Throbbing Tooth Pain: Causes, Evidence-Based Treatments & When to See a Dentist

Experiencing a throbbing tooth pain can instantly disrupt your daily life, turning simple tasks like eating, drinking, or even resting into agonizing challenges. Unlike a dull, background ache that fades into the periphery of your awareness, this pulsating sensation often signals that something deeper is occurring within the dental structure or surrounding periodontal tissues. When you feel that rhythmic, heartbeat-like pressure radiating from a single tooth, it is rarely a condition that will simply resolve with time. Understanding the underlying physiological mechanisms, recognizing the clinical warning signs, and knowing when to seek professional dental intervention are crucial steps toward protecting both your oral and systemic health. A throbbing tooth is your body’s direct communication channel, alerting you to inflammation, bacterial invasion, or structural compromise that requires prompt attention. By the end of this comprehensive guide, you will be equipped with evidence-based knowledge to navigate dental discomfort confidently, separate popular myths from clinically proven facts, and implement safe, effective strategies to manage your pain while you arrange for professional care. Whether you are dealing with sudden overnight onset or gradual worsening of symptoms, this article provides a complete medical overview, practical first-aid protocols, and long-term prevention strategies aligned with current guidelines from leading dental and medical institutions.
Understanding the Science Behind Throbbing Tooth Pain
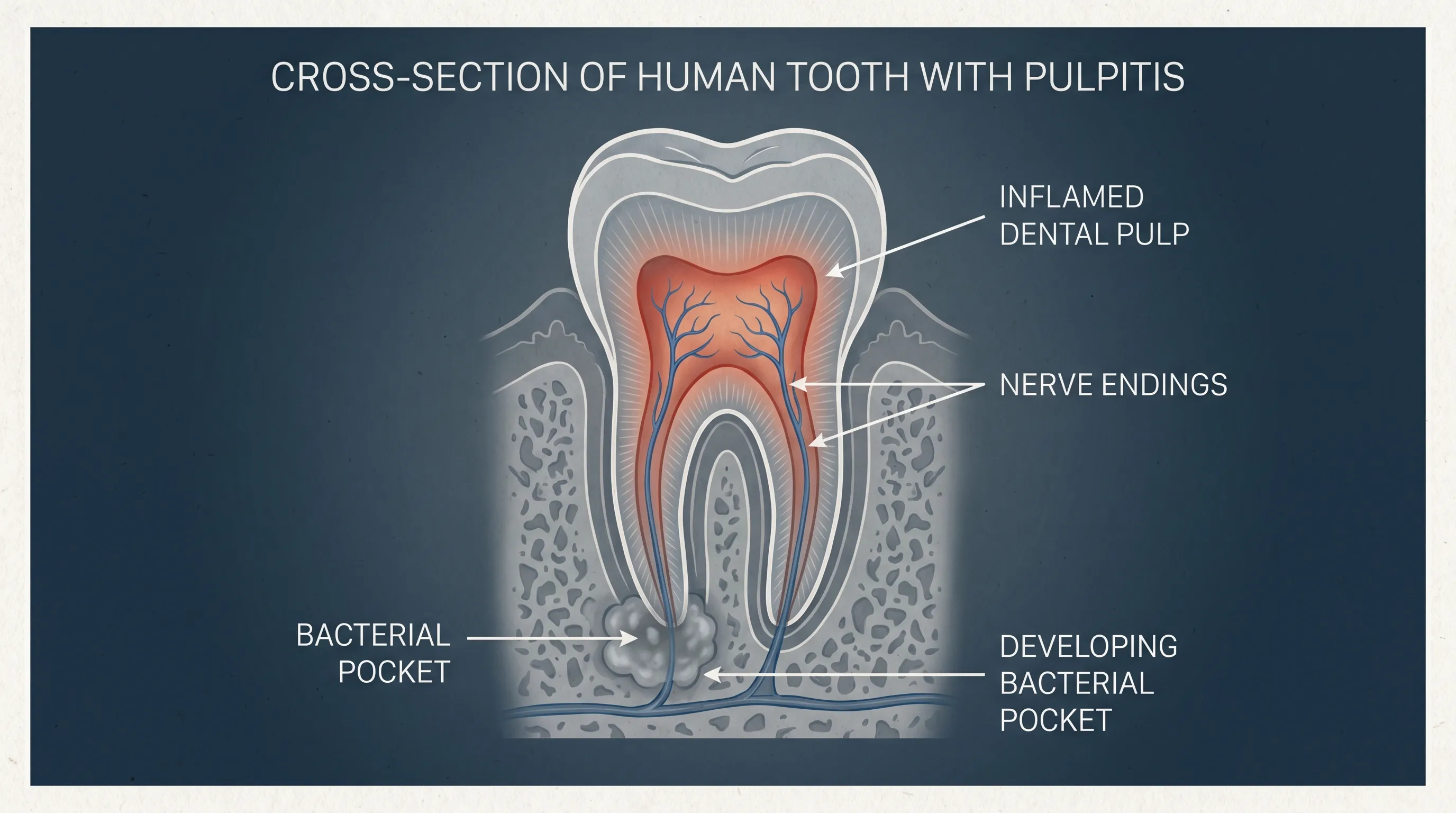
Dental pain operates through a highly specialized neurological and vascular network that differs significantly from typical musculoskeletal discomfort. When clinicians evaluate a throbbing tooth, they are observing a complex cascade of inflammatory mediators, vascular dilation, and nociceptive signaling that converges in the central nervous system. Research from the National Institutes of Health (NIH) highlights how the characteristic pulsation occurs because the inflamed dental pulp becomes trapped within a rigid, non-expandable chamber. As blood vessels dilate in response to infection or injury, the resulting increase in intra-pulpal pressure compresses sensory nerve fibers. This pressure fluctuates synchronously with your heartbeat, creating the unmistakable rhythmic throbbing that patients describe. Understanding this mechanism helps explain why over-the-counter pain relievers provide temporary relief but rarely eliminate the underlying issue without targeted dental treatment.
Why Does Dental Pain Throb?
The throbbing sensation is fundamentally a vascular phenomenon. Healthy dental pulp contains a delicate balance of arterioles, venules, and lymphatic vessels that maintain tissue vitality. When trauma, bacterial acids, or deep decay penetrate the enamel and dentin, the pulp initiates an inflammatory response. Mediators such as prostaglandins, bradykinin, and substance P are released, causing vasodilation and increased capillary permeability. Because the pulp is encased in hard dentin walls, there is no physical room for swelling. The resulting hydraulic pressure directly stimulates high-threshold A-delta and unmyelinated C fibers, which transmit sharp and dull aching signals, respectively. Research consistently demonstrates that the intensity of this pulsation correlates directly with the degree of pulpal inflammation and edema. This physiological reality explains why the discomfort intensifies when you lie down or bend over: positional changes temporarily increase craniofacial venous return, adding even more volume and pressure to the already compromised pulp chamber.
The Dentine-Pulp Complex and Nociception
The dentine-pulp complex functions as a unified sensory unit. Dentin contains microscopic tubules filled with fluid that extend from the enamel-dentin junction directly to the pulp. When these tubules are exposed by decay, enamel loss, or cracked tooth syndrome, external stimuli such as temperature changes, sweet foods, or even air flow cause rapid fluid displacement. This fluid shift mechanically activates odontoblast processes and free nerve endings in the pulp. A comprehensive review published in BMJ Open (Thompson et al., 2022) analyzed 27 clinical studies on acute dental pain and confirmed that evaluating outcomes requires tracking both objective clinical signs and subjective patient-reported metrics. The review highlighted that throbbing pain severity directly correlates with the progression of pulpal necrosis and periapical tissue breakdown, emphasizing the need for timely clinical intervention rather than prolonged self-management.
Referred Pain and the Trigeminal Nerve
Dental pain rarely stays isolated to a single tooth because of the trigeminal nerve's complex branching pattern. The maxillary and mandibular divisions of cranial nerve V transmit sensory input from all teeth, periodontal ligaments, gingiva, facial skin, and masticatory muscles. These afferent signals converge onto nociceptive neurons in the trigeminal subnucleus caudalis, also known as the medullary dorsal horn. Due to this neural convergence, the brain sometimes misinterprets the origin of pain signals. A severely inflamed lower molar can cause discomfort that radiates into the ear, jawline, temple, or even the neck. Similarly, an infected upper tooth can mimic sinus congestion or temporal headaches. Springler's research on dental pain pathogenesis confirms that this referred pain phenomenon occurs frequently in clinical practice, which is why dentists perform comprehensive percussion testing, thermal vitality assessments, and radiographic imaging to accurately pinpoint the offending tooth rather than relying solely on patient localization.
Common Causes of a Throbbing Tooth
Identifying the precise etiology of your discomfort is essential for selecting the correct treatment pathway. While the symptoms may feel identical across different conditions, the underlying causes range from reversible enamel demineralization to life-threatening systemic infections. The Cleveland Clinic and the American Association of Endodontists (AAE) have documented ten primary clinical categories responsible for persistent dental pain. Recognizing these patterns early allows patients to communicate effectively with dental professionals and avoid unnecessary delays in care.
Dental Caries and Progressive Pulpitis
Tooth decay begins when acid-producing bacteria metabolize dietary sugars, gradually dissolving the protective enamel layer. Once the decay breaches into the dentin, the process accelerates. If left untreated, bacteria eventually invade the pulp chamber, triggering pulpitis. Reversible pulpitis causes mild, transient sensitivity to cold, while irreversible pulpitis leads to spontaneous, lingering, and often throbbing pain that may persist for hours after the stimulus is removed. The transition from reversible to irreversible status marks a critical clinical threshold where restorative treatment alone is insufficient, and endodontic intervention becomes necessary to preserve the tooth structure and eliminate the source of infection.
Periapical Abscess and Bacterial Infection
A tooth abscess represents a localized collection of pus at the apex of the tooth root. This occurs when bacterial byproducts and necrotic tissue exit the apical foramen into the surrounding bone and periodontal ligament. The resulting inflammatory response creates significant pressure within the rigid alveolar bone, generating intense, unrelenting throbbing that worsens with biting pressure. Mayo Clinic guidelines emphasize that abscesses do not drain spontaneously in many cases and require professional intervention. Risk factors include prolonged poor oral hygiene, frequent consumption of fermentable carbohydrates, and xerostomia (dry mouth) induced by certain medications or medical conditions. Without timely drainage and definitive treatment, the infection can dissect through fascial planes into the maxillary sinus, submandibular space, or systemic circulation.
Cracked, Fractured, or Structurally Compromised Teeth
Microfractures and visible cracks can result from trauma, large unsupported restorations, or chronic parafunctional habits. A cracked tooth often exhibits sharp pain upon release of biting pressure, but as the fracture deepens toward the pulp, the discomfort shifts to a constant, rhythmic throbbing. Some fractures remain invisible to the naked eye and even evade standard two-dimensional radiography, requiring dental transillumination, cone-beam computed tomography (CBCT), or specialized staining techniques for accurate diagnosis. Delayed treatment of a cracked tooth frequently results in complete pulp necrosis and subsequent abscess formation.
Bruxism, Sinusitis, and Secondary Contributors
Chronic teeth grinding or clenching generates excessive occlusal forces that traumatize the periodontal ligament, causing diffuse, aching discomfort that can evolve into throbbing pressure, particularly in the morning. Additionally, viral or bacterial sinus infections can cause significant referred pain to the maxillary posterior teeth due to the close anatomical proximity between the floor of the maxillary sinus and the roots of these teeth. New orthodontic appliances, recently placed crowns with high bite contacts, and erupting impacted wisdom teeth also create inflammatory environments that mimic primary dental pathology. Differentiating these secondary triggers from true odontogenic disease requires thorough clinical evaluation and targeted diagnostic testing.
Recognizing the Symptoms and Warning Signs
Symptom recognition bridges the gap between early home care and urgent professional intervention. Dental pain follows predictable clinical patterns that signal the severity of tissue compromise. Paying close attention to these manifestations helps patients make informed decisions about self-care versus emergency dental visits.
Primary Pain Characteristics
The hallmark of a throbbing tooth is its persistent, pulsating nature that often escalates in intensity over several days. Unlike musculoskeletal aches that improve with rest or positional changes, dental throbbing frequently worsens at night when distractions diminish and craniofacial blood flow increases. The pain typically responds initially to temperature extremes, with hot or cold stimuli triggering sharp exacerbations. As pulpitis progresses to necrosis, heat sensitivity often becomes more pronounced while cold sensitivity paradoxically decreases, a clinical sign known as the 'hot sensitivity, cold relief' phenomenon frequently observed in advanced pulpal inflammation.
Associated Local and Systemic Symptoms
Mayo Clinic and Medical News Today document several accompanying signs that indicate spreading inflammation or established infection. Patients frequently report swelling of the cheek, jawline, or gingival tissues, along with tender, enlarged submandibular lymph nodes that react to bacterial byproducts in the drainage pathway. A foul taste or persistent bad breath often signals purulent drainage or anaerobic bacterial metabolism within the oral cavity. When an abscess spontaneously ruptures through the gingiva, patients may experience a sudden rush of salty, foul-tasting fluid followed by temporary pain relief as intra-pulpal pressure decreases. However, this drainage is rarely sterile, and the infection continues to proliferate beneath the gumline without professional debridement.
When Pain Becomes a Dental Emergency
Not every toothache requires a midnight trip to the emergency department, but specific red flags demand immediate action. Unbearable throbbing tooth pain accompanied by fever, chills, or malaise indicates that the localized infection has triggered a systemic immune response. Facial swelling that extends past the alveolar ridge into the facial soft tissues, particularly if it affects the submental space or approaches the eye, constitutes a potentially life-threatening condition. Difficulty swallowing, trismus (inability to fully open the mouth), or compromised airway function require immediate emergency medical evaluation to prevent rapid deterioration. The Cleveland Clinic explicitly notes that these combinations represent true dental emergencies where delayed intervention can lead to cavernous sinus thrombosis, Ludwig's angina, or sepsis.
Professional Treatments and Clinical Guidelines
Modern dentistry relies on a stepwise, evidence-based approach to managing acute dental pain and infection. Treatment selection depends entirely on the clinical diagnosis, radiographic findings, and pulpal vitality status. Understanding what to expect during professional care helps alleviate patient anxiety and ensures compliance with post-treatment protocols.
Evidence-Based Dental Interventions
When you present to a dental professional with a throbbing tooth, they will perform a comprehensive examination including vitality testing, percussion and palpation assessments, periodontal probing, and targeted imaging. Based on these findings, the clinician will determine whether the pulp is salvageable. Small cavities or minor enamel fractures typically receive direct composite restorations to seal the dentinal tubules and halt bacterial progression. Larger structural compromises may require full-coverage crowns or indirect restorations like inlays and onlays to redistribute occlusal forces and prevent future fractures. When bacteria have irreversibly damaged the pulp tissue, root canal therapy becomes the standard of care. This procedure involves careful debridement of the pulp chamber and root canals, disinfection with antimicrobial irrigants, and three-dimensional sealing with biocompatible materials to eliminate the infection source while preserving the natural tooth structure. In cases where the crown or root is severely compromised beyond structural repair, extraction followed by prosthetic replacement remains the only viable option to prevent chronic infection and bone loss.
ADA Guidelines on Antibiotics and Pain Management
A critical paradigm shift in dental medicine occurred with the 2019 American Dental Association (ADA) evidence-based clinical guideline on antibiotic use for dental pain. The guideline strongly recommends against prescribing antibiotics for most localized pulpal and periapical conditions, a stance fully supported by Centers for Disease Control and Prevention (CDC) antibiotic stewardship protocols. Research demonstrates that antibiotics cannot penetrate necrotic pulp tissue or abscess cavities effectively due to compromised blood supply and acidic, anaerobic microenvironments. Instead, the ADA advocates for definitive dental intervention combined with over-the-counter analgesics. Clinical trials consistently show that combining ibuprofen with acetaminophen provides superior pain relief compared to opioid prescriptions or antibiotics alone. Antibiotics are strictly reserved for cases demonstrating systemic involvement, immunocompromise, or rapidly spreading cellulitis. This antibiotic stewardship approach is endorsed by the American College of Emergency Physicians and aligns with global efforts to combat antimicrobial resistance while delivering faster, more effective patient outcomes.
Treatment Comparison and Clinical Pathways
| Treatment Modality | Primary Indication | Clinical Objective | Recovery Timeline |
|---|---|---|---|
| Direct Dental Fillings | Early caries, minor enamel/dentin breakdown | Seal dentinal tubules, halt decay progression | Immediate relief post-procedure, 24-48 hours for anesthesia wear-off |
| Inlays/Onlays/Crowns | Moderate to severe structural loss, cracked teeth | Restore occlusal function, protect remaining tooth structure | 1-2 weeks for cementation finalization, temporary sensitivity possible |
| Root Canal Therapy | Irreversible pulpitis, symptomatic periapical periodontitis | Remove necrotic tissue, disinfect canals, prevent reinfection | 3-7 days for acute inflammation resolution, full healing in months |
| Incision and Drainage | Localized fluctuant abscess, purulent accumulation | Evacuate pus, reduce tissue pressure, accelerate healing | Immediate pressure relief, 48-72 hours for soft tissue normalization |
| Tooth Extraction | Non-restorable fracture, advanced periodontal destruction | Remove infection source, prevent systemic complications | 3-5 days for initial clot stabilization, 2-3 weeks for gingival closure |

Safe Home Remedies and First-Aid Strategies
While definitive dental treatment is non-negotiable for resolving a throbbing tooth, evidence-based first-aid measures can provide crucial temporary relief and prevent secondary complications while you wait for your appointment. Implementing these strategies correctly ensures you do not inadvertently worsen the underlying pathology or introduce new oral health risks.
Immediate Relief and Hygiene Techniques
Begin by gently rinsing your mouth with warm saline solution. A mixture of half a teaspoon of salt in eight ounces of warm water acts as an isotonic cleanser that reduces edema, neutralizes acidic byproducts, and dislodges trapped food debris from cavities or around restorations. Follow the rinse with careful dental flossing to remove interproximal plaque or impactions that might be exerting additional pressure on inflamed tissues. Avoid aggressive brushing around the symptomatic area, as inflamed gingiva bleeds easily and can introduce additional oral bacteria into the microenvironment. Taking over-the-counter non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or acetaminophen according to manufacturer guidelines remains the most effective pharmacological intervention. These medications inhibit cyclooxygenase enzymes, reducing prostaglandin production and directly targeting the inflammatory cascade responsible for throbbing pressure, as recommended by clinical guidelines from NIH.
Evidence-Based Natural and Supportive Remedies
Several adjunctive approaches have demonstrated mild analgesic or antiseptic properties in dental literature. Cold compresses applied externally to the cheek for fifteen-minute intervals cause localized vasoconstriction, temporarily reducing blood flow to the inflamed pulp and decreasing pain signal transmission. Clove oil (eugenol) has documented antiseptic and mild anesthetic properties; a small amount applied sparingly with a cotton swab directly to a decayed tooth can provide temporary soothing, though it must be kept away from gingival tissues to avoid chemical irritation. Peppermint tea bags contain menthol, which produces a mild cooling sensation and transient analgesic effect when placed against the affected area. Garlic releases allicin, a compound with documented antimicrobial activity, though its strong flavor and potential tissue irritation limit its clinical utility. These methods should strictly be viewed as temporary bridges to professional care, not curative treatments.
Critical Warnings and Practices to Avoid
The FDA has issued explicit warnings regarding over-the-counter topical anesthetics containing benzocaine, particularly in patients under two years old, due to the rare but potentially fatal risk of methemoglobinemia, a condition that severely impairs oxygen transport in red blood cells. Even in adults, excessive use of topical gels can cause mucosal sloughing and secondary ulceration. Never place aspirin, vinegar, alcohol, or hydrogen peroxide directly against a tooth or gum. Aspirin is a caustic acid that dissolves mucosal tissue upon contact, creating painful chemical burns. Undiluted hydrogen peroxide can cause necrosis of healthy epithelial cells and delay natural healing. Furthermore, attempting to lance, drain, or extract a tooth at home introduces uncontrolled bacterial contamination, risks aspiration of tooth fragments, and often drives infection deeper into fascial spaces. If pain persists beyond forty-eight hours, if swelling develops, or if you experience fever, professional evaluation becomes medically urgent.
Prevention and Long-Term Oral Health Strategies
A throbbing tooth is rarely an isolated, random event. It is typically the end result of prolonged ecological shifts within the oral microbiome, compromised defensive barriers, or delayed clinical intervention. Implementing proactive, evidence-based preventive strategies significantly reduces the likelihood of experiencing severe dental emergencies and preserves natural tooth structure for a lifetime.
Daily Hygiene and Mechanical Plaque Control
Effective plaque removal disrupts the biofilm that harbors acidogenic and aciduric bacteria. Brushing twice daily with a fluoride-containing toothpaste for two minutes ensures adequate remineralization of early demineralization lesions. Fluoride integrates into the hydroxyapatite crystal structure, forming fluorapatite that resists acid dissolution at lower pH levels. Interdental cleaning with dental floss or water flossing devices removes plaque from contact areas that toothbrushes cannot reach, preventing proximal caries that frequently progress to the pulp undetected. Replacing toothbrushes every three to four months or immediately after bristle fraying maintains optimal cleaning efficacy. For patients with dry mouth, xerostomia management through saliva substitutes, sugar-free xylitol products, and increased hydration becomes critical, as saliva serves as the mouth's natural buffering and cleansing system.
Lifestyle Modifications and Dietary Factors
Dietary patterns directly influence the frequency and duration of acid attacks on tooth structure. Reducing the frequency of fermentable carbohydrate and sugary beverage intake prevents prolonged pH drops below the critical threshold of 5.5, where enamel begins to demineralize. Consuming acidic foods and drinks alongside meals, rather than sipping them continuously throughout the day, minimizes the duration of acid exposure. Rinsing with water after meals helps neutralize residual acids. Smoking cessation is equally vital, as tobacco use impairs gingival blood flow, compromises immune cell function, and significantly increases the risk of periodontal disease and delayed wound healing following dental procedures. Managing systemic conditions like diabetes also plays a crucial role, as uncontrolled glycemic levels impair neutrophil function and accelerate periodontal breakdown, creating pathways for bacterial invasion into deeper tooth structures.
Professional Monitoring and Early Intervention
The American Dental Association and CDC guidelines emphasize that biannual professional cleanings and examinations are essential for detecting pathology before it progresses to symptomatic stages. Dental radiographs reveal interproximal caries, periapical radiolucencies, and bone loss that are completely invisible during self-examination. Professional fluoride applications and pit-and-fissure sealants provide additional protective barriers for vulnerable surfaces. Addressing parafunctional habits through custom-fabricated occlusal guards prevents enamel attrition and microfracture formation. Early detection of reversible pulpitis or small carious lesions allows for minimally invasive treatments that preserve vitality, whereas delayed presentation almost invariably necessitates complex, multi-visit procedures. Establishing a trusted dental home ensures continuity of care, personalized risk assessment, and rapid access to emergency management when acute symptoms do arise. The World Health Organization (WHO) further emphasizes that integrating routine oral care into broader primary health frameworks is essential for long-term systemic well-being.
Frequently Asked Questions
Why does a throbbing tooth hurt more at night?
The intensification of dental pain during nighttime hours stems from physiological and environmental factors. When you lie down, hydrostatic pressure changes increase craniofacial blood flow, elevating intra-pulpal pressure in an already inflamed chamber. Additionally, cortisol levels naturally decrease at night, reducing the body's endogenous anti-inflammatory response. The absence of daytime distractions also lowers your pain threshold, making the pulsating sensation more prominent and difficult to ignore.
Can a throbbing tooth heal on its own without dental treatment?
Once a tooth reaches the stage of spontaneous, rhythmic throbbing, the underlying pulp tissue is typically irreversibly damaged or necrotic. Unlike superficial skin wounds, the dental pulp lacks regenerative capacity when severely compromised by bacterial invasion or traumatic injury. While pain may temporarily subside if the nerve tissue dies completely, the infection continues to spread into the periapical bone. Leaving a throbbing tooth untreated almost always results in abscess formation, bone destruction, and potential systemic complications.
Are prescription opioids effective for dental pain?
Current clinical evidence consistently demonstrates that prescription opioids provide inferior pain relief for acute dental pain compared to NSAID and acetaminophen combinations, and they carry significantly higher risks of dependence, tolerance, and adverse side effects. The ADA, American Association of Endodontists, and major medical organizations recommend against first-line opioid prescribing for dental pain. Non-opioid regimens targeting inflammation directly address the pathophysiology of throbbing dental pain while maintaining a much safer systemic profile.
How soon should I see a dentist after a throbbing tooth begins?
Schedule a professional evaluation within twenty-four to forty-eight hours of experiencing persistent throbbing pain. Delaying beyond this window allows bacterial proliferation and tissue destruction to progress, often transforming a straightforward, single-visit restorative procedure into a complex endodontic or surgical intervention. If you notice rapid swelling, fever, difficulty opening your mouth, or pain that radiates significantly, seek immediate emergency dental or medical care rather than waiting for a routine appointment.
What is the difference between a toothache and referred pain from other conditions?
True odontogenic pain typically localizes to a specific tooth, responds predictably to thermal stimuli or biting pressure, and worsens with positional changes or heat application. Referred pain from conditions like trigeminal neuralgia, temporal arteritis, cardiac ischemia (in rare cases), or maxillary sinusitis often presents as diffuse discomfort across multiple teeth, lacks clear dental triggers on examination, and accompanies other systemic or neurological symptoms. Comprehensive dental diagnostics, including vitality testing, radiographic imaging, and clinical correlation, reliably differentiate primary dental pathology from secondary referred pain syndromes.
Key Takeaways
A throbbing tooth serves as a critical physiological warning sign that demands attention, not dismissal. The rhythmic, pulsating nature of this pain originates from vascular pressure within an inflamed, confined pulp chamber, typically triggered by advanced decay, bacterial infection, structural fractures, or severe periodontal compromise. Evidence-based clinical guidelines emphasize that antibiotics alone cannot resolve localized dental infections; definitive intervention through restorative dentistry, endodontic therapy, or extraction remains the only path to permanent resolution. While temporary home management strategies like warm saline rinses, cold compresses, and appropriate NSAID use can bridge the gap to professional care, they should never delay evaluation, especially when systemic symptoms or facial swelling develop. Prioritizing consistent preventive hygiene, regular professional monitoring, and prompt response to early sensitivity signs significantly reduces the risk of progressing to debilitating dental emergencies. By understanding the science, recognizing the symptoms, and adhering to clinically validated treatment pathways, you can effectively manage dental discomfort, preserve your natural dentition, and maintain optimal overall health for years to come.

About the author
Benjamin Carter, MD, is a board-certified otolaryngologist specializing in head and neck surgery, with an expertise in treating throat cancer. He is an associate professor and the residency program director at a medical school in North Carolina.