Hyperextended Elbow: A Comprehensive Guide to Causes, Treatment, and Recovery

Key points
- Grade I (Mild): The ligaments are microscopically stretched but remain intact. Patients experience mild pain and minimal loss of function. The joint remains stable, and full recovery usually occurs within two to four weeks.
- Grade II (Moderate): Partial tearing of the ligaments occurs. There is noticeable swelling, bruising, and a clear loss of range of motion. The joint may feel slightly unstable during certain movements, requiring four to six weeks of structured rehabilitation.
- Grade III (Severe): Complete ligamentous rupture, often accompanied by joint subluxation (partial dislocation), cartilage damage, or associated fractures. This grade typically involves significant instability, severe pain, and a prolonged recovery timeline that may span several months and occasionally require surgical reconstruction.
A hyperextended elbow occurs when the arm is forcefully straightened past its normal range of motion, causing damage to the ligaments, bones, and other structures that stabilize the joint. This common and painful injury can happen suddenly from a fall, a direct blow in contact sports, or during weight-bearing activities. The elbow's complex biomechanical design relies on a precise balance of bony congruence and soft tissue tension; when that balance is disrupted by an excessive anterior or posterior force, the joint capsule and supporting ligaments are placed under extreme tensile stress. Without proper intervention, a seemingly simple hyperextension can lead to chronic joint laxity, accelerated cartilage wear, and long-term functional deficits.
Whether you're an athlete, have experienced an accidental fall, or are simply trying to understand your elbow pain, this comprehensive guide covers the symptoms, causes, effective treatments, and crucial prevention strategies for a hyperextended elbow. Understanding the intricate interplay between the skeletal framework, ligamentous restraints, and dynamic muscular stabilizers is essential for navigating recovery and returning to pain-free movement.
What is a Hyperextended Elbow?
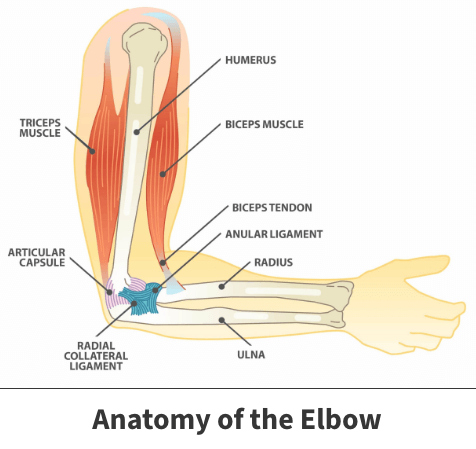
The elbow is a hinge joint where the upper arm bone (humerus) connects with the two forearm bones (radius and ulna). Ligaments, muscles, and tendons work together to allow the arm to bend and straighten within a specific range. A hyperextension injury happens when a force pushes the elbow beyond its limit, stretching or tearing these supportive tissues. This can range from a mild sprain to a severe dislocation or fracture.
To understand the injury fully, it is essential to recognize the specific anatomical structures involved. The elbow's stability is primarily maintained by three key ligament complexes: the medial (ulnar) collateral ligament (MCL/UCL), the lateral (radial) collateral ligament (LCL), and the annular ligament. During hyperextension, the anterior joint capsule is stretched, while the posterior compartment experiences compressive forces. If the force continues, the collateral ligaments are subjected to extreme valgus or varus stress, potentially leading to partial or complete tears. In adolescents and young adults, the bony growth plates (physes) around the elbow may be weaker than the ligaments, making them more susceptible to avulsion fractures where a tendon pulls a fragment of bone away from its attachment site.
Beyond the primary stabilizers, the elbow relies heavily on dynamic muscular control. The flexor-pronator mass and extensor-supinator muscles act as secondary restraints, absorbing shock and modulating joint loading during rapid movements. When a sudden hyperextension occurs, these muscles are often unable to contract quickly enough to counteract the external force, leaving the passive ligamentous structures to bear the brunt of the mechanical stress. Additionally, the synovial membrane lining the joint capsule can become inflamed, leading to effusion and increased intra-articular pressure, which further restricts mobility and triggers pain receptors. The elbow's natural carrying angle (cubitus valgus), typically ranging from 5 to 15 degrees, also influences the vector of force during hyperextension. An abnormal carrying angle can predispose individuals to uneven ligament strain, complicating both the injury mechanism and subsequent rehabilitation.
Clinicians typically classify hyperextension injuries into three grades based on structural damage:
- Grade I (Mild): The ligaments are microscopically stretched but remain intact. Patients experience mild pain and minimal loss of function. The joint remains stable, and full recovery usually occurs within two to four weeks.
- Grade II (Moderate): Partial tearing of the ligaments occurs. There is noticeable swelling, bruising, and a clear loss of range of motion. The joint may feel slightly unstable during certain movements, requiring four to six weeks of structured rehabilitation.
- Grade III (Severe): Complete ligamentous rupture, often accompanied by joint subluxation (partial dislocation), cartilage damage, or associated fractures. This grade typically involves significant instability, severe pain, and a prolonged recovery timeline that may span several months and occasionally require surgical reconstruction.
Recognizing the Symptoms: How Do You Know If You've Hyperextended Your Elbow?
The signs of a hyperextended elbow can vary depending on the severity of the injury, the individual's pain tolerance, and the exact mechanism of trauma. Understanding the progression and specific characteristics of these symptoms is critical for accurate self-assessment and timely intervention. Symptom presentation often evolves over the first 48 to 72 hours as the inflammatory cascade intensifies and secondary muscular guarding sets in.
Immediate Signs
According to orthopedic specialists, many people experience distinct signs at the moment of injury:
- A "popping" sound: This often indicates ligament damage or a sudden shift in joint alignment. While not always present, an audible pop frequently correlates with structural compromise of the collateral ligaments or joint capsule.
- Sudden, sharp pain: The pain is immediate and localized to the elbow. It typically radiates along the anterior or posterior aspect of the joint, depending on which structures absorbed the brunt of the hyperextension force.
Common Symptoms
Following the initial injury, you may notice:
- Swelling and Inflammation: Fluid builds up around the joint as part of the body's natural response to tissue damage. Hemarthrosis (bleeding into the joint space) can occur if small intra-articular vessels are torn, causing rapid and pronounced swelling.
- Stiffness: You may have difficulty bending or fully straightening your arm. The inflammatory cascade and muscle guarding create a protective barrier of tension around the joint, severely limiting functional mobility.
- Tenderness to the Touch: The area around the elbow may be painful when pressed. Palpation often reveals point tenderness over the medial or lateral epicondyles, indicating specific ligament involvement.
- Bruising or Redness: Discoloration can appear around the injured joint. Ecchymosis (bruising) may track down the forearm or up the upper arm due to gravity and the dispersion of extravasated blood from damaged capillaries.
- Weakness: A noticeable loss of strength in the affected arm, wrist, or hand. Pain inhibition and reflexive muscle relaxation often mask true muscle function initially, but genuine neuromuscular weakness can persist as swelling increases intra-articular pressure.
- Muscle Spasms: The biceps muscle may spasm, especially when trying to move the arm. The triceps may also contract involuntarily to splint the joint, creating a cycle of pain and restricted movement.
It is also common for patients to report a sensation of "tightness" or a feeling that the joint is physically blocked from achieving full flexion. This is frequently caused by a combination of joint effusion and reflexive inhibition of the flexor muscles, a protective neurological response designed to prevent further tissue stretching. Grip strength often diminishes significantly due to the interconnected neural pathways linking the wrist flexors to the elbow stabilizers. Additionally, referred pain patterns can sometimes cause discomfort to radiate into the distal biceps tendon or proximal forearm, mimicking tendinopathy or nerve irritation. Tracking the trajectory and character of these symptoms over the first week provides clinicians with valuable diagnostic clues.
Severe Symptoms
In more serious cases, symptoms can include:
- Visible Deformity: The elbow may look misshapen, which could signal a dislocation. Posterior dislocations are the most common and present with a prominent olecranon and a squared-off elbow contour.
- Numbness or Tingling: Sensations of numbness or tingling in the forearm or hand may indicate nerve compression or damage. The ulnar nerve runs through the cubital tunnel near the medial epicondyle, while the median nerve traverses anteriorly; both are vulnerable during hyperextension trauma.
- Instability: A feeling that the elbow joint is loose or could "give way." Mechanical instability suggests that the primary or secondary stabilizers have been compromised, increasing the risk of recurrent subluxations.
When to Seek Medical Attention: Is Your Elbow Injury Serious?
While some mild elbow sprains can be managed at home, certain symptoms are red flags that require immediate medical care to prevent long-term complications. Delaying professional evaluation for significant hyperextension injuries can lead to improper healing, malunion of fractures, or permanent joint contractures. Early intervention is particularly crucial for athletes, laborers, and pediatric patients, whose biomechanical demands or developmental status heighten the risk of irreversible structural damage.
Go to an emergency room or seek immediate medical attention if you experience:
- A visible deformity in the elbow or a bone penetrating the skin.
- Inability to move or straighten your arm.
- Severe, uncontrolled pain that does not respond to initial rest and positioning.
- Loss of feeling, numbness, or poor circulation in your hand and fingers. Check for capillary refill time; if pressing on a fingernail does not cause color to return within two seconds, vascular compromise is possible.
- Cold, pale, or bluish fingers distal to the injury site, suggesting arterial injury or compression.
Schedule an appointment with a doctor if:
- Pain and swelling do not improve after a few days of home care using the RICE method.
- The pain interferes with your daily activities or sleep.
- The joint feels unstable or loose.
- You hear persistent clicking, catching, or grinding during gentle movement, which may indicate loose bodies (osteochondral fragments) within the joint space.
Clinicians also monitor closely for signs of acute compartment syndrome, a rare but limb-threatening complication. This condition arises when severe swelling increases pressure within the fascial compartments of the forearm, compromising blood flow and nerve function. The classic "6 P's" (pain out of proportion to injury, pallor, paresthesia, paralysis, pulselessness, and poikilothermia) warrant immediate surgical evaluation and possible fasciotomy. Furthermore, pediatric patients require specialized attention due to the presence of open growth plates (physes), which can sustain subtle Salter-Harris fractures that may not be apparent on initial physical examination but can significantly impact limb growth if misdiagnosed.
Common Causes and Risk Factors
A hyperextended elbow is typically caused by a traumatic event. Common scenarios include:
- Falls: Falling onto an outstretched hand is a primary cause, as the full impact travels up the arm to the elbow. This mechanism, known as a FOOSH injury, places immense axial load and posteriorly directed force on the ulnohumeral joint.
- Contact Sports: Athletes in sports like football, wrestling, and boxing are at high risk from direct blows or awkward landings. Blocking maneuvers, grappling holds, and sudden arm checks can forcibly drive the elbow past its anatomical limit.
- Weight-Bearing Activities: Gymnasts, weightlifters, and yoga practitioners can be susceptible if they put excessive weight on their arms with locked elbows. The repetitive compressive forces in activities like handstands, vaulting, or heavy bench pressing can fatigue the dynamic stabilizers, leaving the passive ligaments to bear the load.
- Accidents: Car accidents or other high-impact events can force the joint beyond its normal limits. Dashboard injuries during frontal collisions or bracing against sudden deceleration frequently result in complex elbow trauma.
Certain demographic and physiological factors also elevate risk:
- Age-Related Degeneration: Older adults often experience decreased ligament elasticity and cartilage thinning, making the joint more susceptible to injury from lower-impact forces.
- Prior Elbow Injuries: A history of sprains, dislocations, or surgeries weakens the structural integrity of the joint, increasing the likelihood of recurrent hyperextension.
- Muscle Imbalances: Overdevelopment of the biceps without proportional triceps strength, or poor scapular stabilization, alters upper extremity biomechanics and shifts excessive stress to the elbow during overhead or pushing movements.
- Connective Tissue Disorders: Individuals with inherited conditions such as Ehlers-Danlos syndrome, Marfan syndrome, or benign joint hypermobility syndrome possess inherently lax collagen fibers. This genetic predisposition reduces the tensile strength of ligaments, making them prone to microtrauma and macroscopic failure under normal physiological loads.
- Occupational Repetition: Jobs requiring repetitive forceful pushing, pulling, or prolonged terminal extension (e.g., carpentry, plumbing, manufacturing assembly) can cause cumulative microtrauma to the anterior joint capsule. Over time, this chronic stress compromises tissue resilience and lowers the threshold for acute hyperextension injuries.
- Improper Ergonomics and Equipment Use: Incorrect workstation setup, particularly desk height and chair positioning, can force the elbow into sustained extended postures during keyboard use or tool manipulation. Similarly, using improperly fitted weightlifting belts or gripping bars that exceed natural hand span can alter kinetic chain mechanics, transferring excessive torque to the elbow joint.
Traumatic Injury vs. Congenital Hypermobility
It's important to distinguish between an acute hyperextension injury and having naturally "hypermobile" or "double-jointed" elbows. The clinical presentation, management strategies, and long-term prognosis differ significantly between acquired trauma and systemic connective tissue variants.
- Traumatic Injury: A one-time event that damages the joint structures. The tissue disruption is acute, and the body initiates a well-defined inflammatory and proliferative healing response.
- Congenital Hypermobility: A lifelong genetic condition where connective tissues are looser, allowing joints to move beyond the normal range without an initial injury. While not inherently painful, this condition can increase the risk of dislocations, sprains, and chronic pain. It is frequently associated with syndromes like Ehlers-Danlos or falls under the broader category of Hypermobility Spectrum Disorders (HSD).
| Feature | Traumatic Injury | Congenital Hypermobility |
|---|---|---|
| Onset | Sudden, due to a specific event (e.g., fall, impact). | Lifelong condition, often noticed in childhood. |
| Cause | External force damages ligaments, bones, or tendons. | Genetic predisposition affecting connective tissue laxity. |
| Primary Symptoms | Acute pain, popping sound, immediate swelling. | Generalized joint flexibility, potential for chronic pain. |
| Affected Area | Localized to the elbow. | Often affects multiple joints throughout the body. |
| Management | RICE protocol, immobilization, physical therapy, surgery. | Muscle strengthening, activity modification, pain management. |
Clinicians may use the Beighton Score to quantify generalized joint hypermobility, which evaluates bilateral fifth finger hyperextension, elbow hyperextension, knee hyperextension, thumb-to-forearm apposition, and the ability to place palms flat on the floor with knees straight. A score of 4 or higher out of 9 typically indicates generalized hypermobility, requiring a tailored rehabilitation approach that prioritizes proprioceptive training and dynamic stabilization over aggressive stretching. For hypermobile individuals, the therapeutic focus shifts from tissue healing (as seen in trauma) to neuromuscular re-education, teaching the central nervous system to maintain joint alignment through active muscular co-contraction rather than relying on passive ligamentous restraint.
Diagnosis: How Doctors Confirm a Hyperextended Elbow
A proper diagnosis is key to effective treatment. A doctor will typically:
- Conduct a Physical Examination: The doctor will assess your elbow for swelling, tenderness, and instability. They will also check your range of motion and the strength of your arm. Specific orthopedic maneuvers, such as the valgus and varus stress tests at 30 degrees of flexion, help isolate UCL and LCL integrity. The moving valgus stress test is highly sensitive for medial collateral ligament pathology, while checking for a positive posterolateral rotatory drawer test can reveal posterolateral corner injuries.
- Review Your Medical History: You'll be asked how the injury occurred to understand the mechanism of force. Details about the direction of impact, the surface involved, and immediate functional capacity post-injury provide critical diagnostic clues. The clinician will also inquire about occupational demands, athletic participation, and prior joint issues.
- Order Imaging Tests: To determine the extent of the damage, your doctor may order:
- X-rays: To check for fractures or dislocations of the bones. Standard views include anteroposterior (AP), lateral, and oblique projections. Radiographs can also reveal joint effusions through the presence of fat pad signs (sail sign on lateral view), which indicate intra-articular bleeding.
- MRI or CT Scans: To get detailed images of soft tissues like ligaments, tendons, and cartilage, which can reveal sprains or tears. CT is particularly valuable for mapping complex fracture patterns or identifying occult intra-articular loose bodies, while MRI excels at visualizing ligamentous disruptions, tendon avulsions, and bone marrow edema.
- Dynamic Ultrasound: Increasingly utilized in sports medicine, ultrasound allows real-time visualization of ligament integrity under stress and can assess tendon sliding dynamics during flexion and extension.
Advanced diagnostic protocols may also include diagnostic arthrocentesis (joint aspiration) to analyze synovial fluid for hemarthrosis or inflammatory markers, particularly when infection or crystal arthropathy is in the differential. Stress radiography, where controlled valgus/varus forces are applied during imaging, helps quantify joint gapping and ligamentous insufficiency with high precision. Electromyography (EMG) and nerve conduction studies may be ordered if persistent numbness or tingling suggests significant peripheral nerve injury, particularly ulnar neuropathy at the elbow.
Treatment and Recovery Pathway
Treatment for a hyperextended elbow is tailored to the severity of the injury. The goal is to reduce pain and swelling, restore movement, and prevent future injury. A phased, evidence-based approach ensures that biological healing aligns with mechanical loading, minimizing the risk of reinjury.
Immediate First Aid: The RICE Method
For the first 48-72 hours after the injury, follow the RICE protocol:
- Rest: Avoid any activity that causes pain or strains the elbow. Early aggressive loading disrupts the fragile fibrin clot and delays tissue remodeling.
- Ice: Apply an ice pack wrapped in a cloth for 15-20 minutes every few hours to reduce swelling and numb the pain. Cryotherapy induces vasoconstriction, decreasing metabolic demand and limiting secondary tissue hypoxia.
- Compression: Use an elastic bandage to wrap the elbow. It should be snug but not so tight that it causes numbness or increased pain. Proper compression mitigates interstitial fluid accumulation.
- Elevation: Keep your elbow propped up on pillows above the level of your heart to help decrease swelling. Gravitational drainage enhances venous return and lymphatic clearance of inflammatory mediators.
Modern sports medicine has also introduced the PEACE & LOVE protocol (Protect, Elevate, Avoid anti-inflammatories, Compress, Educate & Load, Optimism, Vascularization, Exercise) for the subacute phase, emphasizing early protected loading and psychological resilience over prolonged immobilization. Contrast hydrotherapy (alternating hot and cold water immersion) can be introduced after 72 hours to promote vasodilation and enhance metabolic waste removal, accelerating the transition from the inflammatory to proliferative healing phase.
Non-Surgical Treatments
Most cases are treated without surgery. Your doctor may recommend:
- Pain Relievers: Over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen (Advil, Motrin) or naproxen (Aleve) can help manage pain and inflammation. Acetaminophen is an alternative for patients who cannot tolerate NSAIDs. Topical diclofenac gel may also provide localized relief with minimal systemic absorption.
- Immobilization: A brace or sling may be used to keep the elbow stable and limit movement, allowing the tissues to heal. Hinged elbow braces are particularly effective as they permit controlled flexion and extension while blocking terminal hyperextension and valgus stress. Immobilization typically lasts 1-3 weeks, followed by gradual mobilization.
Rehabilitation and Physical Therapy
Once the initial pain and swelling subside, a physical therapist can guide you through exercises to:
- Restore Range of Motion: Gentle stretching exercises, such as wrist flexion and extension, help regain flexibility. Therapists utilize passive, active-assisted, and active range-of-motion exercises, often incorporating joint mobilizations to break down early scar tissue adhesions. Pendulum exercises and towel-assisted stretches are commonly introduced early.
- Strengthen Supporting Muscles: Strengthening the biceps, triceps, and forearm muscles provides better stability for the elbow joint. Isometric contractions are initiated first, progressing to isotonic exercises (curls, extensions) with light resistance bands, and eventually to eccentric loading programs which enhance tendon stiffness and load tolerance.
- Improve Stability: A therapist will ensure you can return to activities safely, with proper form and technique. Proprioceptive training using wobble boards, closed-chain weight-bearing drills, and neuromuscular re-education helps restore dynamic joint control. Sport-specific drills mimic the exact vectors of force encountered during the athlete's activity.
A structured rehabilitation program is typically divided into distinct phases. Phase I (Days 1-14) focuses on edema control, pain management, and protected range of motion within a pain-free arc. Phase II (Weeks 2-6) introduces progressive strengthening, emphasizing closed-chain kinetic exercises and scapular stabilization. Phase III (Weeks 6-12) incorporates plyometric training, advanced proprioceptive challenges, and gradual return to functional tasks. Each phase requires meeting specific clinical milestones, including full extension without pain, symmetrical grip strength, and normalized tissue tolerance to eccentric loads before progression.
Surgical Options
Surgery is reserved for severe injuries. According to WebMD, surgery may be necessary for complex fractures, completely torn ligaments or tendons, or significant joint instability that doesn't respond to conservative treatment. Procedures can range from minimally invasive arthroscopy to open surgery to repair damaged structures. Arthroscopic debridement can remove loose cartilage fragments and smooth damaged surfaces, while open ligament reconstruction (e.g., ulnar collateral ligament reconstruction using autologous palmaris longus or gracilis tendon grafts) restores static stability. Fracture fixation involves internal plates, screws, or percutaneous pinning to maintain anatomical alignment during bone union. Post-surgical rehabilitation is highly protocol-driven, often requiring extended immobilization followed by meticulous, graded mobilization to prevent arthrofibrosis while ensuring graft or fixation integrity.
Recovery Timeframe
Recovery time depends on the injury's severity:
- Mild Sprains: May resolve in a few weeks with home care. Functional return often occurs within 10-21 days.
- Moderate Injuries: Often require 3-4 weeks or more of rest and rehabilitation. Full return to unrestricted activity typically takes 6-8 weeks, pending clinical milestones.
- Severe Injuries/Surgery: Full recovery can take several months. Ligament reconstructions and intra-articular fracture repairs generally require 4-6 months of structured rehab before returning to high-demand sports or heavy labor.
Return-to-activity clearance is rarely time-based alone; it is criteria-driven. Clinicians assess for symmetrical range of motion, isokinetic strength ratios (flexor/extensor balance), absence of joint effusion, and successful completion of functional sport simulations. Psychological readiness, including confidence in joint stability during dynamic tasks, is equally critical to prevent premature reinjury and kinesiophobia.
Long-Term Outlook and Potential Complications
With proper treatment, most people fully recover from a hyperextended elbow. However, without adequate rehabilitation, or in cases of repeated injury, long-term complications can arise:
- Chronic Instability: The elbow may feel permanently loose or prone to re-injury. Capsular laxity or incompletely healed ligament fibers can lead to functional apprehension and recurrent subluxations during overhead or weight-bearing tasks.
- Long-Term Stiffness: A persistent loss of range of motion. Heterotopic ossification (abnormal bone formation in soft tissues) or extensive capsular contracture can permanently limit flexion or extension, particularly if immobilization was prolonged without guided mobilization.
- Chronic Pain: A dull ache or sharp pain that continues long after the injury has healed. Neuropathic pain may develop if the ulnar nerve was stretched or compressed during the initial trauma, requiring specialized desensitization therapy or surgical decompression.
- Osteoarthritis: Severe damage to the joint cartilage can increase the risk of developing arthritis later in life. Post-traumatic osteoarthritis occurs when altered joint mechanics and residual inflammation accelerate cartilage degradation, leading to pain, crepitus, and progressive functional decline over decades.
Psychological factors also play a significant role in long-term recovery. Fear of reinjury (kinesiophobia) can cause athletes to alter their movement patterns, inadvertently shifting stress to other joints or reducing performance output. Addressing these concerns through graded exposure, psychological counseling, and confidence-building rehab progressions is integral to optimal outcomes. Additionally, patients should monitor for delayed-onset complications such as myositis ossificans (heterotopic bone formation within the brachialis or biceps following trauma), which typically presents as a palpable, painful mass and progressive stiffness 3-4 weeks post-injury. Early recognition and modified loading strategies can often mitigate these complications without requiring aggressive surgical intervention. Regular follow-up assessments ensure that subtle biomechanical deviations are corrected before they manifest as chronic dysfunction or degenerative joint disease.
Prevention: Prophylactic Strategies to Protect Your Elbows
While accidents are unavoidable, you can take steps to reduce your risk of a hyperextended elbow, especially if you are an athlete or have hypermobile joints. Prevention is multifactorial, encompassing neuromuscular control, biomechanical optimization, and systemic tissue health.
- Warm-Up Properly: Always prepare your muscles and joints before exercise. A comprehensive warm-up increases synovial fluid viscosity, enhances neural conduction velocity, and primes the musculotendinous units for rapid force production. Dynamic movements like arm circles, light band pull-aparts, and scapular mobilizations are highly effective.
- Strengthen Surrounding Muscles: A consistent strengthening program for your arms and shoulders provides better joint support. Focusing on eccentric triceps training, biceps brachii hypertrophy, and forearm pronator/supinator endurance creates a robust muscular corset that absorbs impact forces before they reach passive stabilizers.
- Use Proper Form: Learn and use correct techniques during weightlifting and sports to avoid placing undue stress on your elbows. Under coaching supervision, ensure proper scapulohumeral rhythm during pressing movements and maintain neutral wrist alignment during grip-intensive exercises to prevent compensatory elbow valgus.
- Avoid "Locking" Your Elbows: When doing exercises like push-ups or lifting weights, maintain a slight bend in your elbow to keep the muscles engaged and protect the joint. Terminal locking transfers the entire load from contractile tissues to the joint capsule and articular cartilage, increasing hyperextension vulnerability.
- Wear Protective Gear: In contact sports, consider wearing elbow pads or a supportive brace. Modern prophylactic braces utilize polycentric hinges and compression sleeves that provide external proprioceptive feedback and limit end-range excursion without significantly impeding athletic performance.
- Optimize Nutrition and Hydration: Adequate protein intake, vitamin C, zinc, and omega-3 fatty acids support collagen synthesis and modulate systemic inflammation. Proper hydration maintains the viscoelastic properties of tendons and ligaments, keeping them resilient under sudden tensile loads.
- Implement Periodization: Avoid sudden spikes in training volume or intensity. Progressive overload allows connective tissues time to adapt structurally, significantly reducing the risk of acute ligamentous failure during high-demand activities.
- Ergonomic Optimization: Evaluate daily workstations to ensure keyboards, mice, and tools are positioned to keep the forearms parallel to the ground. Use supportive armrests to offload elbow stress during prolonged computer use. Incorporate micro-breaks every 30-45 minutes to reset posture, stretch shortened flexor tendons, and activate dormant scapular retractors.
- Neuromuscular Training: Incorporate proprioceptive drills such as medicine ball throws, resistance band deceleration exercises, and closed-chain weight shifts. These activities train the central nervous system to rapidly recruit stabilizing muscles upon unexpected perturbation, creating a reflexive protective response that can intercept hyperextension forces before they damage passive tissues.
References
- Medical News Today. (2018). Hyperextended elbow: Symptoms, treatment, and recovery.
- Florida Orthopaedic Institute. Hyperextended Elbow.
- WebMD. (2025). What to Know About a Hyperextended Elbow.
- Motion Orthopaedics. (2024). How to Treat a Hyperextended Elbow.
- Resurgens Orthopaedics. Hyperextended Elbow: Symptoms, Causes & Treatment.
Frequently Asked Questions
Can a hyperextended elbow heal on its own without medical treatment?
Mild Grade I hyperextension injuries often resolve independently with diligent home care, including rest, ice, compression, and protected activity modification. The ligaments undergo natural healing through inflammatory, proliferative, and remodeling phases. However, attempting to self-manage moderate or severe injuries without professional evaluation is risky. Undiagnosed fractures, cartilage defects, or complete ligament ruptures can lead to chronic instability, malunion, or early-onset osteoarthritis. Medical imaging and a clinical assessment ensure that conservative treatment is appropriate and that no structural damage requires surgical intervention.
How soon should I start physical therapy after hyperextending my elbow?
Physical therapy typically begins once the acute inflammatory phase subsides, usually within 5 to 7 days post-injury, depending on pain tolerance and tissue response. Early intervention focuses on pain modulation, edema management, and gentle passive range-of-motion exercises to prevent joint stiffness and capsular adhesions. As healing progresses into the subacute phase, therapists introduce active-assisted movements, isometric strengthening, and proprioceptive training. Starting rehabilitation too early with aggressive loading can disrupt healing, while delaying it excessively can result in permanent stiffness and muscle atrophy.
Is it safe to pop or crack my elbow after a hyperextension injury?
It is strongly advised against manipulating, forcing, or attempting to pop a recently hyperextended elbow. Cracking sounds during normal joint movement are often benign and caused by the rapid release of nitrogen gas bubbles within the synovial fluid (cavitation). However, post-traumatic manipulation can exacerbate ligament tears, displace healing tissues, or worsen underlying joint effusions. If your elbow produces painful clicking, catching, or locking, it may indicate intra-articular loose bodies, cartilage flaps, or tendon subluxation, all of which require diagnostic imaging and professional evaluation rather than self-manipulation.
What sleeping positions are best for recovering from this injury?
Sleep positioning significantly influences pain control and tissue healing. The optimal strategy is to keep the elbow elevated above heart level on a firm pillow stack to minimize overnight fluid accumulation. Avoid sleeping directly on the injured side, as prolonged pressure can compromise circulation and increase pain. Many patients find that sleeping supine with the arm resting comfortably against the torso, or in a semi-reclined position using a wedge pillow, reduces tension on the anterior joint capsule and ligamentous structures. Using a soft hinged brace set at 30-45 degrees of flexion overnight can prevent involuntary extension during sleep while allowing venous return.
Will a hyperextended elbow affect my long-term athletic performance?
With comprehensive rehabilitation and a gradual return-to-sport protocol, most athletes regain full pre-injury performance levels. The key is achieving objective clinical milestones: pain-free full range of motion, bilateral strength symmetry (within 90% of the uninjured side), and successful completion of sport-specific functional drills. Rushing back before neuromuscular control and tissue tolerance are restored significantly increases reinjury risk. Some athletes with chronic hypermobility may experience residual stiffness or mild apprehension during high-velocity overhead motions, but targeted eccentric training, biomechanical adjustments, and proper taping or bracing strategies typically allow for sustained elite-level participation without long-term performance deficits.
Can I return to work with a desk job immediately after a mild hyperextension?
Yes, individuals with sedentary, low-impact occupations can often return to desk work within a few days, provided the elbow is adequately supported and pain is managed. Ergonomic adjustments are crucial: position the keyboard and mouse close to the body to minimize reach, use a padded armrest to offload joint stress, and consider wearing a lightweight compression sleeve to enhance proprioception and limit end-range extension. However, if your role involves repetitive lifting, forceful pushing, or prolonged static postures, a modified duty period or short-term medical leave may be necessary to prevent symptom exacerbation. Always consult your healthcare provider before resuming work activities, particularly if your job requires heavy manual labor or repetitive upper-extremity strain.
Conclusion
A hyperextended elbow is a complex orthopedic injury that disrupts the delicate balance of bony alignment and soft tissue stability. While the initial presentation is often sudden and painful, the majority of cases respond exceptionally well to structured, phased management. Early recognition of symptoms, prompt medical evaluation, and adherence to evidence-based rehabilitation protocols are the cornerstones of optimal recovery. Distinguishing between simple sprains and more severe structural compromises ensures that treatment is appropriately scaled, preventing unnecessary complications like chronic instability or post-traumatic arthritis. By prioritizing proper biomechanics, progressive strengthening, and proactive joint protection strategies, individuals can not only heal fully but also build resilient upper extremities capable of withstanding future physical demands. Always consult a qualified healthcare provider or physical therapist for a personalized treatment plan tailored to your specific injury severity and functional goals. Long-term success hinges on patience, consistency, and a commitment to addressing both the physical and neurological components of joint rehabilitation, ultimately restoring not just movement, but confidence in the restored joint's capabilities.

About the author
Samuel Jones, MD, is a board-certified orthopedic surgeon specializing in joint replacement and orthopedic trauma. He is a team physician for a professional sports team and practices at a renowned orthopedic institute in Georgia.