differentiating between amalgam tattoos, bruises, and true melanotic lesions is a routine clinical skill.
Systemic Diseases and Underlying Health Conditions
While localized and physiological factors account for most cases, a dark area on gums can occasionally serve as an early clinical sign of systemic disease. Oral manifestations of internal disorders often precede other symptoms, making the dental examination a vital diagnostic checkpoint. Clinicians trained in oral medicine are skilled at recognizing mucosal clues that point toward broader physiological imbalances.
Endocrine and Autoimmune Disorders
Addison’s disease, also known as primary adrenal insufficiency, is perhaps the most well-documented systemic condition associated with gingival hyperpigmentation. When the adrenal cortex fails to produce adequate cortisol and aldosterone, the pituitary gland compensates by secreting elevated levels of adrenocorticotropic hormone (ACTH). ACTH shares a common precursor with melanocyte-stimulating hormone (MSH), meaning elevated ACTH levels inadvertently trigger widespread melanin production. Patients often present with characteristic bronze-like hyperpigmentation across sun-exposed skin, creases, scars, and notably, the oral mucosa. Dark patches typically appear on the buccal mucosa, palate, tongue, and gums. Because adrenal insufficiency is a potentially life-threatening condition requiring hormone replacement therapy, dentists frequently serve as the first to detect these early warning signs. Other endocrine disturbances, including hyperthyroidism and certain pituitary disorders, have also been anecdotally linked to mucosal pigmentation, though Addison's remains the primary systemic differential.
Genetic Syndromes and Rare Conditions
Several inherited syndromes feature distinctive oral pigmentation patterns. Peutz-Jeghers syndrome is an autosomal dominant disorder characterized by the development of hamartomatous gastrointestinal polyps and prominent mucocutaneous melanotic macules. These freckle-like spots commonly appear on the lips, perioral skin, buccal mucosa, and gingiva, typically emerging in infancy or early childhood. While the oral lesions themselves are benign, the syndrome carries a significant risk of gastrointestinal and extra-intestinal malignancies, requiring lifelong endoscopic surveillance and multidisciplinary care. Laugier-Hunziker syndrome is another rare, benign condition presenting with acquired hyperpigmentation of the lips, oral mucosa, and longitudinal nail streaks, predominantly in middle-aged adults. Unlike Peutz-Jeghers, it carries no associated malignancy risk but requires accurate diagnosis to prevent unnecessary interventions. When a patient presents with a dark area on gums accompanied by cutaneous, gastrointestinal, or familial symptoms, clinicians initiate a targeted workup involving genetic counseling, dermatological consultation, and appropriate laboratory testing.
When to Seek Professional Evaluation: Red Flags and Warning Signs
Distinguishing between harmless pigmentation and clinically concerning lesions relies on systematic assessment and clinical vigilance. While most dark areas on gums are stable and benign, certain morphological and temporal features demand prompt professional evaluation. Understanding the difference empowers patients to monitor their oral health effectively and seek care at the appropriate time.
Benign vs. Concerning Lesions
Benign pigmentation typically exhibits predictable, reassuring characteristics. Physiological and smoker-related melanosis are usually flat, symmetrically distributed, and uniform in color. They do not cause pain, bleeding, or tissue elevation, and they remain unchanged over years. In contrast, concerning lesions display features that align with clinical warning criteria. A newly appeared dark patch that lacks symmetry, exhibits variegated coloring (shades of brown, black, gray, or red mixed together), possesses irregular or notched borders, or demonstrates rapid enlargement over weeks or months requires immediate attention. Additional red flags include spontaneous ulceration, unexplained bleeding, nodular elevation, induration (hardening of the tissue), or associated pain. These clinical hallmarks mirror the ABCDE criteria adapted for oral mucosa and serve as essential triage tools. Early recognition is critical, as malignant conditions like oral melanoma, though exceedingly rare, progress rapidly and respond best to early surgical intervention.
Diagnostic Tools and Biopsy Protocols
When a lesion presents with atypical features, clinicians employ a structured diagnostic pathway. The process begins with a comprehensive medical and dental history, including medication review, tobacco and alcohol use, family history of skin or mucosal cancers, and symptom chronology. Visual inspection is enhanced with intraoral photography and, increasingly, dermatoscopy or optical coherence tomography, which allow visualization of pigment network patterns at a microscopic level without tissue disruption. If clinical suspicion persists, an incisional or excisional biopsy becomes necessary. Biopsy involves removing a small tissue sample for histopathological examination, where a pathologist evaluates cellular architecture, melanin distribution, nuclear atypia, and mitotic activity. As noted in expert clinical guidelines, clinicians must be prepared to biopsy any oral pigmented lesion that cannot be definitively diagnosed through history and visual examination alone. Early biopsy of focal pigmentations of undetermined etiology remains the gold standard for detecting rare malignancies at their most treatable stages.
Treatment and Management Options
Management strategies for gingival hyperpigmentation depend entirely on etiology, symptomatology, and patient preference. Physiological pigmentation and asymptomatic benign lesions require no intervention, while secondary causes demand targeted medical or lifestyle modifications. For individuals seeking aesthetic improvement, modern dentistry offers highly effective, evidence-based depigmentation techniques with minimal downtime.
Conservative and Medical Management
The first line of defense for non-physiological pigmentation involves addressing the underlying trigger. For smoker's melanosis, comprehensive tobacco cessation programs, nicotine replacement therapy, and behavioral counseling yield the best long-term outcomes. Pigmentation gradually fades as melanocyte stimulation resolves. When medication-induced hyperpigmentation is suspected, the prescribing physician may explore alternative therapeutic agents, adjust dosages, or monitor the patient closely, weighing cosmetic concerns against the necessity of the original treatment. Traumatic bruises resolve spontaneously, and amalgam tattoos require intervention only if they are misdiagnosed, cause psychological distress, or interfere with future dental procedures. In all conservative approaches, patient education, regular monitoring, and maintenance of optimal oral hygiene form the foundation of successful management.
Clinical Depigmentation Procedures
When a dark area on gums causes significant aesthetic concern or psychosocial distress, clinical depigmentation provides reliable results. The goal is to selectively remove the epithelium containing excess melanin while preserving underlying connective tissue to promote healthy regeneration. Techniques have evolved significantly over the past two decades, moving away from aggressive chemical peels toward precise, minimally invasive modalities. Modern procedures prioritize patient comfort, rapid healing, and predictable aesthetic outcomes.
Laser Therapy vs. Traditional Surgical Techniques
Laser-assisted depigmentation has emerged as the gold standard due to its precision, hemostatic properties, and reduced postoperative discomfort. Diode lasers operating at 980 nanometers are highly absorbed by melanin, allowing clinicians to target pigmented epithelium with minimal damage to adjacent tissue. Erbium-doped YAG (Er:YAG) lasers at 2940 nanometers offer excellent ablation efficiency with superior coagulation control, promoting favorable wound healing environments. Clinical studies comparing these modalities consistently demonstrate high patient satisfaction scores, reduced need for sutures or periodontal packing, and lower postoperative pain compared to conventional methods. Traditional techniques such as scalpel gingivectomy, electrosurgery, and cryosurgery remain viable but typically involve longer healing times, greater postoperative sensitivity, and higher recurrence rates. Air-abrasion (rotary brushing) is another mechanical alternative, though it requires significant operator skill to achieve uniform pigment removal.
| Procedure Type | Mechanism of Action | Anesthesia Required | Healing Time | Pain Level | Recurrence Risk | Best For |
|---|---|---|---|---|---|---|
| Diode Laser (980 nm) | Selective photothermolysis of melanin | Topical/Local | 5-10 days | Mild to Moderate | Low to Moderate | Generalized physiological pigmentation, high precision |
| Er:YAG Laser (2940 nm) | Water-absorbed tissue ablation | Local | 7-14 days | Minimal | Low | Patients prioritizing comfort & rapid epithelialization |
| Scalpel Gingivectomy | Mechanical epithelial removal | Local | 10-14 days | Moderate | Higher | Localized lesions, clinician preference |
| Electrosurgery | Radiofrequency tissue vaporization | Local | 10-14 days | Moderate | Moderate | Smoker's melanosis, budget-conscious care |
| Cryosurgery | Controlled tissue freezing | Topical/Local | 10-14 days | Moderate | Moderate to High | Patients avoiding anesthesia, widespread patches |
Regardless of the chosen method, recurrence depends heavily on individual genetics and ongoing environmental triggers. Patients who undergo laser or surgical depigmentation should maintain strict sun protection for facial tissues, avoid tobacco entirely, and adhere to gentle brushing techniques to preserve the newly healed epithelium. Follow-up appointments at six-month intervals ensure optimal healing and early detection of any pigment return.
Preventive Care and Daily Oral Hygiene Practices
Preventing secondary gum discoloration and maintaining optimal gingival health relies on consistent, evidence-based daily habits. While genetic pigmentation cannot be prevented, lifestyle and hygiene modifications significantly reduce the risk of acquired hyperpigmentation, periodontal inflammation, and early pathological changes.
Lifestyle Modifications
Eliminating tobacco use in all forms—cigarettes, chewing tobacco, vaping, and secondhand exposure—is the single most impactful step for preserving natural gum color and overall oral health. Chronic tobacco exposure not only stimulates melanin overproduction but also compromises microvascular circulation, delays wound healing, and dramatically increases the risk of squamous cell carcinoma. Adopting a balanced diet rich in antioxidants, vitamins C and D, and omega-3 fatty acids supports mucosal integrity and immune function. Limiting alcohol consumption and maintaining adequate hydration further protect the delicate oral epithelium from chemical irritation and dryness-induced inflammation. Stress management techniques, including mindfulness, regular exercise, and quality sleep, help regulate cortisol levels, which can indirectly influence mucosal health and inflammatory responses.
Routine Dental Visits and Monitoring
Professional dental cleanings every six months are essential for removing subgingival plaque and calculus that contribute to chronic inflammation and secondary pigmentation. During routine examinations, dental hygienists and periodontists perform comprehensive soft tissue screenings, documenting baseline gum color, symmetry, and texture. This creates a reference library for detecting subtle changes over time. Patients are encouraged to perform monthly self-examinations using a well-lit mirror, noting any new dark spots, asymmetry, texture changes, or persistent ulcers. If you observe a sudden dark area on gums accompanied by bleeding, swelling, or altered sensation, schedule an appointment promptly rather than waiting for the next scheduled cleaning. Early detection remains the most powerful tool in differentiating benign variations from clinically significant conditions. Maintaining excellent oral hygiene, attending regular dental checkups, and avoiding known mucosal irritants form the cornerstone of lifelong gingival health.
Frequently Asked Questions
Is a dark area on gums always a sign of oral cancer?
No, the vast majority of dark spots on the gums are completely benign. They are most often caused by natural physiological melanin production, tobacco use, dental restorations, or medications. However, any new, asymmetrical, rapidly changing, or ulcerated lesion should be evaluated promptly by a dental professional to rule out rare conditions like oral melanoma.
How long does it take for smoker's melanosis to fade after quitting?
Smoking cessation is the primary treatment for smoker's melanosis. Once tobacco exposure stops, melanin production gradually normalizes. In most patients, noticeable fading occurs within six to twelve months, though complete resolution can take up to three years depending on the duration and intensity of prior tobacco use.
Can I safely lighten dark gums at home with natural remedies?
There is no scientific evidence supporting home remedies like baking soda, hydrogen peroxide, or essential oils for safely removing gum pigmentation. These substances can cause severe tissue irritation, chemical burns, and permanent damage to the gingival epithelium. Professional laser or surgical depigmentation performed by licensed clinicians remains the only safe and effective approach.
Will dark gums grow back after laser depigmentation?
Recurrence is possible but not guaranteed. Physiological pigmentation depends on individual melanocytic activity and genetic factors. While modern laser treatments effectively remove existing melanin, natural pigment production may gradually return over a period of six months to several years. Maintaining excellent oral hygiene and avoiding tobacco significantly extends results.
Does a dark area on gums indicate poor oral hygiene?
Not necessarily. While plaque and tartar buildup can cause localized gingival inflammation and redness, melanin-based hyperpigmentation is primarily driven by genetics, systemic factors, medications, or tobacco use. However, maintaining rigorous oral hygiene remains essential for overall periodontal health and helps clinicians accurately monitor gum tissue for any concerning changes.
Conclusion
A dark area on gums is overwhelmingly a benign finding, reflecting natural melanin distribution, lifestyle habits, or harmless dental materials. The oral cavity's rich vascular and pigmentation network produces a wide range of healthy tissue colors, and understanding this physiological diversity helps prevent unnecessary concern. Nevertheless, clinical vigilance remains essential. Any newly appearing, asymmetrical, rapidly growing, or symptomatic pigmented lesion warrants prompt evaluation by a dentist or oral medicine specialist to exclude medication effects, systemic disease, or the exceptionally rare possibility of oral malignancy. For patients seeking aesthetic improvement, modern depigmentation techniques such as diode and Er:YAG laser therapy offer safe, precise, and highly effective solutions with minimal discomfort and rapid recovery. Regardless of whether treatment is pursued, maintaining excellent daily oral hygiene, committing to tobacco cessation, and attending routine dental screenings form the foundation of long-term periodontal and systemic health. By combining evidence-based clinical knowledge with proactive self-care, patients can confidently manage gum discoloration while safeguarding their overall well-being.
For further reading on oral pigmentation disorders, treatment protocols, and diagnostic guidelines, consult authoritative resources such as the Merck Manual Consumer Version: Color Changes and Spots in the Mouth, the comprehensive clinical review on Disorders of Oral Pigmentation from Medscape, and recent clinical trials comparing Laser Depigmentation Efficacy published in the International Journal of Dentistry (NCBI PMC). Additionally, explore detailed histological mechanisms in the ScienceDirect publication on Gingival Pigmentation.

About the author
Benjamin Carter, MD, is a board-certified otolaryngologist specializing in head and neck surgery, with an expertise in treating throat cancer. He is an associate professor and the residency program director at a medical school in North Carolina.