Understanding Ankle Cracking: Causes, Risks, and Expert Management Strategies

Key points
- Resisted Eversion and Inversion: Use a medium-tension resistance band anchored securely to perform slow, controlled repetitions focusing on the outer and inner lower leg. Perform 3 sets of 12-15 repetitions per side, emphasizing a 3-second eccentric lowering phase.
- Calf Raise Variations: Execute bilateral and single-leg calf raises on a flat surface, progressing to a slight elevation for increased range of motion. Complete 3 sets of 10-15 repetitions with controlled tempo to build Achilles and soleus strength.
- Tibialis Anterior Raises: Stand against a wall or sit upright with feet flat. Lift the toes and forefoot while keeping the heels grounded, holding briefly at the top. Perform 3 sets of 15-20 repetitions to strengthen anterior compartment muscles and improve dorsiflexion control.
- Single-Leg Balance Progressions: Practice standing on one leg for 30-60 seconds, progressing to closed-eye variations or unstable surfaces like foam pads. This enhances proprioceptive feedback and neuromuscular coordination, directly reducing compensatory snapping during dynamic movement.
Have you ever noticed a sudden, audible snap or pop when you stand up after sitting for a while, or perhaps when you gently twist your foot to stretch after a long day on your feet? That phenomenon is remarkably common, yet it often raises eyebrows—or at least sparks quiet concern—about what might be happening inside your lower extremities. When it comes to lower joint mechanics, many individuals experience audible sensations that range from harmless physiological releases to subtle indicators of structural changes. Understanding why your joints produce these sounds requires a closer look at anatomy, biomechanics, and the everyday habits that shape our mobility. While most people dismiss joint noises as mere quirks of the human body, ignoring them completely can sometimes mean missing early warning signs of underlying mechanical stress. By exploring the science behind these sounds, you will learn how to differentiate between normal physiological phenomena and situations that warrant professional evaluation. This comprehensive guide will walk you through the biological mechanisms, risk factors, self-care strategies, and preventive measures you need to keep your lower extremities moving smoothly for years to come. Whether you are an avid runner, a weekend athlete, or simply someone who spends long hours standing on hard surfaces, gaining clarity about joint acoustics empowers you to take proactive control of your mobility health.
The Anatomy Behind the Pop: What Actually Happens in Your Lower Joints?
To understand why joints produce sound, it is essential to first examine the intricate architecture that enables movement. The human lower extremity is a marvel of engineering, composed of multiple bones, ligaments, tendons, cartilage surfaces, and synovial compartments working in precise harmony. The primary weight-bearing structure in the foot and lower leg relies on a highly mobile hinge that allows dorsiflexion, plantarflexion, inversion, and eversion. Surrounding this complex junction is a sophisticated network of connective tissues that stabilize the joint while permitting fluid motion. When any component of this system shifts, stretches, or compresses under load, it can generate an audible release. The mechanisms responsible for these sounds fall into three primary categories: synovial cavitation, tendon or ligament movement, and cartilage surface irregularities.
Synovial Fluid Dynamics and Joint Cavitation
Inside every freely moving joint is a thin layer of synovial fluid, a viscous substance that serves as both a lubricant and a nutrient delivery system for avascular cartilage. This fluid contains dissolved gases, primarily nitrogen, oxygen, and carbon dioxide. When joint surfaces are rapidly separated during stretching or positional changes, the intra-articular pressure drops significantly. This sudden pressure reduction causes the dissolved gases to rapidly coalesce into a small vapor bubble, creating a distinct popping or cracking sound. The phenomenon, known as cavitation, has been extensively studied and confirmed through high-speed magnetic resonance imaging. The bubble formation requires time to re-dissolve back into the fluid, which explains why you cannot repeatedly crack the exact same joint in quick succession. This physiological release is entirely harmless, does not cause joint damage, and often leaves a temporary sensation of increased range of motion due to the brief reduction in joint capsule tension.
Ligament and Tendon Mechanics
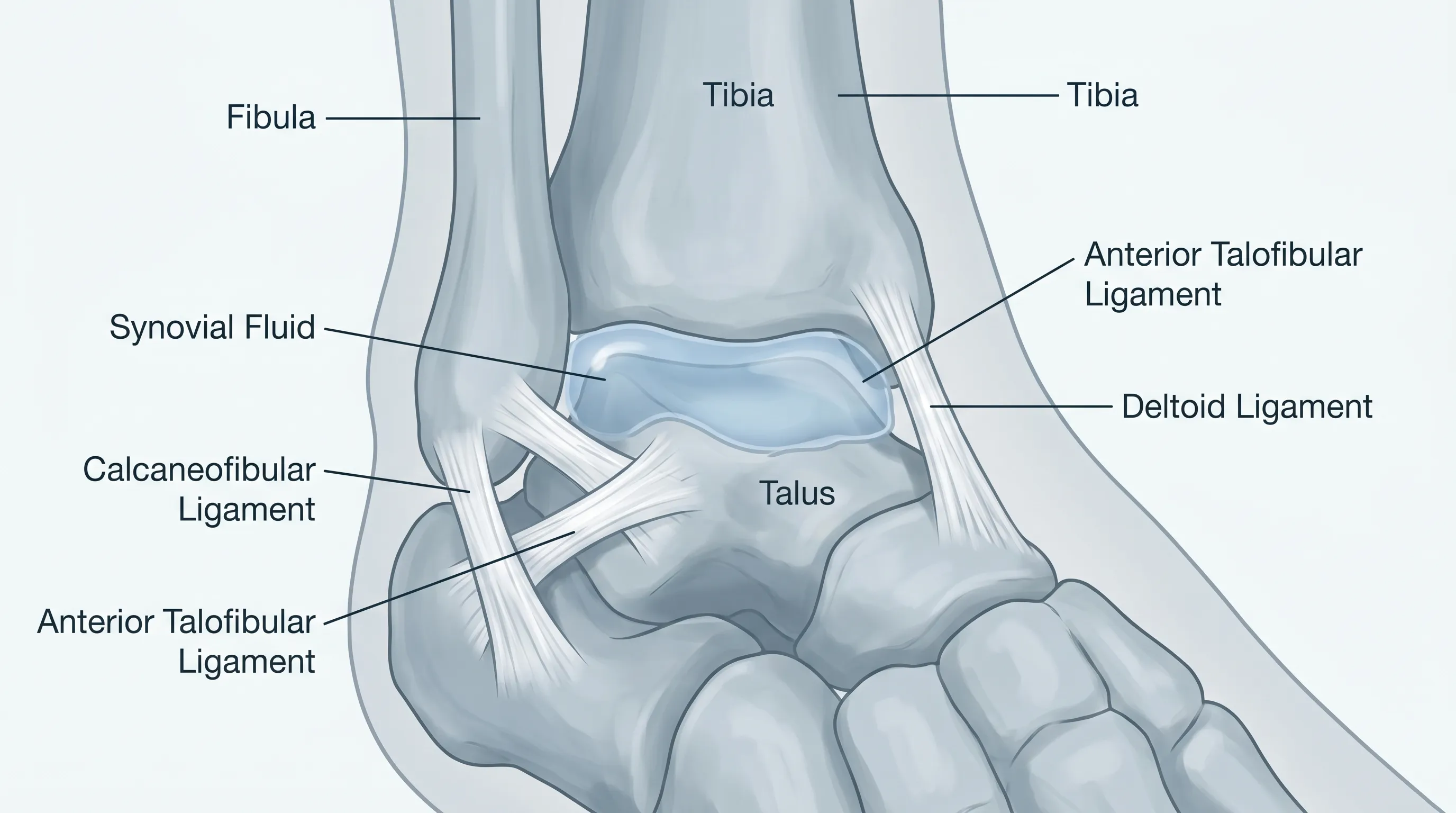
Another frequent source of joint noise involves the dynamic interaction between soft tissues and bony prominences. The human ankle is stabilized by multiple robust ligament complexes, including the lateral ligament group, the deltoid ligament medially, and the syndesmotic connections between the tibia and fibula. Overlying these ligaments are tendons from the peroneal, tibialis anterior, tibialis posterior, and flexor digitorum longus muscles. When these structures glide over anatomical ridges, bony landmarks, or slightly malaligned segments, they can snap audibly. This is particularly common during repetitive movements, sudden direction changes, or when muscle tension creates abnormal tracking patterns. Unlike cavitation, tendon and ligament snapping occurs on demand and is heavily influenced by muscular balance, flexibility, and postural alignment.
Cartilage Surface Changes
In degenerative or post-traumatic scenarios, the smooth hyaline cartilage covering the joint surfaces may develop microscopic roughening, fibrillation, or localized thinning. When compromised cartilage glides against opposing surfaces, it can produce a grinding or crunching sound known as crepitus. This differs distinctly from the sharp pop of cavitation or the snap of tendon movement. Crepitus is often associated with progressive stiffness, morning discomfort, and a gradual decline in functional mobility. Recognizing the acoustic difference between harmless gas release and cartilage-related grinding is crucial for determining whether the noise requires medical attention or can be managed conservatively.
Common Causes of Ankle Popping and Cracking
The reasons behind joint noises vary widely based on age, activity level, injury history, and genetic predisposition. While some causes are purely physiological and require no intervention, others reflect biomechanical inefficiencies or structural changes that benefit from targeted management. Understanding the underlying triggers allows you to respond appropriately rather than dismissing every sound or reacting with unnecessary alarm.
Physiological Joint Release
Harmless popping is the most prevalent explanation for occasional joint noises. It occurs naturally during stretching, standing up after prolonged sitting, or initiating movement after rest. The body experiences temporary stiffness from fluid redistribution and capsule tightening overnight or during sedentary periods. When movement resumes, pressure normalization releases gas bubbles, creating an audible signal. This process is completely benign and often correlates with a subjective feeling of joint "looseness" afterward. Research consistently shows that habitual physiological cracking does not accelerate wear or increase arthritis risk in healthy individuals.
Ligamentous Laxity and Microinstability
Chronic joint laxity develops from repetitive microtrauma, inadequate recovery from previous sprains, or inherent connective tissue variability. When ligaments become elongated or lose optimal tension, the joint experiences excessive accessory motion during weight-bearing activities. This hypermobility allows tendons and capsule structures to shift unpredictably, generating repetitive snapping or cracking sensations. Individuals with naturally flexible joints or those who participate in high-impact sports are particularly susceptible. Over time, unaddressed microinstability can contribute to compensatory muscle tightness, altered gait patterns, and increased joint stress during daily activities.
Post-Injury Scar Tissue Formation
Following an ankle sprain, fracture, or surgical procedure, the healing process often produces fibrous scar tissue within the joint capsule, ligaments, or surrounding soft tissues. Unlike healthy elastic tissue, scar tissue lacks organized collagen alignment and can restrict smooth gliding mechanics. When the joint moves through its range of motion, fibrotic bands can catch, stretch, or release against neighboring structures, creating audible pops or clicks. Proper rehabilitation during the subacute healing phase significantly reduces scar tissue adhesions, but incomplete recovery frequently leaves behind mechanical noises that persist for months or even years.
Degenerative Osteoarthritis
Age-related or post-traumatic degeneration gradually alters the joint environment. The protective cartilage thins, bone spurs may form along joint margins, and synovial fluid composition shifts toward a less viscous state. These changes collectively increase friction during movement and produce grinding, cracking, or clicking sounds that worsen with activity. Osteoarthritis remains one of the most common musculoskeletal conditions worldwide, and early recognition of acoustic changes paired with stiffness and pain enables timely intervention. Lifestyle modifications, targeted strengthening, and weight management can significantly slow progression and preserve functional mobility.
Footwear and Biomechanical Misalignments
Everyday footwear choices profoundly influence lower joint mechanics. Shoes with inadequate arch support, worn-out cushioning, or improper heel geometry force the foot into compensatory positioning. Overpronation, supination, and uneven weight distribution alter tendon tracking and increase ligament strain, creating repetitive snapping or cracking during walking, running, or standing. Additionally, structural variations such as flat feet, high arches, or leg length discrepancies can shift loading patterns across the lower kinetic chain, amplifying mechanical noises during routine activities.
When Should You Be Concerned About Ankle Cracking?
Distinguishing between normal physiological sounds and clinically significant symptoms is a critical skill for maintaining joint health. While most popping is harmless, certain accompanying signs indicate that professional evaluation may be necessary. Recognizing red flags early prevents minor mechanical inefficiencies from progressing into chronic pain or functional impairment.
Pain and Inflammatory Signs
The most important warning sign is the presence of pain alongside joint noises. Discomfort that occurs during the pop, immediately afterward, or lingers throughout the day suggests tissue irritation or structural strain. Swelling, warmth, or visible puffiness around the joint further indicates an active inflammatory response. When mechanical sounds consistently trigger pain or coincide with fluid accumulation, it is advisable to consult a musculoskeletal specialist to rule out ligament damage, cartilage injury, or synovial irritation.
Mechanical Locking and Giving Way Sensations
If your lower joint occasionally catches, locks in place, or suddenly buckles beneath you during weight-bearing, the acoustic changes likely reflect mechanical obstruction rather than harmless cavitation. Loose cartilage fragments, meniscal-like tissue irregularities, or severe ligament insufficiency can physically block smooth joint translation. These mechanical disruptions increase the risk of falls, recurrent sprains, and compensatory injuries higher up the kinetic chain. Immediate assessment is recommended when popping coincides with instability or intermittent locking.
Progressive Stiffness and Swelling
Gradual loss of range of motion, particularly when accompanied by persistent swelling, suggests underlying degenerative or inflammatory processes. Morning stiffness lasting longer than thirty minutes, difficulty pointing the foot upward or downward, and a sensation of "rustiness" during initial movement all point to synovial or capsular involvement. Tracking symptom progression over several weeks helps differentiate temporary overuse reactions from chronic joint changes.
History of Ankle Sprains
Individuals with a history of moderate to severe sprains face a higher likelihood of chronic mechanical noises due to residual ligament laxity and altered proprioception. If cracking sounds emerge months or years after the initial injury and correlate with recurrent instability or activity-related discomfort, targeted rehabilitation is essential to restore neuromuscular control and prevent long-term joint deterioration.
Practical Self-Care and Management Strategies
Implementing evidence-based self-care protocols can significantly reduce unnecessary joint noises, improve stability, and enhance overall functional mobility. A structured approach combining targeted strengthening, mobility work, supportive footwear, and recovery practices yields the most reliable results.
Targeted Strengthening Exercises
Strengthening the muscles that cross and stabilize the lower joint is the most effective strategy for reducing mechanical snapping. The peroneal muscles control lateral stability, while the tibialis anterior and posterior regulate medial support and arch integrity. A comprehensive routine should include:
- Resisted Eversion and Inversion: Use a medium-tension resistance band anchored securely to perform slow, controlled repetitions focusing on the outer and inner lower leg. Perform 3 sets of 12-15 repetitions per side, emphasizing a 3-second eccentric lowering phase.
- Calf Raise Variations: Execute bilateral and single-leg calf raises on a flat surface, progressing to a slight elevation for increased range of motion. Complete 3 sets of 10-15 repetitions with controlled tempo to build Achilles and soleus strength.
- Tibialis Anterior Raises: Stand against a wall or sit upright with feet flat. Lift the toes and forefoot while keeping the heels grounded, holding briefly at the top. Perform 3 sets of 15-20 repetitions to strengthen anterior compartment muscles and improve dorsiflexion control.
- Single-Leg Balance Progressions: Practice standing on one leg for 30-60 seconds, progressing to closed-eye variations or unstable surfaces like foam pads. This enhances proprioceptive feedback and neuromuscular coordination, directly reducing compensatory snapping during dynamic movement.

Mobility and Flexibility Routines
Tight calf muscles, restricted talocrural mobility, and limited foot intrinsic flexibility force surrounding tendons to overcompensate, increasing snapping frequency. Daily mobility work restores optimal tissue length and joint glide:
- Wall-Assisted Calf Stretch: Place hands against a wall, step one foot back, and press the heel firmly toward the floor. Keep the knee straight for gastrocnemius stretching, then bend the knee slightly to target the soleus. Hold each position for 45 seconds, repeating 3 times per leg.
- Joint Circles and Alphabet Tracing: While seated or reclining, slowly draw each letter of the alphabet with your big toe. This movement encourages multi-planar mobility, reduces capsule stiffness, and promotes synovial fluid circulation. Perform once or twice daily, particularly after prolonged rest.
- Plantar Fascia and Foot Intrinsic Mobilization: Use a textured rolling tool or frozen water bottle to gently roll the sole of your foot for 2-3 minutes per side. Follow with toe yoga exercises, spreading and curling the digits to activate small stabilizing muscles.
Proper Footwear and Orthotic Support
Footwear selection profoundly impacts joint acoustics and long-term structural health. Choose shoes with adequate arch support, a secure heel counter, and cushioning that matches your activity level. Replace athletic shoes every 300-500 miles, as compressed midsoles lose shock-absorbing capacity and alter biomechanical loading. For individuals with significant pronation or supination patterns, custom or over-the-counter orthotic insoles can realign weight distribution, reduce tendon tracking abnormalities, and eliminate unnecessary popping during walking and exercise.
Ice, Compression, and Anti-Inflammatory Care
When mechanical sounds coincide with mild overuse discomfort, targeted recovery practices prevent symptom escalation. Apply ice wrapped in a thin towel for 15-20 minutes post-activity to modulate inflammation. Compression sleeves can provide gentle proprioceptive feedback and reduce fluid pooling. Incorporate omega-3 fatty acids, turmeric, and adequate hydration to support systemic inflammation management. Avoid prolonged immobilization after minor discomfort, as controlled movement actually promotes fluid exchange and tissue healing.
Medical Interventions and Professional Treatments
While self-management resolves most benign joint noises, certain scenarios require structured clinical intervention. Understanding when and how professionals assess joint acoustics ensures you receive appropriate care without unnecessary delays or excessive procedures.
Diagnostic Imaging and Assessment
Musculoskeletal specialists begin with a comprehensive physical examination, evaluating range of motion, ligament integrity, tendon tracking, and joint stability. Special tests such as the anterior drawer and talar tilt assess lateral ligament competence, while palpation identifies localized tenderness or crepitus. When structural concerns persist, weight-bearing radiographs evaluate joint space narrowing, alignment, and bone spurs. Ultrasound imaging dynamically visualizes tendon movement during real-time motion, making it highly effective for diagnosing snapping peroneal tendon syndrome. Magnetic resonance imaging provides detailed cartilage, ligament, and bone marrow visualization when complex soft tissue injury or advanced degeneration is suspected.
Physical Therapy Protocols
A structured rehabilitation program addresses biomechanical deficits through progressive loading, neuromuscular re-education, and manual therapy techniques. Therapists utilize joint mobilizations to restore optimal capsule mobility, soft tissue massage to reduce fascial restrictions, and balance retraining to rebuild proprioceptive accuracy. Gradual exposure to plyometric drills, agility ladders, and sport-specific movements ensures safe return to high-demand activities. Adherence to home exercise programs significantly accelerates recovery and reduces recurrence rates.
When Surgery Becomes Necessary
Surgical intervention remains a last resort for mechanical joint issues. Indications include complete ligament ruptures causing chronic instability, severe osteochondral defects, loose bodies causing joint locking, or degenerative changes unresponsive to conservative management. Procedures such as ligament reconstruction, cartilage restoration, and ankle arthroscopy restore structural integrity and eliminate pathological clicking. Post-surgical rehabilitation follows phased protocols to protect healing tissues while progressively restoring function.
Prevention and Long-Term Joint Health
Proactive joint preservation relies on consistent daily habits that support connective tissue resilience, optimal biomechanics, and systemic metabolic health. Implementing sustainable prevention strategies minimizes mechanical stress and maintains smooth, pain-free movement throughout adulthood and aging.
Daily Movement Habits
Sedentary behavior accelerates joint stiffness and reduces synovial fluid circulation. Incorporate frequent movement breaks during desk work, standing or walking every 45-60 minutes. Replace high-impact running on hard surfaces with mixed training that includes cycling, swimming, or elliptical work to maintain cardiovascular fitness while reducing repetitive joint loading. Listen to early fatigue signals and schedule adequate recovery between intense training sessions to allow tissue remodeling.
Nutrition for Joint Integrity
Connective tissue requires specific micronutrients for collagen synthesis and cartilage maintenance. Prioritize lean protein sources rich in essential amino acids, particularly glycine and proline, which form collagen structural backbones. Consume vitamin C-rich foods to activate hydroxylation enzymes critical for collagen cross-linking. Include omega-3 fatty acids from fatty fish, flaxseeds, and walnuts to modulate inflammatory pathways. Adequate hydration maintains synovial fluid viscosity, directly supporting smooth joint gliding and reducing friction-related noises.
Warm-Up Routines Before Activity
Dynamic warm-ups significantly reduce mechanical stress during exercise. Begin with 5-10 minutes of light cardiovascular movement to elevate core temperature and increase blood flow. Progress to dynamic stretches including leg swings, ankle circles, walking lunges with torso rotation, and light bounding drills. Avoid static stretching before intense activity, as prolonged holding temporarily reduces muscle stiffness and can compromise joint stability during high-speed movements.
| Symptom Type | Typical Cause | Associated Features | Recommended Action |
|---|---|---|---|
| Sharp, single pop after rest | Synovial cavitation | Painless, improved mobility, infrequent | No intervention required; continue normal activity |
| Repetitive snapping during movement | Tendon tracking / ligament laxity | Occurs with specific motions, mild discomfort possible | Strengthen stabilizers, improve footwear, monitor progression |
| Grinding or crunching sound | Cartilage irregularity / osteoarthritis | Stiffness, swelling, activity-related pain | Professional evaluation, imaging, targeted rehab |
| Catching or locking | Mechanical obstruction / loose body | Sudden loss of motion, instability, recurrent giving way | Orthopedic consultation, diagnostic imaging, possible intervention |
Frequently Asked Questions
Is frequent ankle cracking harmful to joint cartilage?
Occasional joint popping caused by cavitation is not harmful and does not damage cartilage or lead to arthritis. However, if the cracking is accompanied by pain, swelling, or instability, it may indicate underlying structural changes that require professional evaluation. Maintaining consistent strengthening and mobility routines preserves cartilage health and reduces unnecessary mechanical stress.
How can I stop my ankles from cracking during exercise?
Proper warm-ups, targeted strengthening of the peroneal and calf muscles, dynamic mobility drills, and wearing supportive footwear can significantly reduce mechanical snapping. Consistency in low-impact conditioning and avoiding abrupt directional changes also help stabilize joint mechanics. If snapping persists despite corrective strategies, a physical therapy assessment can identify specific tracking abnormalities.
Does ankle cracking always mean arthritis is developing?
No. While osteoarthritis can cause joint noises due to cartilage roughening, most popping sounds stem from harmless gas bubble formation or tendon movement. Persistent grinding (crepitus) with stiffness and pain is a stronger indicator of degenerative changes. Early lifestyle intervention, weight management, and targeted exercise can slow progression regardless of acoustic changes.
What exercises strengthen the ankle joint safely?
Evidence-based routines include resisted ankle eversion/inversion with bands, single-leg balance progressions, calf raises, tibialis anterior raises, and controlled range-of-motion circles. These exercises improve proprioception, muscular support, and ligament stability. Perform movements 3-4 times weekly with progressive loading to build resilient connective tissue without overtraining.
Should I see a doctor if my ankle cracks but doesn’t hurt?
If the sound is painless, infrequent, and not accompanied by swelling or functional limitation, monitoring is usually sufficient. However, if the cracking began after trauma, worsens with activity, or restricts daily movement, scheduling a musculoskeletal assessment is recommended. Early evaluation prevents compensatory patterns from developing and ensures appropriate management strategies are implemented promptly.
Conclusion
Joint acoustics are a natural part of human biomechanics, reflecting the complex interplay between fluid dynamics, soft tissue movement, and structural integrity. Understanding why these sounds occur empowers you to distinguish between harmless physiological releases and meaningful clinical signals. By implementing targeted strengthening, optimizing footwear, maintaining consistent mobility practices, and recognizing red flags early, you can preserve lower joint function and prevent minor mechanical quirks from progressing into chronic limitations. Whether your goal is athletic performance, daily comfort, or long-term mobility preservation, a proactive, evidence-based approach to joint care yields sustainable results. Prioritize movement quality over quantity, listen to your body’s feedback, and seek professional guidance when symptoms persist beyond normal adaptation periods. With informed self-care and structured rehabilitation strategies, you can confidently manage joint sounds while maintaining active, pain-free movement throughout every stage of life.

About the author
Samuel Jones, MD, is a board-certified orthopedic surgeon specializing in joint replacement and orthopedic trauma. He is a team physician for a professional sports team and practices at a renowned orthopedic institute in Georgia.